Department of Pharmaceutics, Rasiklal M Dhariwal Institute of Pharmaceutical Education and Research, Chinchwad, Pune.
The global rise in opioid overdose has created an urgent demand for rapid, targeted, and safer therapeutic interventions beyond conventional antidote administration. Self-destructing (self-immolative) nanocapsules have emerged as a promising advanced drug delivery platform capable of responding to specific biological or chemical triggers associated with opioid toxicity. These nanocarriers are designed to remain stable under normal physiological conditions and undergo controlled degradation upon exposure to predefined stimuli, leading to immediate release of encapsulated therapeutic agents such as opioid antagonists. This review critically discusses the concept, design principles, and mechanisms of self-immolative nanocapsules with emphasis on their application in opioid overdose management. Various fabrication approaches, including nanoprecipitation, interfacial polymerization, and layer-by-layer techniques are reviewed along with commonly used polymers and trigger mechanisms. The pharmacological advantages, safety considerations, and potential challenges related to scalability, toxicity, and regulatory approval are also analyzed. Overall, self-destructing nanocapsules represent a novel and intelligent drug delivery strategy with significant potential to improve the efficacy and responsiveness of opioid overdose treatment.
1.1 OPIOIDS
Opioids are a broad class of substances that include naturally occurring compounds obtained from the opium poppy (Papaver somniferum), as well as semi-synthetic and fully synthetic drugs that produce similar pharmacological effects.[1] These substances exert their actions by binding to specific opioid receptors- namely μ (mu), δ (delta), and κ (kappa)- which are widely distributed in the brain and peripheral tissues.[2] At the neuronal level, opioid receptors mainly produce inhibitory effects by decreasing neurotransmitter release at presynaptic sites and causing hyperpolarization of postsynaptic neurons.[3]
Although the terms opioid and opiate are often used interchangeably, they are not identical. The term opioid refers to all natural, semi-synthetic, and synthetic substances that interact with opioid receptors, whereas opiates specifically describe the naturally occurring alkaloids derived from the opium poppy, such as morphine and codeine.[4] Commonly used opioids include morphine, heroin, codeine, fentanyl, methadone, tramadol, and several related compounds.[5]
Opioids act on the central nervous system and other organs to produce morphine-like effects, most notably pain relief and sedation. However, these drugs can also depress respiratory function, and excessive use or overdose may result in life-threatening breathing difficulties or death. Due to these potent effects, opioids carry a high risk of dependence and misuse.[6]
Certain opioid medications, particularly methadone and buprenorphine, are widely used in maintenance therapy for the treatment of opioid dependence. These drugs help reduce withdrawal symptoms and cravings, thereby supporting long-term recovery.[7]
Globally, drug use remains a major public health concern. In 2021, approximately 296 million people aged 15-64 years used drugs at least once, with nearly 60 million individuals using opioids. Around 39.5 million people were estimated to be living with drug use disorders during the same year. While illicit heroin remains the most commonly used opioid among dependent individuals, the misuse of prescription opioids has been increasing steadily.[8]
Fig.1: Opium poppy (Papaver somniferum)
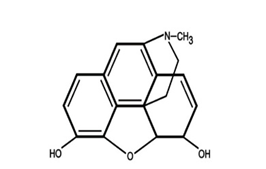
Fig.2: Structure of opium
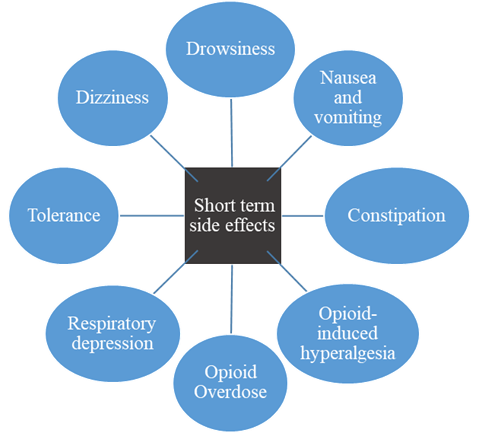
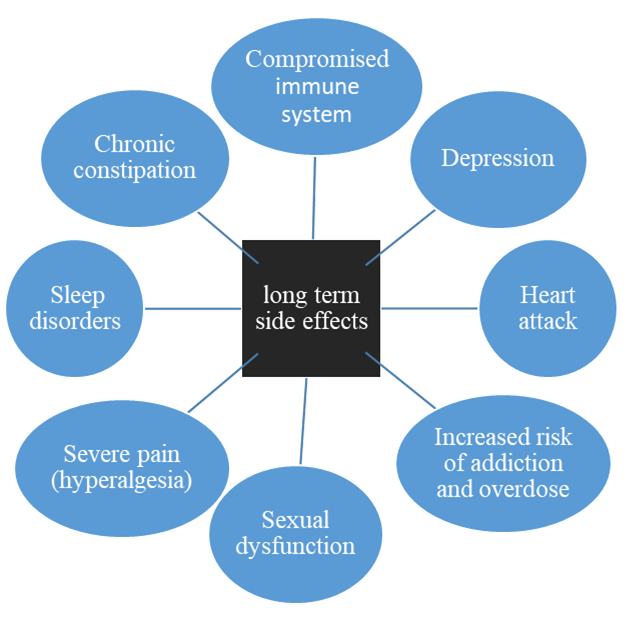
1.2 opioids side effects [2,5,9]
1.3 CLASSIFICATION OF OPIOIDS
1. Natural opium alkaloids: Morphine, Codeine [1,2]
2. Semisynthetic opiates: Diacetylmorphine (Heroin), Pholcodeine, Ethylmorphine. Many others like- Hydromorphone, Oxymorphone, Hydrocodone, Oxycodone are not used in India.[5]
3. Synthetic opioids: Pethidine (Meperidine), Fentanyl, Methadone, Dextropropoxyphene, Tramadol.[4]
1.4 Opioid receptor transducer mechanisms
All 3 types of opioid receptors (µ, κ, δ) have been cloned; all are GPCRs located mostly on prejunctional neurones. They generally exercise inhibitory modulation by decreasing release of the junctional transmitter. As such, various monoaminergic (NA, DA, 5-HT), GABA, glutamate (NMDA/AMPA) pathways are intricately involved in opioid actions. Opioid receptor activation reduces intracellular cAMP formation and opens K+ channels (mainly through µ and δ receptors) or suppresses voltage gated N type Ca2+ channels (mainly κ receptor). These actions result in neuronal hyperpolarization and reduced availability of intracellular Ca2+→decreased neurotransmitter release by cerebral, spinal, and myenteric neurones (e.g. glutamate from primary nociceptive afferents). However, other mechanisms and second messengers may also be involved, particularly in the long term.[1]
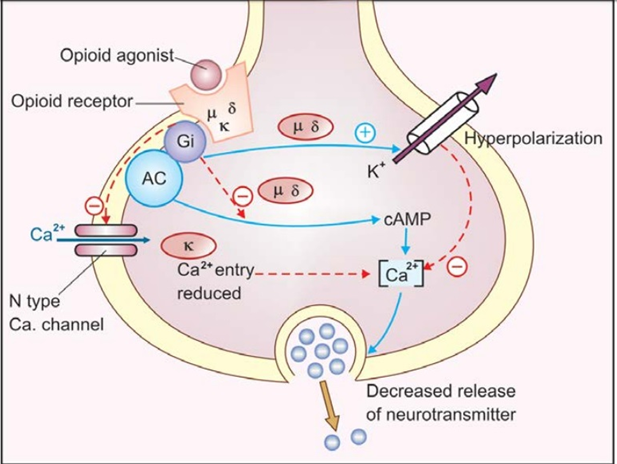
Fig.3: Mechanism of opioid
1.5 Opioid Misusage
Prescription opioids are usually safe for short-term pain management when taken exactly as prescribed by a doctor. However, misuse occurs when these medicines are taken in ways other than intended. This includes taking higher doses or using the drug more often than recommended, using opioids without a valid prescription, or taking medication that was prescribed for someone else. Some individuals misuse opioids not to relieve pain, but to experience feelings of relaxation or euphoria.
People may misuse prescription opioids by swallowing them as tablets or capsules, but others alter the medication to intensify its effects. This can involve crushing pills or opening capsules and dissolving the contents to inject into a vein, or inhaling the powdered drug through the nose. Such practices significantly increase the risk of addiction, overdose, and other serious health complications.[10]
1.6 Opioid Examples
|
Name of Drugs |
Structure |
|
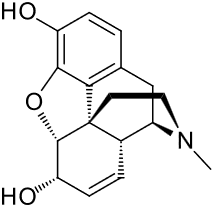
Morphine |
|
|
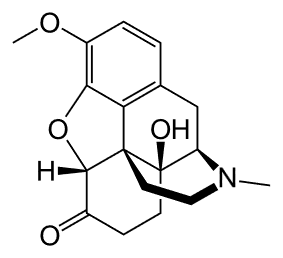
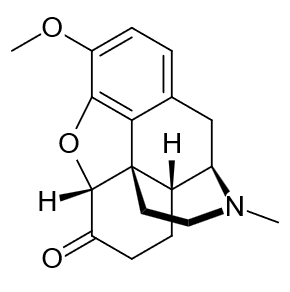
Oxycodone
|
|
|
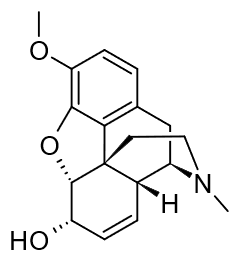
Codeine |
|
|
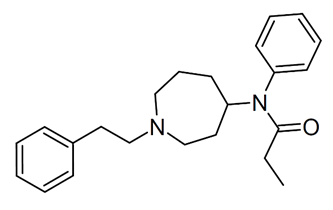
Fentanyl |
|
|
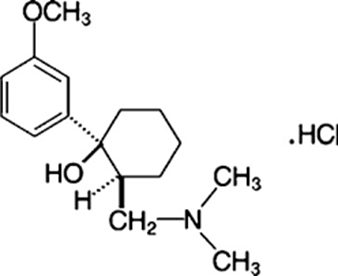
Tramadol |
|
|
Hydrocodone |
|
2. Opioid Overdose
An opioid overdose happens when the body is overwhelmed by opioids, either because too much was taken or because opioids were combined with other addictive substances such as alcohol or sedatives.[6] This risk exists with all opioids, whether they are prescribed medicines or obtained without a prescription. What may be a safe dose for one person can be dangerous for another, since tolerance levels and drug strength vary widely.[11] This makes it difficult to judge safe limits, especially when the exact dosage is unknown. For this reason, it is essential to use prescribed opioids exactly as directed and to avoid substances of uncertain strength. An opioid overdose is a serious, life-threatening condition that requires immediate medical attention.[12]
2.1 Risk Factors Associated with Opioid Overdose
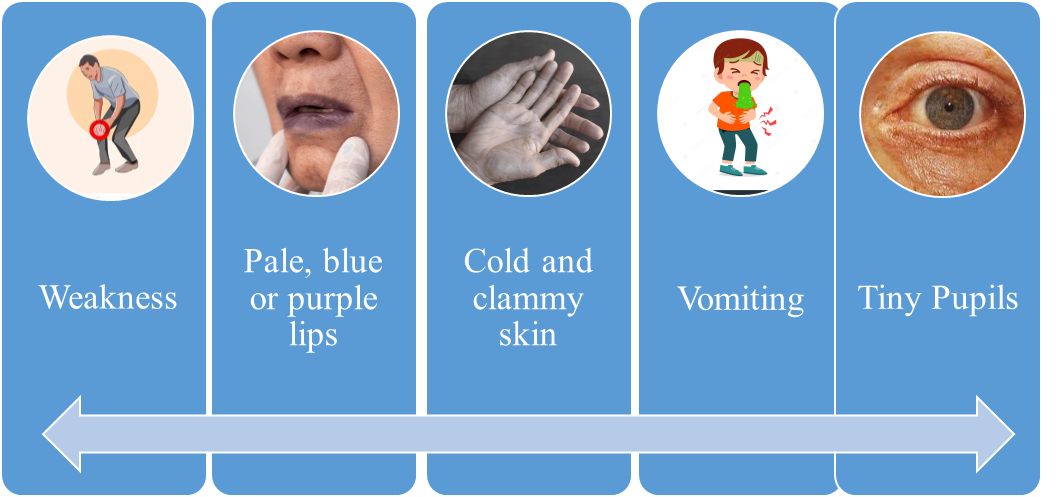
2.2 Signs and symptoms of an opioid overdose
2.3 Management of opioid overdose
Management of opioid overdose primarily focuses on supporting vital functions. Adequate respiratory support is essential, as positive-pressure ventilation not only improves oxygenation but also helps counteract the development of pulmonary edema. Blood pressure should be stabilized through the administration of intravenous fluids and, if required, vasoconstrictor agents.[6]
Gastric lavage using potassium permanganate may be carried out to eliminate any drug that has not yet been absorbed. This procedure can be beneficial even when morphine has been administered by injection, because morphine is a weakly basic compound. It tends to accumulate in the acidic environment of the stomach, where it becomes ionized and is unable to diffuse back into the systemic circulation, allowing removal through lavage.[1]
3. Naloxone
Naloxone is the specific antidote of choice for opioid overdose. It is administered intravenously in doses of 0.4-0.8 mg and can be repeated every 2-3 minutes until adequate respiration is restored. Naloxone acts rapidly, lacks intrinsic agonist activity, and does not independently depress respiratory function. However, because its duration of action is relatively short, repeated dosing at intervals of 1-4 hours may be necessary depending on the patient’s clinical response.[13]
Naloxone is a life-saving drug that reverses opioid overdose by blocking the receptors in the brain where opioids act. It works most strongly on the μ-opioid receptor, which is responsible for the main effects of opioids, including pain relief, euphoria, and dangerous slowing of breathing. Naloxone binds more tightly to this receptor than opioids do, allowing it to quickly push them off and reverse overdose symptoms.[14]
Although naloxone can also interact with κ (kappa) and σ (sigma) receptors, its action at these sites is much weaker. When used at low doses, naloxone primarily targets μ receptors, with minimal influence on δ (delta) and κ receptors. This selective action helps restore breathing and consciousness while limiting unnecessary effects on other opioid receptor systems.[15]
3.1 Mechanism of Action
Naloxone works by strongly competing with opioids for the μ-opioid receptor (MOR), the main receptor responsible for opioid effects.[1] It binds very tightly to this receptor, with high affinity, and reversing an overdose usually requires naloxone to occupy around half of the available MORs.[2] Because naloxone crosses the blood–brain barrier rapidly and attaches to and detaches from receptors very quickly, its effects are seen within minutes.[1,16] Unlike opioid drugs, naloxone does not activate the receptor or produce opioid-like effects of its own. Instead, it works by pushing opioids off the receptor, leading to a sudden loss of their effects. This explains why people often experience an abrupt improvement in breathing and consciousness after naloxone administration.[1]
Clinical studies, including those involving fentanyl exposure, show that naloxone’s success depends on several factors, such as the amount of opioid in the body, how long the opioid has been taken, and the dose of naloxone used.[17] Breathing problems can return once naloxone levels in the blood fall to low concentrations, indicating that its action is mainly governed by how quickly it is cleared from the body.[1,17]When naloxone is compared with longer-acting opioid blockers like alvimopan, the reason for its short duration becomes clear. Naloxone leaves the μ-opioid receptor very quickly-often within one to two minutes-whereas drugs such as alvimopan stay bound for much longer. Some opioids, including buprenorphine and fentanyl, also bind more tightly to the receptor than naloxone does.
Together, these differences in receptor binding explain why naloxone is highly effective for rapid overdose reversal, but why repeat doses or continuous infusion may be needed when long-acting or high-potency opioids are involved.[17,18]
3.2 Pharmacokinetics
Absorption:
Naloxone acts quickly, but the speed of its effect depends on how it is administered. When given intravenously (IV) or intraosseously (IO), its action can begin within about one minute.[1] Intranasal formulations are also fast-acting, with roughly 50% bioavailability, making them effective in emergency settings.[4] Most opioid overdoses show improvement within minutes of administration, although overdoses involving potent opioids such as fentanyl may require higher or repeated doses. If there is no response even after a total dose of 10 mg, it suggests that other substances such as alcohol, benzodiazepines, or stimulantsmay be contributing to the condition.[6]
Distribution:
Once in the body, naloxone is widely distributed and is capable of crossing the placenta. It shows minimal binding to plasma proteins, primarily albumin, which allows a larger fraction of the drug to remain active and available at receptor sites.[1,4]
Metabolism:
Naloxone is mainly broken down in the liver, where it undergoes glucuronidation, a common metabolic pathway that prepares the drug for elimination.[1,19]
Excretion:
The drug is cleared primarily through the kidneys, with approximately 25–40% excreted in the urine within the first 6 hours, and up to 70% eliminated within 72 hours. After intranasal administration, naloxone has a half-life of about 1.85–2.08 hours, which is slightly longer than the ~1.24-hour half-life observed following intramuscular injection.[19]
4.Nanoparticles
The term nano originates from the Greek word “nanos,” meaning dwarf or extremely small. In scientific terminology, it is used as a prefix to denote one billionth of a unit. Accordingly, a nanometer represents one billionth of a meter, equivalent to 10?? meters.[20]
Nanoparticles are solid, colloidal systems with sizes typically ranging from 1 to 1000 nanometers.[21] They are composed of macromolecular substances in which active pharmaceutical ingredients or other biologically active compounds may be dissolved, entrapped, encapsulated, or adsorbed within the particle structure.[22
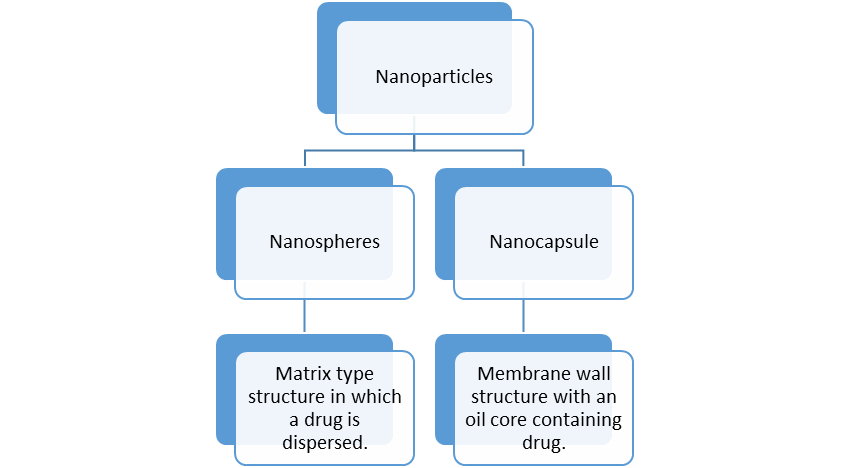
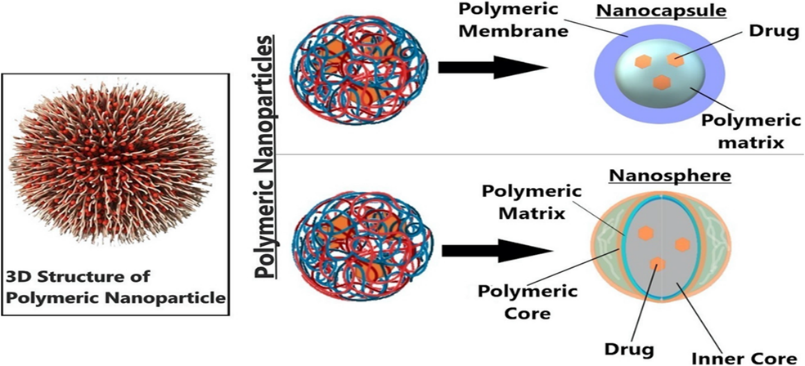
Fig.4: Types of nanoparticles
4.1 Nanocapsule
Nanotechnology, derived from the Greek term “nano” meaning extremely small, involves the manipulation and application of materials at the nanometer scale, typically ranging from 0.1 to 100 nm. Nanomaterials exhibit distinct physicochemical characteristics that have enabled their extensive use in biomedical, pharmaceutical, electronic, and molecular diagnostic applications. In drug delivery systems, these nanostructures generally comprise a solid or liquid core containing the therapeutic agent, which is enclosed within a polymeric membrane composed of either natural or synthetic polymers.[23] Such nano-based carriers have attracted considerable research interest due to their ability to protect drugs that are sensitive to oxidation or environmental degradation, thereby improving stability and facilitating controlled or delayed release of the active pharmaceutical ingredient.[24,22]
Two types of polymers can be employed in the manufacture of Nano capsules:
1) Polymers found in nature
2) Polymers that have been synthesised.
Nanocapsules have been created as drug delivery methods for a variety of medications via a variety of routes, including oral and parental administration. Drug toxicity should be reduced.
4.2 Composition of nanocapsule
Nanocapsules are submicroscopic colloidal drug delivery systems in which an aqueous or organic core is enclosed within a thin polymeric membrane.[22,23] This membrane may be composed of either natural or synthetic polymers, depending on the intended application.[22,24] The aqueous core typically contains water along with suitable surfactants, whereas the organic core consists of a solvent, polymer, oil, and the incorporated drug.[20,23]Nanocapsules are commonly prepared using techniques such as interfacial deposition of preformed polymers or interfacial polymerization of monomers.[21,24] During the formulation process, polymers carrying either positive or negative charges are sequentially introduced. Each newly deposited layer carries an opposite charge to the preceding one, leading to the formation of multilayered polyelectrolyte complexes. These alternating layers collectively form the capsule wall, which can consist of approximately 4 to 20 layers, depending on the desired thickness and functional properties.[25]
4.3 Mechanism of action of self immolative nanocapsule
1. Administration of Self-Immolative Nanocapsules
(Nanocapsules encapsulating an opioid antagonist such as naloxone)
↓
2. Systemic Circulation
Nanocapsules remain stable under normal physiological conditions (minimal premature drug leakage)
↓
3. Overdose Microenvironment Encounter
Elevated opioid concentration and/or specific physiological triggers (e.g., enzymatic activity, pH changes, redox conditions)
↓
4. Trigger-Induced Bond Cleavage
Trigger activates a sensitive linker in the nanocapsule shell
↓
5. Self-Immolative Depolymerization Cascade
Single cleavage initiates rapid, head-to-tail polymer breakdown
↓
6. Nanocapsule Shell Disintegration
Polymer converts into small, non-toxic molecular fragments
↓
7. Rapid Release of Opioid Antagonist
Naloxone (or similar antagonist) is liberated in a burst manner
↓
8. Competitive Binding at Opioid Receptors
Antagonist displaces opioids from μ-opioid receptors
↓
9. Reversal of Opioid Effects
Restoration of respiratory function and CNS activity [17,26,27]
4.4 Method of preparation
1) Nano-precipitation / Solvent Displacement Method
Nano-precipitation, also known as the solvent displacement method, is a simple and widely used technique for the preparation of polymeric nanocapsules. In this method, a pre-formed polymer is dissolved in a water-miscible organic solvent and then introduced into an aqueous phase, either with or without a stabilizing or wetting agent. Upon contact with the aqueous medium, the organic solvent rapidly diffuses, leading to the precipitation of the polymer and formation of nanocapsules.
When a small quantity of a non-toxic oil is incorporated into the organic phase, nanocapsules with an oil-filled core are formed. These oil-based central cavities significantly enhance drug loading, making the method particularly suitable for lipophilic drugs. Due to the miscibility of the organic solvent with water, this technique is less effective for the encapsulation of hydrophilic or water-soluble drugs.
The solvent displacement method has been successfully employed with several polymeric materials, including poly (lactic-co-glycolic acid) (PLGA), poly(lactic acid) (PLA), polycaprolactone (PCL), and poly(methyl vinyl ether-maleic anhydride) (PVM/MA). High entrapment efficiencies have been reported using this approach; for example, cyclosporine A-loaded nanocapsules achieved entrapment efficiencies as high as 98%. Additionally, this method has been utilized to develop highly loaded nanoparticulate systems based on amphiphilic β-cyclodextrins, facilitating the parenteral delivery of poorly water-soluble antifungal agents such as bifonazole and clotrimazole.[28,29]
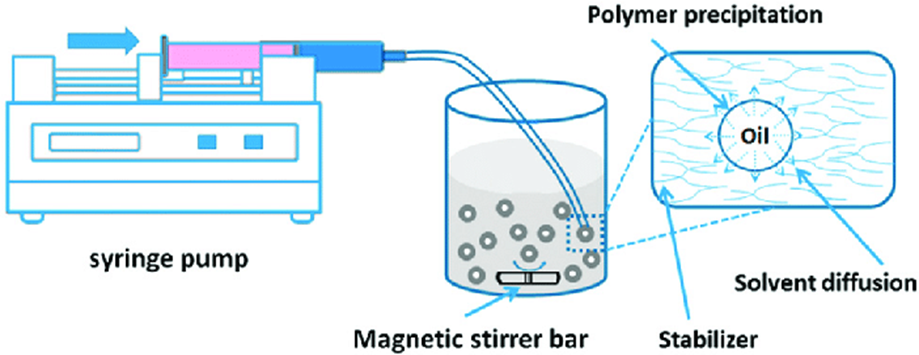
Fig.5: Nano-precipitation / solvent displacement method.
2) Layer-by-Layer (LbL) Technique
The layer-by-layer (LbL) technique is primarily employed for the preparation of colloidal particles and enables the formation of vesicular structures known as polyelectrolyte nanocapsules. This approach, first systematically developed by Sukhorukov and co-workers in 1998, allows precise control over the chemical composition and structural characteristics of the resulting capsules.
The formation of nanocapsules in this method is driven by strong electrostatic interactions between oppositely charged polyelectrolytes. At sufficiently high polyelectrolyte concentrations, irreversible adsorption occurs on the particle surface, leading to the sequential build-up of polymer layers. The process requires a colloidal template onto which a polymer layer is deposited either by immersing the template in a polymer solution followed by washing, or by reducing polymer solubility through the gradual addition of a miscible solvent.
This cycle is repeated with alternating polymers, resulting in the stepwise assembly of multiple layers. One of the major challenges associated with this technique is the formation of relatively large particles. However, this limitation has been addressed by applying ultrasonic treatment to aqueous suspensions, which reduces drug particle size to the nanoscale range (approximately 100–200 nm). Subsequent ultrasonic-assisted LbL coating stabilizes these particles in solution, allowing the formation of thin and uniform polyelectrolyte shells on their surfaces.
Although significant advancements have improved the efficiency of this method, the large number of deposition steps makes the process complex and time-consuming, especially when fabricating thick-walled polymeric nanocapsules.[30]
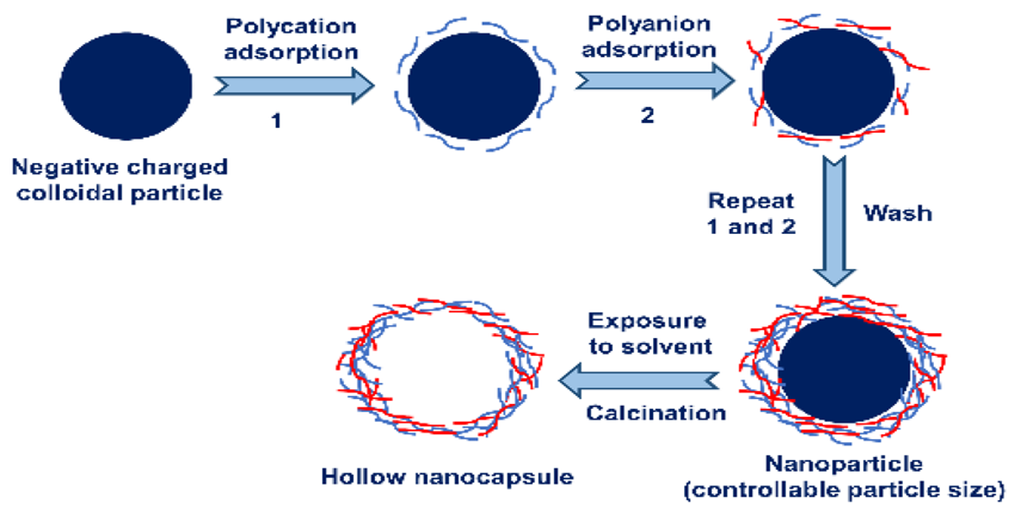
Fig.6: Layer-by-layer (LbL) technique.
3) Solvent Displacement / Interfacial Deposition Method
The solvent displacement method, also referred to as the interfacial deposition technique, is an alternative approach to conventional bulk polymerization, which typically requires elevated temperatures. This method is based on the interaction between two immiscible phases, where monomers present in one phase react at the interface with monomers or polymers in the second phase. Depending on reaction kinetics, polymerization may occur instantaneously or over a defined time period. Higher molecular weight polymers are often favoured due to the increased probability of monomer interaction with growing polymer chains.
Nanocapsules can be prepared using this method by forming a water-in-oil (W/O) emulsion, where the aqueous core may contain hydrophilic biomolecules such as oligonucleotides, and the polymer (e.g., isobutyl cyanoacrylate) is present in the organic phase. Following polymer formation at the interface, the resulting nanocapsules are purified by ultracentrifugation and re-dispersed in water to obtain a stable suspension of aqueous-core nanocapsules.
In this technique, both solvent (organic) and non-solvent (aqueous) phases are essential. The organic phase typically consists of solvents such as ethanol, acetone, or hexane, along with natural or synthetic polymers, the drug substance, and oils. The aqueous phase contains a non-solvent for the polymer, supplemented with one or more natural or synthetic surfactants to ensure colloidal stability. Generally, the solvent phase is organic, while the non-solvent phase is predominantly water.
Nanocapsules are formed as a colloidal dispersion when the organic phase is slowly introduced into the aqueous phase under continuous and moderate stirring. Among the biodegradable polymers commonly employed in this method, poly-ε-caprolactone (PCL) is one of the most frequently used materials due to its biocompatibility and controlled drug-release properties.[31]
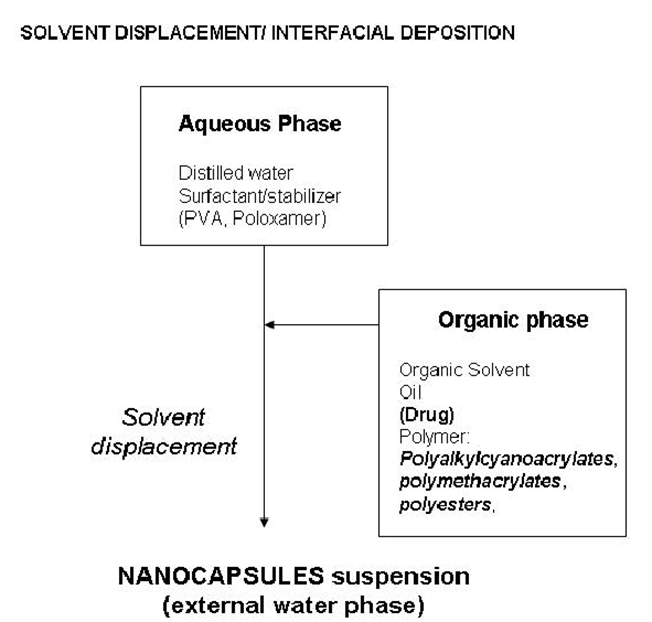
Fig.7: Solvent displacement / interfacial deposition method.
4) Phase Inversion Method
The phase inversion method is a technique used to develop silica nanocapsules through interfacial polymerization. First, a nano-emulsion is formed using the Phase Inversion Temperature (PIT) approach, which relies on a low-pressure homogenizer to create tiny droplets. In this process, decane acts as the oil phase and tetraethoxysilane (TESO) is dissolved in it, along with an ethoxylated alcohol that serves as the surfactant.
Once the nano-emulsion is prepared, TESO undergoes hydrolysis and polymerization to form the silica shell. This reaction is controlled by adjusting the environment with acidic (HCl) and basic (ammonia) conditions. The end product is a population of silica nanocapsules typically measuring 100–300 nm in size, each featuring a decane-filled core surrounded by a silica-based outer layer.
To understand the characteristics of these capsules, analytical tools such as dynamic light scattering (DLS), FTIR spectroscopy, high-resolution scanning electron microscopy (HR-SEM), and fluorescence studies (using an encapsulated chromic dye) are used. Additionally, after formation, the surface of these nanocapsules can be altered to carry either a positive or negative electrical charge, simply by introducing ionic surfactants that adsorb onto their surface.[29,31]
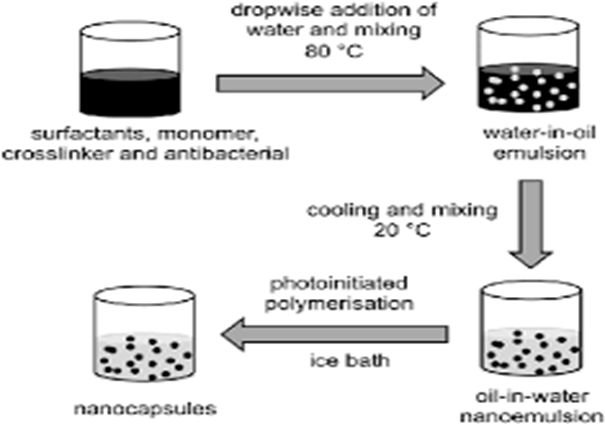
Fig.8: Phase inversion method.
4.5 Advantages and disadvantages of nanocapsule
|
ADVANTAGES |
DISADVANTAGES |
|
Nanocapsules provide sustained and controlled release of drugs. |
Nanocapsule formulations are very costly. |
|
They improve drug bioavailability and effectiveness. |
They often have low production yield. |
|
They reduce drug toxicity and side effects. |
Large-scale production is difficult. |
|
Due to their small size, they easily reach the target site. |
Technology transfer to industry is challenging. |
|
They can be administered by oral and parenteral routes. |
Dose adjustment after preparation is limited. |
|
Nanocapsules protect the drug from degradation by pH, light, and enzymes. |
Preparation requires highly advanced technology. |
|
They improve the stability of the drug. |
Skilled personnel are needed for manufacturing. |
|
They have high drug encapsulation efficiency. |
Stability is a major issue due to nano size. |
|
They allow better cellular and intracellular drug uptake. |
Recycling of materials is expensive. |
4.6 Applications of Nanocapsules:
1. Cancer Treatment:
Nanocapsules play an important role in modern cancer therapy by enabling targeted and controlled drug delivery. They are designed to deliver therapeutic agents such as proteins, anticancer drugs, or genes directly into cancer cells. For example, nanocapsules carrying the protein apoptin can selectively enter the nucleus of cancer cells and induce apoptosis (programmed cell death) without affecting normal healthy cells.
These nanocapsules are usually very small (around 100 nm), which allows them to easily penetrate tumors. In active targeting, ligands are attached to the surface of nanocapsules that specifically bind to receptors overexpressed on cancer cells. This improves drug accumulation at the diseased site, enhances therapeutic efficacy, and reduces systemic toxicity compared to conventional chemotherapy or gene therapy.
2. Food Applications:
In the food industry, nanocapsules are widely used to enhance food quality and stability. Nanoencapsulation helps protect sensitive food ingredients such as flavors, vitamins, antioxidants, and colorants from environmental factors like heat, oxygen, and light. Nanocapsules also improve texture, taste, and appearance of food products and allow controlled release of ingredients during consumption. Additionally, they increase the shelf life of food by preventing degradation and loss of nutritional value.
3. Nutraceuticals:
Nutraceuticals are bioactive food components that provide health benefits beyond basic nutrition, such as antioxidants, omega-3 fatty acids, vitamins, and herbal extracts. Many nutraceuticals have poor solubility and low bioavailability. Nanocapsules enhance their solubility, stability, and absorption in the gastrointestinal tract. Due to their small size, nanocarriers can easily enter the bloodstream, leading to improved therapeutic effectiveness. Natural and biodegradable materials such as lipids, collagen, gelatin, and albumin are commonly used to prepare nanocapsules, making them safe for oral consumption.
4. Ethyl Alcohol Absorption:
Recent research has demonstrated that digestive enzymes can be encapsulated inside non-toxic polymer-based nanocapsules. These enzyme-loaded nanocapsules are capable of absorbing or metabolizing ethyl alcohol from the bloodstream. In animal studies (mice), these nanocapsules significantly reduced blood alcohol levels. They act like artificial organelles, performing specific biochemical functions inside the body. This technology opens new possibilities for enzyme-based therapies, including potential treatments for alcohol intoxication and research applications in areas such as hair loss therapy.
5. Self-Healing Materials:
Nanocapsules are extensively used in self-healing materials such as polymer coatings, adhesives, composites, and microelectronics. These materials contain nanocapsules filled with healing agents. When cracks or damage occur, the nanocapsules rupture and release the healing substance, which fills the crack and restores the material’s integrity. Dicyclopentadiene (DCPD) is a commonly used healing agent. This technology increases the durability, reliability, and lifespan of materials by preventing further damage and reducing maintenance costs.
6. Targeted Drug Delivery:
Nanocapsules are specially designed carriers that help deliver drugs directly to the required site in the body, such as a specific organ or diseased cell. To achieve this, targeting molecules called ligands are attached to the surface of the nanocapsules. These ligands recognize and bind to receptors present on target cells. This approach ensures that most of the drug reaches the desired site, which improves treatment effectiveness and reduces unwanted side effects on healthy tissues.
7. Controlled and Sustained Drug Release:
Nanocapsules are capable of releasing drugs in a controlled and sustained manner over a longer period of time. Instead of releasing the entire dose at once, the drug is slowly released from the nanocapsule. This helps maintain steady drug levels in the body, reduces the need for frequent dosing, and improves patient compliance while providing better therapeutic results.
8. Gene and Protein Delivery:
Genes and proteins are highly sensitive molecules that can easily degrade inside the body. Nanocapsules act as protective carriers for DNA, RNA, and therapeutic proteins, shielding them from enzymatic breakdown. By improving stability and cellular uptake, nanocapsules enhance the effectiveness of gene therapy, protein therapy, and vaccination strategies.
9. Food Industry:
In the food industry, nanocapsules are used to protect and improve food ingredients. They help preserve flavors, colors, vitamins, and antioxidants by preventing their degradation due to light, oxygen, or heat. Nanoencapsulation also improves food texture and shelf life, resulting in better quality, more stable, and nutritious food products.
10. Enzyme Therapy:
Nanocapsules are used to enclose enzymes so that they remain stable and active within the body. Encapsulated enzymes can carry out specific biological reactions, such as helping in alcohol metabolism by lowering blood alcohol levels. These nanocapsules function like artificial cellular components and show promise in treating metabolic disorders and other enzyme-based conditions.
11. Cosmetics and Personal Care:
In cosmetic and personal care products, nanocapsules are used to carry active ingredients like vitamins, antioxidants, and skin-repair agents. Encapsulation improves the stability of these ingredients and allows them to penetrate deeper into the skin. Controlled release from nanocapsules enhances product effectiveness while reducing irritation and improving user safety.
12. Agriculture:
In agriculture, nanocapsules are applied for the controlled delivery of fertilizers, pesticides, and herbicides. This ensures that agrochemicals are released slowly and efficiently, reducing the amount required. Such controlled release helps lower environmental pollution, minimizes chemical runoff, and supports sustainable farming practices.[30,31,32]
CONCLUSION
Self-destructing nanocapsules represent an innovative advancement in the field of smart drug delivery systems, offering a targeted and stimulus-responsive approach for the management of opioid overdose. By exploiting self-immolative mechanisms, these nanocarriers enable rapid and controlled release of therapeutic agents precisely when pathological conditions arise, thereby minimizing systemic exposure and reducing adverse effects. The reviewed formulation strategies and material choices demonstrate the flexibility of this platform in achieving stability, sensitivity, and efficient drug loading. Despite their significant promise, challenges such as large-scale manufacturing, long-term biocompatibility, in vivo stability, and regulatory validation must be addressed before clinical translation. Continued interdisciplinary research integrating pharmaceutical nanotechnology, toxicology, and clinical pharmacology is essential to optimize these systems. In conclusion, self-destructing nanocapsules hold strong potential as next-generation interventions for opioid overdose, with the capability to enhance therapeutic outcomes and patient safety when appropriately developed and validated.
REFERENCES




Sayali Deth, Dinesh Choudhary, Suyog Kamble, Swapnil Balkunde, Suresh Choudhary, Self Immolative Nanocapsule for Opioid Overdose, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 3957-3972. https://doi.org/10.5281/zenodo.19338943
 10.5281/zenodo.19338943
10.5281/zenodo.19338943
