Professor, HOD Department of Pharmaceutics, NRI College of pharmacy, Pothavarappadu, Agiripalli, Eluru District.
Stem cell therapy has emerged as a transformative field in regenerative medicine, offering promising therapeutic applications for a wide range of diseases. Stem cells possess two unique properties: the ability to self-renew and the capacity to differentiate into specialized cell types, making them 44 invaluable for tissue repair and regeneration. Various types of stem cell therapies are under investigation or in practice, such as embryonic stem cells for tissue regeneration, adult stem cells for hematological and autoimmune conditions, mesenchymal stem cells for inflammatory and orthopedic disorders, and neural stem cells for neurological diseases. Clinical applications extend to cancer, cardiovascular diseases, diabetes, and bronchopulmonary dysplasia (BPD) in neonates. In BPD, stem cell therapy, particularly mesenchymal stem cells, demonstrates potential in reducing inflammation, promoting alveolarization, and supporting lung repair, although translation from animal models to clinical use remains limited. Preventive strategies for BPD also emphasize antenatal interventions, lung-protective ventilation, and neonatal intensive care practices. Despite substantial progress, challenges remain regarding long-term efficacy, safety, and standardization. Continued research into molecular mechanisms, optimal cell sources, and therapeutic delivery methods is vital to harness the full potential of stem cell therapy in modern medicine.
Two distinguishing features set stem cells apart from other cells. They are able to make more of their own cells. They renew themselves, that is. They also have the ability to differentiate into other cells that have different functions. Almost every tissue in the body contains stem cells. They are also required for tissue maintenance and after-injury repair. Stem cells differentiate into different types of tissues depending on their location. For example, bone marrow houses hematopoietic stem cells, which are able to make all the cells in the blood. Stem cells can also grow into many different types of cells, including bone, muscle, heart, or brain cells.

Figure-1: Stem cells
A variety of stem cells can be found, with the most flexible being embryonic stems that can form any cell in the developing fetus. The majority of body stem types are less capable of proliferation and may only assist in conserving and repairing tissues and organs where they exist. No other cell on its own can generate new cell types. [1]
Types Of Stem Cell Therapies:
During a stem cell transplant, healthy blood-forming stem cells are infused intravenously. The majority of blood-forming stem cells used in transplants are sourced from the bloodstream. When stem cells are derived from blood, the procedure may be referred to as a peripheral blood stem cell transplant, or PBSCT. However, blood stem cells can also be obtained from the bone marrow or from cord blood, which is collected at birth. The procedure may be called a bone marrow transplant, or BMT, when the stem cells are from bone marrow. Likewise, the procedure may be called a cord blood transplant when the stem cells come from cord blood. Mini-transplants represent a form of allogeneic transplant that is less intensive in its cancer treatment regimen as compared to a regular transplant. While a mini-transplant does not completely eliminate your blood-forming stem cells, it does eliminate some cancer cells. This variation of allogeneic transplant assists with immune suppression that can reduce the chances of rejection of stem cells from the donor. Tandem transplants are an autologous transplant. With a tandem transplant, you get a course of high-dose chemotherapy and a stem cell transplant. Then later on after numerous weeks or months, you go through another round of high-dose chemotherapy and another stem cell transplant.
Whether a stem cell transplant is right for you and which type you might have depends on many factors, such as:
Source: Derived from early-stage embryos (blastocyst stage)

Figure 2: Embryonic Stem cell (ESC)
Use: Regeneration of tissues (retina, spinal cord), potential for pluripotent- based therapy.
Ethical concern: Involves destruction of embryos.
Example: Clinical trials in macular degeneration.[2]

Figure 3: Adult Stem Cell (ASC)
Source: Found in tissues like bone marrow, fat, and blood.
Use: Treating blood cancers (e.g., leukemia), autoimmune diseases, orthopedic conditions.
Example: Hematopoietic stem cell transplantation (HSCT).[3]

Figure 4: Induced Pluripotent Stem Cell (IPSC)
Source: Reprogrammed adult cells (e.g., skin) to a pluripotent state.
Use: Disease modeling, drug testing, regenerative medicine.
Advantages: Avoids ethical concerns of ESCs.
Example: iPSCs used in Parkinson’s disease research.[4]
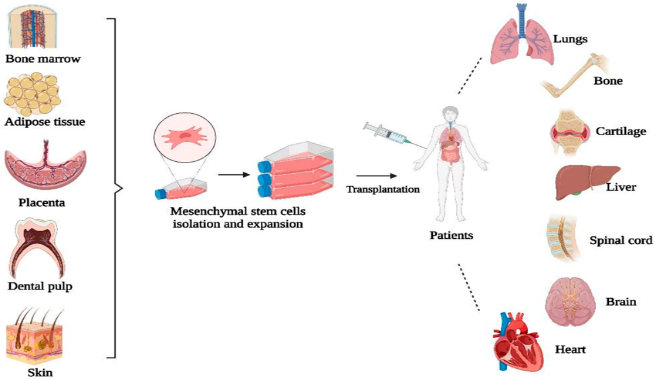
Figure 5: Mesenchymal Stem Cell (MSC)
Source: Bone marrow, umbilical cord, adipose tissue.
Use: Anti-inflammatory, immunomodulatory effects; used in arthritis, Crohn’s disease, and COVID-19.
Properties: Multipotent, easy to harvest and expand.[5]

Figure 6: Hematopoietic Stem Cell Therapy (HSCT)
Source: Bone marrow, peripheral blood, or umbilical cord blood.
Use: Primarily in blood disorders like leukemia, lymphoma, and anemia.
Procedure: Transplantation after chemotherapy or radiation.[6]
Source: Collected from umbilical cord at birth.

Figure 7: Umbilical Cord Blood Stem Cell Therapy
Use: Pediatric cancers, immune deficiencies.
Advantages: Lower risk of graft-versus-host disease.[7]

Figure 8: Neural Stem Cell
Source: Brain tissue or derived from pluripotent stem cells.
Use: Treatment of neurological diseases such as spinal cord injury, Parkinson’s, ALS.
Status: Mostly in experimental and clinical trial stages.[8]
Stem Cell Therapy Used in the Bronchopulmonary Dysplasia in Neonates:
The multifactorial condition known as bronchopulmonary dysplasia (BPD), or chronic lung disease (CLD) of prematurity, is typified by an inflammatory cascade that seriously damages the preterm lung and halts its normal development. Impaired lung function is one example of a clinical consequence that can last into adulthood. Numerous therapies have been employed to lower the risk of BPD, such as diuretics, steroids, coffee, and protective breathing techniques. Nonetheless, the condition is still very common in premature babies, impacting about 40% of those delivered before 28 weeks of pregnancy.[9] About 14.9 million infants are born at less than 37 weeks of gestation globally, constituting 11% of all neonates. Preterm birth is an increasingly emerging issue among infants. Complications related to early gestational age are the cause of an estimated half of all neonatal deaths. Technological and medical advances have also resulted in a dramatic increase in the survival rates of preterm infants. Such babies are at greater risk of various short-term and long-term complications, however. The oxygen and ventilatory needs of premature neonates with minimal to no pulmonary disease rise during the first few weeks of life. Several reasons such as acute lung injury (ALI) and respiratory distress syndrome (RDS) can cause respiratory failure in preterm infants.[10]

Figure 10: Stem Cell Therapy Used in the Bronchopulmonary Dysplasia in Neonates
Factors Influencing the Bronchopulmonary Dysplasia:
Factors affecting bronchopulmonary dysplasia (BPD) include prematurity, which causes lung immaturity, and postnatal factors like mechanical ventilation, high oxygen concentrations, infections, poor nutrition, and inflammation. Prenatal factors also play a role, including maternal smoking, lack of antenatal steroids, placental dysfunction from conditions like chorioamnionitis (inflammation of fetal membranes), and intrauterine growth restriction (IUGR).
Numerous studies have demonstrated that tobacco smoking during pregnancy affects respiratory function in children, including preterm infants and otherwise healthy infants. Animal studies have shown that tobacco compounds, especially nicotine, have a negative impact on lung development. Smoke exposure during pregnancy has been identified in a number of studies as a separate risk factor for the onset of BPD. Interestingly, a recent meta-analysis found that the relationship between maternal smoking and BPD can be affected by whether BPD is defined as oxygen requirement at different time points (postnatal day 28 vs. postmenstrual age 36 weeks). While some studies found no association with maternal smoking when BPD is defined as oxygen requirement at postnatal day 28, there was a significant association when BPD is defined as oxygen requirement at postmenstrual age 36 weeks.
Chorioamnionitis, infection of the placenta or fetal membranes, is a controversial cause of the development of BPD. In animal studies, chorioamnionitis has been found to stimulate lung maturation early on but then impede subsequent lung growth and result in BPD. Human studies have identified an association between BPD and chorioamnionitis. A recent meta-analysis of 158 studies concluded that mild to severe BPD is less likely to be caused by the nature of the disease, but chorioamnionitis is a major risk factor in all patients. In yet another prospective cohort study, the researchers found that the presence of chronic lung disease in infants who were born at less than 32 weeks' gestation was high, as evidenced by their chorioamnionitis and foetal inflammatory response syndrome. This was found to be significant. But the results can also be ambiguous. But there are diverging findings. A 25-year follow-up cohort study of VLBW children determined that chorioamnionitis was related to preterm delivery and neonatal sepsis, which were both compounded by BPD, not that chorioamnionitis is an independent risk factor for BPA.
Maternal hypertensive diseases may be responsible for triggering preterm delivery and intrauterine growth restriction (IUGR), which are both risk factors for BPD. PIH results from placental insufficiency, leading to the development of oxidative stress, diminished VEGFs, and abnormalities in the vasculature. These pathophysiological alterations may lead to BPD and may have an adverse effect on lung development. Even after much research, there is still no conclusive evidence to support this idea. Research on the relationship between BPD and PIH has yielded inconsistent results. A recent comprehensive study revealed that preterm infants born before 37 weeks did not have a significant inverse relationship between PIH and BPD. In contrast, a meta-analysis of 347,963 studies involving 327,919 newborns found that foetuses exposed to maternal hypertension and foetal growth restriction (FGR) had heightened susceptibility to BPD, but not so much to the same extent.
The risk of developing borderline personality disorder (BPD) is higher for preterm infants with foetal growth restriction (FGR) than for those who are appropriate for gestational age (AGA). Early impacts of FGR on lung development are believed to increase the risk of BPD in growth-restricted monozygotic twins. The impact of FGR on the development of the foetal lung has been further explored through preclinical studies using animal models of IUGR. Research indicates that BPD in FGR is connected to increased transforming growth factor beta, restricted surfactant protein genes, decreased pulmonary vascular and alveolar growth, exaggerated mitochondrial oxidative response, reduced VEGF receptor expression in the lungs (an aberrant state of PENDL), and altered function of phelial endothelial (lung).
Complex and poorly understood are the genetic variables that contribute to the development of BPD. Two separate twin studies have found a heritable factor in BPD, with monozygotic twins having higher rates than dizygotic siblings. However, this has not been completely confirmed. The identification of genes or genetic components that are positively associated with BPD is a matter of contention. The discovery of several potential genes associated with BPD has been made possible by recent approaches such as whole exome sequencing and genome-wide association studies. The genes that belong to these classes include matrix metalloproteinases, interleukins, tumour necrosis factor, VEGF, and Toll-like receptors. Also, as a matter of fact, research has shown that different biological processes may explain why BPD is heretical, depending on the severity of the disease. This emphasizes the intricacy of the genetic foundation of BPD and the necessity of additional study to fully comprehend the underlying processes.[11]

Figure 11: Pathophysiology of Bronchopulmonary Dysplasia
1. Arrested Lung Development:
Normally, alveolarization and pulmonary vascular growth occur rapidly in late gestation. In preterm infants, this process is interrupted, leading to fewer, larger alveoli (alveolar simplification) and impaired vascular growth (vascular dysmorphogenetic).
2. Mechanical Ventilation and Oxygen Toxicity
Positive pressure ventilation causes barotrauma and volutrauma, injuring delicate alveoli. Supplemental oxygen generates reactive oxygen species (ROS), leading to oxidative stress and damage to alveolar and endothelial cells.
3. Inflammation:
Prenatal factors (chorioamnionitis, intrauterine infections) and postnatal exposures (ventilation, oxygen, infections) trigger inflammatory cytokine release (IL-6, IL-8, TNF-α). Inflammation disrupts growth factor signalling necessary for normal lung development.
4. Vascular Abnormalities:
Impaired angiogenesis and endothelial injury cause pulmonary hypertension and abnormal vascular remodelling. This contributes to reduced oxygen exchange and chronic hypoxemia.
5. Extracellular Matrix Remodelling:
Increased fibroblast activity, collagen deposition, and elastin disorganization lead to stiff, fibrotic lungs.
6. Genetic and Epigenetic Susceptibility:
Genetic predispositions and epigenetic modifications influence individual risk for developing BPD.

Figure 12: Stem Cells for Treatment of BPD
A complete course of antenatal steroids before birth significantly reduces respiratory distress syndrome and the risk of death in preterm infants, though their direct impact on BPD incidence is debated due to increased survival rates.
The most effective method to prevent BPD is to prevent premature birth through measures like progesterone, smoking cessation, cervical cerclage, and changes in fertility practices.
This practice helps prevent anaemia and reduces the risk of intraventricular haemorrhage (IVH).
Avoid high pressures and large volumes during resuscitation and use positive pressure ventilation with a T-piece resuscitator.
Early use of non-invasive continuous positive airway pressure (CPAP) facilitates lung recruitment, builds functional residual capacity, and protects against lung injury by avoiding barotrauma from mechanical ventilation.
Utilize gentle ventilator strategies such as volume-targeted ventilation, high-frequency ventilation, short inspiratory times, and optimal Positive End-Expiratory Pressure (PEEP).
Administering exogenous surfactant is crucial, with developing minimally invasive surfactant administration (MISA) techniques being a promising advance.
Early initiation of caffeine (within the first 1-2 days) has shown promise in reducing the risk of BPD.
Restricting fluids and using high-calorie concentrated formulas can support growth while managing fluid intake, and early enteral feeding is also beneficial.
Treating very preterm infants colonized with Ureaplasma with azithromycin may reduce BPD risk, though further large-scale trials are needed.
Administering dexamethasone in the late phase (around weeks 2-7) may offer benefits for BPD prevention in at-risk infants, balancing efficacy with risks like sepsis.
Using pulse oximetry to guide oxygen therapy and maintain appropriate saturation goals is important for lung development.
CONCLUSION:
Stem cell therapy holds great promise in regenerative medicine, offering new treatment opportunities for conditions such as cancer, cardiovascular diseases, and bronchopulmonary dysplasia. While clinical trials show encouraging results, further research is essential to establish long-term safety and efficacy.
REFERENCES

Seelam Sowjanya*, Talasila Naga Yasaswini, Dr. Inturi Venkata Ramarao, Stem Cell Therapy Used in the Treatment of Bhronchopulmonary Dysplasia in Neonates, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 10, 2951-2963 https://doi.org/10.5281/zenodo.17461579
 10.5281/zenodo.17461579
10.5281/zenodo.17461579
