Women’s College of Pharmacy, Peth, Vadgoan, Maharashtra
Antibiotic resistance emerges as a major threat globally. By persistent selection pressure, bacteria gain the ability to resist the effects of an antibiotic. Large numbers of infectious diseases such as pneumonia, tuberculosis, and sexually transmitted diseases are Becoming harder to treat as antibiotics lost their effectiveness. Imprudent use of antibiotics is the key driver to the advent and Dissemination of resistant bacterial strains. Worldwide, antibiotic resistance hampers our progress in healthcare, food production, And ultimately life expectancy. Patient’s incompliance, self-medication, over-the-counter availability of antibiotics, a wrong Prescription from unskilled practitioners, diagnostic uncertainty, antibiotics used as growth promoters in animals, and globalization Are some of the predominant factors responsible for antibiotic resistance. Efforts should be made to update and monitor antibiotic Resistance across healthcare, environmental, and agricultural sectors. Educational interventions, vaccine development, and advanced Diagnostic measures throw a ray of hope in the future to curtail the emergence of new bacterial resistance strains.
Ranging from treating several infections to using as prophylaxis for surgical procedures, the advent of antibiotics is a stupendous achievement the modern medicine has ever made. From 1930-1960, ‘the golden era’ of antibiotics has been witnessed. Unfortunately, the use of these ‘wonder drugs’ has been rapidly accompanied by the emergence and dissemination of multidrug-resistant bacteria (MDR) or ‘superbugs’. These bacteria, either by biochemical or physiological mechanisms acquire the potential to resist the effects of an antibiotic leading to antibiotic resistance. Antibiotic resistance is one of the biggest crises threatening the current world as it wreaks harm to the human, animal, and environmental health. Many public organizations across the globe have recounted the rapid emergence of resistant bacteria as a “crisis” or “nightmare scenario” that could have “catastrophic consequences.” In 2013, the Centers for Disease Control and Prevention (CDC) reported that the human race is now in the “post-antibiotic era” and in 2014, the World Health Organization (WHO) declared that the antibiotic resistance crisis is becoming dire.3 A recent update on bacterial genome sequences has shown that over 20,000 potential resistance genes (r genes) of nearly 400 different types are present; however, functional resistance determinants are too meager in number.1 With the occurrence of antibiotic resistance, efficacy in the treatment options has been declined to lead to an increase in mortality rates. A surge in annual death from 70,000 to 10 million could be expected by 2050 accounting for a total cost of 100 trillion United States dollars (US$) due to deadly infections never seen in over 80 years.4
“Antimicrobial resistance: no action today; no cure tomorrow” is the theme of World Health Day in the year 2011. European Centre for Disease Prevention and Control (ECDC) has recently warned about multidrug-resistance of the pathogens ‘Eskape’, an acronym including Enterococci, S.aureus, K.pneumonia, A.baumanii, P.aeruginosa and Enterobacteriaceae resistant to cephalosporins, quinolones, and carbapenems. Worldwide, the methicillin-resistant Staphylococcus aureus(MRSA) is the most serious cause of nosocomial infections resulting in prolonged hospitalization and increased social and economic costs. 5Failure in the rapid discovery of new potential antibiotics and the irrational use of antibiotics are the principal factors for the occurrence of antibiotic resistance. In 1955, Felix Marti-Ibanez stated that “Antibiotic therapy, if indiscriminately used, may turn out to be a medicinal flood that temporarily cleans and heals, but ultimately destroys life itself.” 6 Various fields of medicine including surgery, the care of premature infants, cancer chemotherapy, care of the critically ill, and organ transplantation will be undoubtedly hindered sans effective antibiotics.7
Imprudent use of antibiotics in animals (food, pets, aquatic) and humans, easy availability over-the-counter, globalization, poor hygiene, and release of nonmetabolized antibiotics into the environment through manure/feces are the major factors responsible for increased MDR infections in the community. 2 Microbes will always adapt in a stringent environment as it is evident from the United States recent national data which indicates that among bacteria isolated in ICU, 10% of Klebsiella spp., 20% of Pseudomonas aeroginosa, and 50% of Actinobacter baumannii strains are resistant to carbapenems.8 Neither we will ‘win a war’ against Microbes nor live without them. Furthermore, we must Change our ‘us versus them’ attitude against microbes to Preserve antibiotics for the future. 8 Antibiotic resistance is A big matter of concern as it develops in no time. 9
History
An American microbiologist Waksman and his co-worker Came up with the term “antibiotics”, to describe chemical Substances generated by microorganisms to alter the Growth of other microorganisms. 10 The discovery of penicillin by Sir Alexander Fleming in the year 1928 was a milestone in the modern-day antibiotics as they saved millions of lives. However, the first prescription of antibiotics to treat serious infections was made in 1940. The initial appearance of antibiotic-resistant strain was noticed during World War II which was four years post the fortunate discovery of penicillin. Unfortunately, shortly thereafter, penicillin resistance became a severe matter of concern and many of the advantages it had in the previous decade started to diminish. In retort, a new type of antibiotics known as beta-lactam was discovered, developed, and distributed to mitigate the threat. Nonetheless, in 1962 methicillin-resistant Staphylococcus aureus (MRSA) was discovered in the UK followed by the US in 1968. 3 Mutant strains of Mycobacterium tuberculosis resistant to therapeutic concentration were found to rise after the introduction of streptomycin in 1944 to cure tuberculosis.1A lot of these pathogens have evolved to become a multidrug-resistant form after antibiotic administration.

Figure 1: History of Antibiotic discovery and development of antibiotic resistance.
An increase in the discovery of antibacterial and antifungal antibiotics along with a new generation of semi-synthetic drugs made the people excited thinking that any sort of infection can be easily controlled using antibiotics. Nevertheless, the evolution of bacterial strains proved them wrong. Fleming warned about the resistance that pathogens might develop if used in minimal quantity or for a shorter period.9 They are almost unaffected by any known therapeutically useful antibiotics discovered in the past few decades, thus proving the restricted usage of wonder drugs.10
Global impact
The crisis due to antibiotic resistance is the result of how we have developed and consumed antibiotics since their discovery. 8 Annual deaths due to bacterial infections in US account about 100,000 with around 70% constituted by infections resistant to treatment developed by the protocol. Furthermore, MRSA leads to a death of 19,000 patients which is more than that due to emphysema, HIV/AIDS, Parkinson's disease and homicide combined and even cause seven million visits both at the doctor’s premises or emergency rooms. 5, 7 In Europe, more than 4 million patients are annually affected by heath related infections with an estimate of 147,000 deaths. Commonly found infections are pneumonia (19.4%), post-surgical (19.6%), UTI (19%), bloodstream (10.7%) and gastrointestinal infections (7.7%). 5 Antibiotic resistant infections foster an annual cost of around $21 billion to $34 billion to the US health care system and around 8 million additional hospital days. 7 Resistance to broad-spectrum antibiotics (Fluoroquinolones & Cephalosporins) used to treat various types of illness, is as high as 70% in India for certain bacteria such as E-coli, which commonly cause diseases such as pneumonia, UTI, and diarrhea. According to Washington and New Delhi – based Centre for Disease Dynamics, Economics & Policy, resistance to the carbapenems class of antibiotics (usually used for high-risk infections) is 56% in India for the bacteria K. pneumonia, one of the main causes of pneumonia and lung infection. When effective first-line or second-line treatment options become limited, health care professionals (HCP) may be forced to use more toxic and expensive antibiotics resulting in prolonged hospital stays, frequent doctor visits, longer recovery time, and higher incidence of long-term disability. Antibiotic resistant infections increase the duration of hospital stays by 6.4 to 12.7 days. The medical cost charged for an individual patient due to antibiotic resistant infection may range from $18,588 to $29,069. 3
Challenges
Over the last 25 years, a dramatic slowdown in antibiotic development has been noticed. Clinical trials are facing difficulties in evaluating the effectiveness of new antibiotics against resistant pathogens and for inserting a placebo group for ethical reasons. By the time when the antibiotics show maximum effectiveness, the bacteria have already become resistant to it. Regrettably, antibiotics provide a lower return on investments compared to other drugs such as antiretrovirals. The expenditure for developing an approved antibiotic is currently estimated at between 400-800 million $. Due to these reasons, various pharmaceutical companies have completely left this sector finding it as unprofitable. Thus, a clear decline in research and development of new antibiotics can be seen. 5 Despite surging antibiotic resistance, there are institutional flaws that contribute to the global lack of action. The first is a governance problem- inadequate effective coordination across various working sectors to address this challenge. The second is a compliance issue-though many actions have been promised by states only a few have been implemented. The third is a leadership problem- no strong desire to stop the inappropriate use of antimicrobials in humans and animals. The forth is a financing problem-inadequate resources to implement antimicrobial policies. 9
Mechanism
Most antibiotics are obtained from natural sources (mostly soil) and bacteria sharing the same ecological slot with these molecules have evolved certain mechanisms to overcome the harmful antibiotic effects.
There are two major strategies adopted by the bacteria to thrive in antibiotic presence:
Gene mutation
A group of bacterial cells from a susceptible population develop mutations in genes that enable them to resist the
Effects of an antibiotic.
The following mechanisms change the antibiotic action by a mutation that results in antibiotic resistance:
Modification of antibiotic targets
a) Chemical alterations of the antibiotic: Through the production of enzymes, chemical changes in the antibiotic molecules are introduced. Eg: Aminoglycoside modifying enzymes (AMEs) that covalently modify the hydroxyl or amino groups of the aminoglycoside molecule.
b) Destruction of the antibiotic molecule: Bacteria with the help of enzymes and proteins destroy the drug. Eg: Carbapenemases produced by Klebsiella pneumonia break down carbapenem drugs and other β lactam drugs.A decrease in the drug uptake: Most antibiotics have intracellular bacterial targets particularly with gram-negative bacteria which entail them to penetrate the outer or cytoplasmic membrane to exert their action. Thus, these membranes act as the first line of defense to selectively keep antibiotics from entering. Eg: vancomycin, a glycopeptide antibiotic, is not active against gram-negative organisms due to the inability to penetrate the outer membrane.
A decrease in the drug uptake: Most antibiotics have intracellular bacterial targets particularly with gram-negative bacteria which entail them to penetrate the outer or cytoplasmic membrane to exert their action. Thus, these membranes act as the first line of defense to selectively keep antibiotics from entering. Eg: vancomycin, a glycopeptide antibiotic, is not active against gram-negative organisms due to the inability to penetrate the outer membrane.
Activation of efflux mechanism: Bacteria use efflux pumps. To get rid of antibiotics that enter the cell. Eg: Pseudomonas aeroginosa use efflux pumps to prevent Several antibiotics such as fluoroquinolones, beta-lactams, Chloramphenicol, and trimethoprim from entering the cell.
Global cell adaptation: By evolution, bacteria have Developed intricate mechanisms to survive hostile Environments including the human body. Resistance to Daptomycin and vancomycin is an illustration of global cell Adaptive response.
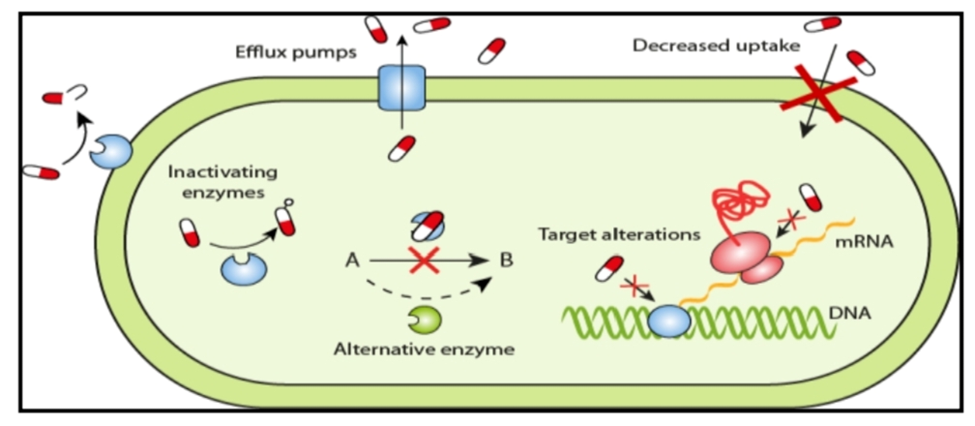
Figure 2: Mechanism of antibiotic resistance by gene Mutation.
Horizontal Gene Transfer (HGT): It is the process by which foreign DNA material is obtained either by transformation (incorporation of naked DNA), transduction (phage mediated), or conjugation (cell-to-cell contact). Mobile genetic elements (MGEs) such as plasmids and transposons act as vehicles to share valuable genetic information. 11, 12.
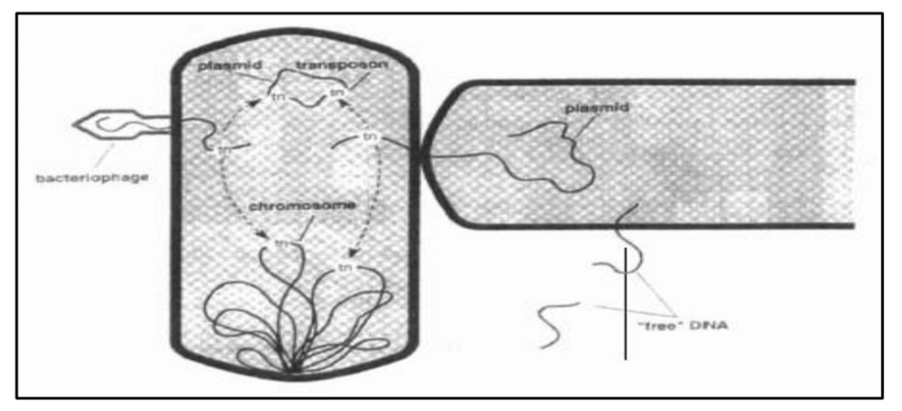
Figure 3: Mechanism of antibiotic resistance by horizontal gene transfer. 13
Causes
Antimicrobials were considered as “silver bullet” when introduced because of their ability to rapidly and specifically treat infectious diseases without causing harmful side effects upon the patient. The incredible effectiveness shown by the antibiotics led to their exuberant usage and generated a persistent belief among the general public that antimicrobials were invariably efficacious and enforced the people to use them for virtually all ailments. Further, over-the-counter (without medical prescription) availability of antibiotics in the developing world has even opened wider doors for antibiotic resistance. 9, 14 Failure in completing the full course of prescribed antibiotic treatment results in the development of resistance as those bacteria that remain untouched subsequently gain more strength against the antibiotics. 9
The empirical use of antimicrobials by clinicians is another root cause of their overuse. The practical limitations in rapidly and accurately diagnosing infectious disease, its causative pathogen, and most importantly, the susceptibility of the pathogen to a particular antimicrobial therapy leads to the random application of antibiotics. This may in turn necessitate frequent visits to clinicians and successive courses of different antimicrobials until an effective treatment is found. Moreover, under the pressure of requiring immediate action for a patient presenting with life-threatening symptoms, the clinician may advise for the simultaneous administration of different antimicrobials in the hope that one will be useful in controlling the unidentified pathogen.
This process subject’s the patient’s microbiota to an intense and repeated selective pressure that encourages the development of antimicrobial resistance (AMR). 14 Some studies have shown that treatment indication, choice of agent, or duration of antibiotic therapy is incorrect in 30% to 50% of cases. 3
Exorbitant use of antibiotics in farm animals has been observed over the past three decades especially in middle-income countries, where antibiotics are administered at low doses for prolonged periods for preventive and growth promotion purposes. In 2013, the US Center for Disease Control and Prevention estimated that around 66% of the global increase in antimicrobial consumption is accounted for by the growing number of animals raised for food production. 15 As per a recent report by the FDA (Food and Drug Administration), farm animals consume 13,000 tons of antibiotics yearly. Many studies have revealed that an exuberant use of antibiotics in livestock may lead to the development of food infections through antibiotic-resistant strains that pass from the GI tract of animals to humans who have eaten meat or dairy products. New multi-resistant bacterial strains such as Campylobacter, Salmonella, E. Coli, and MRSA have emerged with this inappropriate practice leading to their transmission to humans through contact with animals (mainly pig) or with the ingestion of contaminated food. [5] It is interesting to know that certain studies conducted in South America have shown that children who never treated with antibiotics have got food infections due to the consumption of chicken meat spoiled with antibiotic-resistant bacteria. 5
Diagnostic uncertainty is one of the underlying factors for drug misuse and overuse resulting in an increased number of resistant microbes. Due to the lack of accurate clinical or laboratory prediction methods and the risks associated with an untreated microbial infection, the empirical antimicrobial drug therapy is delayed especially for life-threatening infections. 6 Imprudent antibiotic use and rapid spread of resistant microbes are indirectly associated with an increase in immunocompromised patients, the growing life expectancy, and the susceptibility of older persons to infections. 6 Uncertain events such as the terrorist attack in Bali, the war in Iraq, and the tsunami in Southeast Asia have caused sudden outbreaks of deathly infections in other parts of the world by the transfer of patients infected with pan-resistant gram-ve bacteria such as Acinetobacter spp.
Global mixing, high population density, and less traveling time over the next two decades will accelerate the dissemination of numerous antimicrobial-resistant pathogens such as fluoroquinolone-resistant pneumococci and enteric microbes. 6 Online shopping of antibiotics has enabled widespread access to a therapeutically inferior, cheaper, and surplus amount of antibiotics. 11
Nowadays, an increasing number of people are reluctant to vaccinate due to unspecified reasons. In doing so, they are putting themselves into danger by creating increasing reservoirs of a pathogen within society that may later become antimicrobial resistant. 11 Strategy to preserve antibiotics for future use, we need to think distinctively and challenge long-standing assumptions.8
Many pieces of evidence recommend several molecular, immunologic, and microbial techniques that will change the way infectious diseases are diagnosed and lessen diagnostic uncertainty in the next two decades.6 Technological advances in diagnostics would enable prescribers to avoid dispensing antibiotics for viral infections and fevers of unknown origin. 16
Termination of antimicrobial drug therapy in patients who do not have a bacterial infection will reduce antimicrobial selection pressure without compromising patient safety. By reducing the duration of treatment with antimicrobial agents, great progress has been made over the last 5 years.6
National campaigns have been launched across several countries to educate physicians and patients about antibiotic misuse and the threat of resistance. These campaigns show positive results in changing attitudes and behavior among both the public and health care professionals. Through regular campaigns, a decrease in inappropriate patient requests for antimicrobial agents, and inappropriate antimicrobial prescription practices can be achieved. Subsequently, this may decline the dissemination of certain antimicrobial-resistant pathogens. 6 Shortly, modern vaccinology will help to decrease the transmission of antibiotic-resistant bacteria. The new pneumococcal conjugate vaccine has set an illustration for this expectation. Within the next 20 years, other vaccines to prevent invasive antibiotic-resistant infections will be launched to improve patient safety. Hand hygiene with alcohol-based hand rubs, early screening, and isolation of patients carrying resistant organisms appeared to decrease the transmission of resistant organisms.
A campaign organized by the World Health Organization in 2005 is promoting safety guidelines throughout the world. 6 The unnecessary use of antibiotics such as growth promoters in farm animals should be avoided. 17 In 2012, the FDA has established the Generating Antibiotics Incentives Now (GAIN) Act, which provides incentives for companies that invest in research and development of new antibiotics. 5 The Infectious Diseases Society of America (IDSA) has set forth the following recommendations:
The WHO has suggested that children in developing countries should use antibiotics only for the treatment of severe bloody diarrhea and cholera. 9 The existence of an antibiotic crisis and its impact on the future of the human race has stimulated various health care bodies such as the CDC and the WHO to recommend actions and programs to address the present crisis. Two main categories of activities suggested are those that address the prevention of disease so that the need for antibiotics will be reduced and those that provide new or more efficient treatments to augment the existing ones.
In short, these measures include disease prevention through the use of vector control, vaccination, public education, clinical education, and legislative action. 11Improving industrial systems for sanitation and decontaminating hospital sewage water will reduce the risks of environmental exposure. 18 Antimicrobial stewardship programs minimize the undesirable consequences of antimicrobial misuse. Preferably, stewardship programs include the following: 18
Antibiotic resistance breaker (ARB) is a recent strategy designed to tackle the increasing emergence of AMR. These are compounds that may or may not have direct antibacterial effects and can either be co-administered with or conjugated to failing antibiotics to boost their effectiveness. Modifying enzyme inhibitors, membrane permeabilized and efflux pump inhibitors are the major classes of ARBs currently under investigation.19 Nevertheless, intensive surveillance and screening efforts are necessary to curb the global spread of antibiotic resistance.
CONCLUSION
Antibiotics are on their verge of extinction in terms of safety and efficacy due to the emergence and existence of resistant bacterial strains. A rising trend in antibiotic use and misuse fostered antibiotic resistance which imposed tremendous impact on clinical, economic, and societal sectors across the world. For protecting our future generations from infectious diseases, we need to preserve the antibiotics without being attacked by resistant bacteria. Policies and guidelines for judicious antibiotics use should be framed along with strict monitoring of their use. Antibiotic stewardship programs should be undertaken to educate the healthcare professionals who serve as behavioral models to the citizens and patients. Thereby, the judicious use of antibiotics can be promoted. Pharmaceutical companies should be encouraged with incentives to promote the development and production of effective antibiotics. Unanimous efforts should be taken regionally, nationally, and globally to control the spread of virulent bacterial resistance.
REFERENCES

Sayali Karande, Review on Antibiotic Resistance, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 8, 2333-2342. https://doi.org/10.5281/zenodo.16926231
 10.5281/zenodo.16926231
10.5281/zenodo.16926231
