Ashokrao Mane College of Pharmacy, Peth Vadgaon
Cells are essential for treating diabetes because they can help damaged pancreatic tissue grow back and heal. In diabetes, particularly type 1, the insulin-producing ?-cells in the pancreas are destroyed, which makes it harder to control blood sugar levels. Stem cells can turn into working ? cells, which restores insulin production and keeps glucose levels stable. They also have immunomodulatory properties, which means they stop autoimmune attacks on new ?-cells. Because they can self-renew and provide a constant supply of healthy cells, they are a promising way to treat diseases. Stem cell-based therapies possess significant potential for the long-term management and potential cure of diabetes. It aims to bring attention to the most recent research, how stem cell-based therapies work, their pros and cons, and their future prospects for restoring pancreatic function and improving patient outcomes. This paper employs a literature review methodology, examining contemporary research on stem cell-based therapies for diabetes mellitus. A comparative analysis is performed to assess various stem cell types, including embryonic, mesenchymal, and induced pluripotent stem cells, regarding their efficacy, safety, and clinical potential. Experimental insights from preclinical and clinical trials are incorporated as necessary to evaluate therapeutic outcomes. The methodology focuses on recognizing contemporary progress, obstacles, and prospective trajectories in the translation of stem cell research into efficacious diabetes therapies. Stem cell therapies exhibit considerable potential in regenerating pancreatic ?-cells, reinstating insulin production, and enhancing glucose regulation in diabetes. Stem cell therapies exhibit considerable potential in regenerating pancreatic ?-cells, reinstating insulin production, and enhancing glucose regulation in diabetes. They also have effects on the immune system. However, there are several problems, including immune rejection, the potential for tumor formation, ethical concerns, and the fact that it doesn't work effectively in the real world. It is essential to get past these problems so that therapies can be used by a lot of people. Stem cell therapy has the potential to change how diabetes is treated. Future research will focus on safety, clinical translation, and long-term effectiveness.
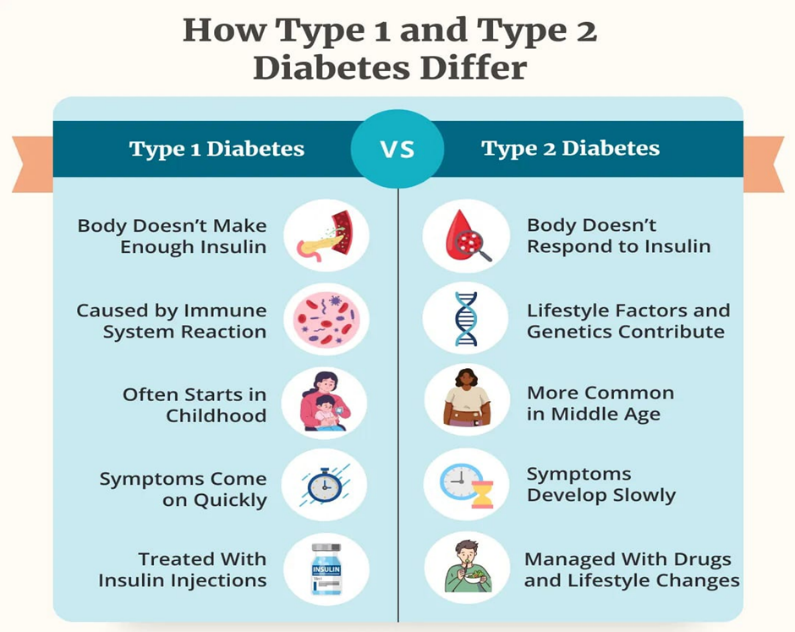
Diabetes mellitus is a long-term illness that makes it hard for the body to process blood sugar, or glucose, because of problems with insulin, a hormone that controls blood sugar levels. There are two main kinds: Type 1 diabetes and Type 2 diabetes. Type 1 diabetes is an autoimmune disorder characterized by the immune system erroneously targeting and obliterating the insulin-secreting beta cells in the pancreas, leading to minimal or absent insulin production. This kind usually starts in childhood or adolescence, but it can happen at any age and needs insulin therapy for the rest of your life. Some common signs are feeling thirsty all the time, needing to pee a lot, losing weight without trying, and being tired. Type 2 diabetes, on the other hand, is when the body doesn't respond well to insulin and makes less of it over time. It is more common in adults over 40, but because more people are becoming obese and not moving around much, it is now often seen in younger people, including kids and teens. People with Type 2 diabetes may not notice their symptoms at first because they are less severe and take longer to show up. Obesity, a bad diet, not enough exercise, a family history, and being of a certain race are all risk factors for Type 2. If not properly managed, both types of diabetes can cause serious long-term problems, such as heart disease, kidney damage (nephropathy), nerve damage (neuropathy), eye problems (retinopathy), and slow healing of wounds.[1] Management of diabetes focuses on maintaining blood sugar levels within a healthy range through a combination of medication (including insulin for Type 1 and sometimes for Type 2), regular physical activity, healthy eating, weight management, and routine monitoring. Education and support are also important components of diabetes care, helping individuals to understand their condition and make informed decisions. Early diagnosis, effective treatment, and lifestyle adjustments are critical in preventing complications and improving the quality of life for individuals with both Type 1 and Type 2 diabetes.
Conventional therapies for diabetes mellitus, including insulin therapy and oral hypoglycemic agents, have significantly improved disease management, but they also present several important limitations. Insulin therapy, essential for patients with Type 1 diabetes and some with advanced Type 2, mimics the body's natural insulin production. However, it cannot precisely replicate physiological insulin secretion, often leading to fluctuations in blood glucose levels. Patients are at risk of both hyperglycemia (high blood sugar) and hypoglycemia (low blood sugar), especially if insulin dosing is not accurately matched with food intake and physical activity. Additionally, the requirement for multiple daily injections or continuous infusion through insulin pumps can be invasive and burdensome, affecting quality of life and adherence to treatment.
In Type 2 diabetes, oral hypoglycemic agents such as metformin, sulfonylureas, DPP-4 inhibitors, and SGLT2 inhibitors are commonly used. While these drugs can be effective in lowering blood glucose, they also have limitations related to side effects, such as gastrointestinal discomfort (metformin), risk of hypoglycemia (sulfonylureas), or increased risk of urinary tract infections (SGLT2 inhibitors)[2]. Furthermore, many of these medications address symptoms rather than the underlying disease mechanisms, such as insulin resistance or beta-cell dysfunction. Over time, the effectiveness of oral agents may decline, leading to the need for combination therapy or transition to insulin.
Another key limitation of both insulin and oral therapies is that they do not prevent or reverse disease progression or the development of long-term complications. Neither therapy cures diabetes; they only manage its symptoms. This underlines the need for innovative therapeutic approaches such as beta-cell regeneration, immunomodulation, or gene therapy, which aim to address the root causes of diabetes rather than just control blood sugar levels.[3]
Regenerative medicine is an emerging field focused on repairing, replacing, or regenerating damaged tissues and organs to restore normal function. It combines biology, engineering, and clinical sciences to develop innovative therapies for chronic and degenerative diseases. One of the most promising tools in this field is stem cell therapy, which uses stem cells—undifferentiated cells capable of developing into various cell types—to promote healing and tissue regeneration. In diabetes research, stem cell therapy holds potential for restoring insulin-producing beta cells in the pancreas, offering hope for a long-term cure rather than merely managing symptoms through conventional treatments.
This paper aims to explore the scope, impact, and future potential of [insert topic], examining key trends, challenges, and opportunities. It seeks to provide a comprehensive understanding of the subject, contributing valuable insights for researchers, practitioners, and policymakers. The objective is to inform, analyze, and suggest practical recommendations.[4]
Pathophysiology of Diabetes Mellitus :
A class of long-term metabolic diseases known as diabetes mellitus (DM) is typified by persistently high blood sugar levels brought on by deficiencies in either insulin action or production, or both. Type 1 Diabetes Mellitus (T1DM), Type 2 Diabetes Mellitus (T2DM), gestational diabetes, and various particular kinds are the basic categories into which it is divided. Although each variety has a unique pathophysiological process, they all cause high blood glucose levels, which can harm different organs and tissues over time if left untreated. [5]
Normal Homeostasis of Glucose
The hormone insulin, which is released by the pancreatic beta cells in response to high blood glucose, strictly controls blood glucose levels in healthy individuals. Insulin prevents the liver from producing glucose and promotes the absorption of glucose by cells, particularly in muscle and adipose tissue. This equilibrium keeps blood glucose levels within a certain physiological range.
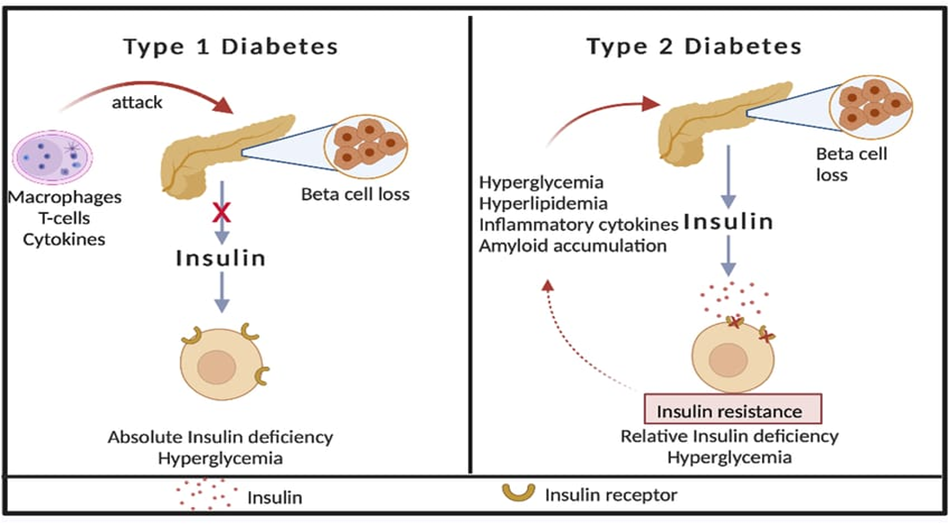
Diabetes Mellitus Type 1 (T1DM)
An autoimmune condition called type 1 diabetes causes the beta cells of the pancreas to be destroyed, which leaves the patient completely insulin-deficient.
Pathogenesis:
Autoimmune Destruction: Environmental causes, like as viral infections, can cause an autoimmune reaction in people who are genetically predisposed. Beta cells are gradually destroyed as a result of immune system attacks.
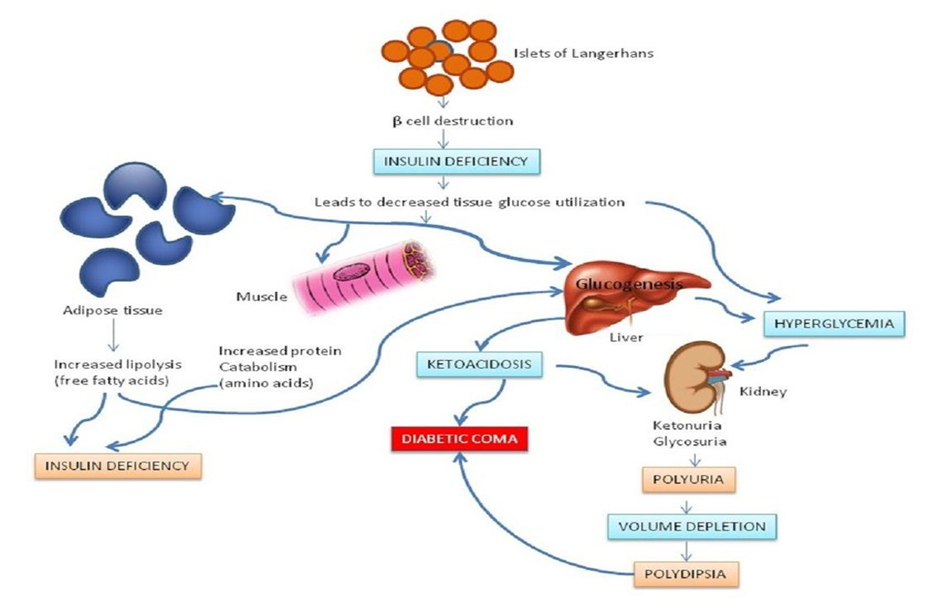
Loss of Insulin Secretion: Insulin synthesis decreases as beta cells are damaged. Hyperglycemia results from glucose building up in the bloodstream and being unable to enter cells in the absence of insulin.[6]
Metabolic Repercussions: Elevated free fatty acids are the result of increased lipolysis. Diabetic ketoacidosis (DKA) can result from the liver's process of ketogenesis, which produces ketone bodies (acetone, acetoacetate, and β-hydroxybutyrate).
When insulin's anabolic actions are absent, protein catabolism rises.
Clinical Characteristics:
Type 2 Diabetes Mellitus (T2DM) is a chronic metabolic condition characterized by insulin resistance and a relative insulin deficit. It accounts for around 90–95% of all diabetes occurrences globally and is closely connected with obesity, a sedentary lifestyle, and genetic susceptibility. The etiology of T2DM includes numerous linked pathways. Firstly, insulin resistance arises when peripheral tissues, notably muscle and adipose tissue, become less sensitive to insulin. This resistance compromises insulin receptor signaling—especially via the insulin receptor substrate (IRS) pathway—resulting in diminished glucose uptake in muscles and increased lipolysis in fat cells. The resultant free fatty acids further worsen insulin resistance. Secondly, beta-cell dysfunction occurs as the pancreas first adjusts by increasing insulin production. However, persistent demand leads to beta-cell depletion and death, with amyloid accumulation and oxidative stress leading to the loss of beta-cell function. Thirdly, hepatic gluconeogenesis remains unregulated, since the liver manufactures glucose despite high insulin levels, adding to fasting hyperglycemia. Additionally, the incretin effect is diminished; hormones such as GLP-1 and GIP, which usually promote insulin production after meals, are less effective in patients with T2DM. Another contributing aspect is enhanced renal glucose reabsorption, when the kidneys reabsorb excess glucose via SGLT2 transporters, maintaining high blood glucose levels.[7]
Clinically, T2DM typically has a gradual onset and may remain asymptomatic in its early stages. Common symptoms include polyuria, polydipsia, fatigue, blurred vision, and recurrent infections. Many patients are diagnosed only after complications such as neuropathy, nephropathy, or retinopathy have developed. In addition to T2DM, other forms of diabetes include Gestational Diabetes Mellitus (GDM), which arises during pregnancy due to placental hormone-induced insulin resistance. While GDM often resolves after childbirth, it significantly increases the mother's risk of developing T2DM later in life. Monogenic diabetes, such as Maturity Onset Diabetes of the Young (MODY), is caused by single-gene mutations affecting insulin secretion and is usually diagnosed in younger individuals. Secondary diabetes may result from other medical conditions, such as pancreatitis or Cushing’s syndrome, or from the use of certain medications like glucocorticoids.
Persistent hyperglycemia in diabetes leads to long-term complications that are broadly categorized as microvascular and macrovascular. Microvascular complications include retinopathy, which damages the retinal blood vessels and may cause blindness; nephropathy, which affects the kidneys and can lead to chronic kidney disease; and neuropathy, which results in pain, numbness, and autonomic dysfunction.[8] Macrovascular complications involve cardiovascular disease, significantly increasing the risk of heart attacks and strokes, and peripheral artery disease (PAD), which leads to poor wound healing and increases the risk of limb ischemia and amputation. These complications are driven by several underlying mechanisms, including the formation of advanced glycation end products (AGEs) that damage tissues, increased oxidative stress, and chronic inflammation that exacerbates endothelial dysfunction and accelerates vascular damage.
Stem Cells in Regenerative Medicine
Stem Cells in Medicine for Regeneration
Stem Cells:
What They Are and How to Classify Them
Stem cells are biological cells that have not yet become specialized. They have the amazing ability to become different types of cells in the body. These cells work as an internal repair system by dividing and renewing themselves over long periods of time while staying undifferentiated. Because they can turn into different types of cells, they are very important to regenerative medicine, which is the field that fixes or replaces damaged tissues and gets organs back to normal.[9]
What stem cells are like
Stem cells are different from other cells in the body in two important ways. The first is self-renewal, which means that a cell can divide many times without changing into another type of cell. The second thing is potency, which means the cell's ability to change into different types of cells. The potency level of a stem cell determines the types of cells or tissues it can make, which affects how it can be used in medicine.
Grouping of Stem Cells
There are two main ways to group stem cells: by potency and by where they come from.
1. Grouping by Potency
Potency is the stem cell's ability to change into different types of cells. Totipotent stem cells have the most options. They can turn into any type of cell in the body, including embryonic tissues (like the three germ layers) and extra-embryonic tissues (like the placenta). Totipotent cells include the zygote and early embryonic cells, which are cells that are still developing.[10]
Pluripotent stem cells can become almost any type of cell that comes from one of the three germ layers: ectoderm, mesoderm, or endoderm. But they cannot make tissues outside of the embryo. The most well-known example is embryonic stem cells (ESCs), which come from the blastocyst's inner cell mass.
Multipotent stem cells possess a restricted differentiation potential. They can make a limited number of cell types that are linked to a certain tissue or organ system. Hematopoietic stem cells (HSCs) in bone marrow can make different kinds of blood cells, but they cannot make other kinds of cells, like neurons or muscle cells.
Oligopotent stem cells can make a small number of cell types that are very similar to each other. For instance, lymphoid stem cells can turn into different kinds of lymphocytes, like B-cells and T-cells, but they cannot turn into cells that are not lymphocytes.[11]
Unipotent stem cells have the least ability to differentiate because they can only make one type of cell. But they still have the most important trait: they can renew themselves. Muscle stem cells (satellite cells), which only make muscle fibers, are a good example.
2. Grouping by Source
Stem cells can also be grouped by where they come from or what tissue they come from.
Embryonic stem cells (ESCs) are derived from the inner cell mass of the blastocyst, typically 4–5 days post-fertilization. They are pluripotent and highly valuable in research and therapy due to their broad differentiation capacity. However, their use raises significant ethical concerns since harvesting ESCs involves the destruction of embryos. [12]
Adult (somatic) stem cells are found in developed tissues such as bone marrow, brain, and skin. These cells are usually multipotent and function primarily in tissue maintenance and repair. Examples include mesenchymal stem cells (MSCs), which can give rise to bone, cartilage, and fat cells, and neural stem cells (NSCs), which differentiate into neurons and glial cells.
Induced pluripotent stem cells (iPSCs) are adult somatic cells that have been genetically reprogrammed to revert to a pluripotent state, mimicking the properties of embryonic stem cells. iPSCs are especially promising in regenerative medicine and disease modelling because they allow for the development of patient-specific therapies while bypassing ethical issues related to embryonic cells. [13]
Perinatal stem cells are found in perinatal tissues such as umbilical cord blood, amniotic fluid, and the placenta. These stem cells exhibit characteristics that bridge embryonic and adult stem cells, often being multipotent or, in some cases, even pluripotent. Due to their accessibility and lower ethical concerns, they represent a valuable source for therapeutic applications.
Stem Cell-Based Strategies in Diabetes
Diabetes mellitus (DM), particularly type 1 diabetes (T1DM), involves the destruction or dysfunction of insulin-producing pancreatic beta cells. Current therapies, including insulin injections and islet transplantation, have limitations such as immune rejection and donor shortages. Stem cell-based approaches offer a promising avenue for both beta-cell replacement and modulation of the diabetic microenvironment. This section outlines advances in stem cell biology as they pertain to diabetes, highlighting both therapeutic and regenerative strategies.
Stem Cell-Derived Beta-Cell Replacement
One of the most promising applications of stem cell research in diabetes therapy is the generation of functional insulin-producing beta cells from pluripotent stem cells, including embryonic stem cells (ESCs) and induced pluripotent stem cells (iPSCs).
Differentiation of Stem Cells into Insulin-Producing Cells
Advances in developmental biology have enabled the stepwise differentiation of stem cells into pancreatic progenitors and eventually into mature beta-like cells. Key transcription factors such as Pdx1, Nkx6.1, and NeuroD1 are sequentially activated during this process. producing cells that secrete insulin in a glucose-responsive manner, closely mimicking endogenous beta-cell function.
Companies like ViaCyte, Vertex Pharmaceuticals, and academic labs have developed scalable methods for generating these cells under acceptable manufacturing practices (GMP).
Transplantation Studies and Clinical Trials
Preclinical studies in diabetic animal models have shown that stem cell-derived beta-like cells can normalize blood glucose levels. Several early-phase clinical trials have now reached human subjects. For example, Vertex’s VX-880 program involves the infusion of stem cell-derived beta cells into patients with T1DM, showing initial success in restoring insulin independence.
However, challenges remain, such as immune rejection, risk of tumorigenicity, and ensuring long-term cell survival and function post-transplantation.
Islet Cell Regeneration
Beyond replacement, another frontier is to stimulate regeneration of native pancreatic islet cells or reprogram other cell types to take on beta-cell-like functions.
Reprogramming of Pancreatic Progenitor Cells
Researchers are investigating the potential to reawaken endogenous pancreatic progenitor cells, particularly those in the ducts or acinar compartments. Key strategies involve the manipulation of transcription factors (e.g., Ngn3, MafA) and signaling pathways (e.g., Notch inhibition) to coax these cells toward a beta-cell fate.
Use of iPSCs for Beta-Cell Replacement
The risk of immune rejection. iPSC-derived beta cells have demonstrated insulin production both in vitro and in vivo. Their autologous nature offers significant benefits but also presents manufacturing and cost-related challenges.
Additionally, gene-editing tools like CRISPR-Cas9 can be used to correct genetic defects in monogenic forms of diabetes (e.g., MODY) before iPSC differentiation.
Immunomodulatory Role of Stem Cells
In T1DM, autoimmune destruction of beta cells is the core pathology. Mesenchymal stem cells (MSCs) have gained attention not just for their regenerative potential but also for their immunomodulatory properties.
MSCs in Reducing Autoimmune Destruction
MSCs from bone marrow, adipose tissue, or umbilical cord can suppress autoreactive T cells, modulate dendritic cells, and promote the expansion of regulatory T cells (Tregs). Several studies have shown that co-transplantation of MSCs with beta cells improves graft survival.
Anti-inflammatory Cytokine Secretion
MSCs secrete a range of anti-inflammatory cytokines, such as IL-10, TGF-β, and PGE2, which help in creating a local immunosuppressive microenvironment. This property is being harnessed to delay the onset of T1DM in at-risk individuals and protect transplanted islets.
Recent studies also suggest that extracellular vesicles (EVs) derived from MSCs may carry similar immunoregulatory potential, offering a cell-free therapeutic strategy.
Stem Cells for Vascular Complications
Chronic hyperglycemia in diabetes leads to microvascular complications, including neuropathy, nephropathy, and retinopathy. Stem cells are being explored not just for glucose control but also for repairing damaged vasculature. [15]
Role in Treating Diabetic Neuropathy, Nephropathy, and Retinopathy
Diabetic Neuropathy: MSCs can promote nerve regeneration by releasing neurotrophic factors such as NGF and BDNF. Transplantation in diabetic models has shown improved nerve conduction velocity and reduced pain sensitivity.
Diabetic Nephropathy: Stem cells may reduce glomerular injury and fibrosis by modulating immune responses and promoting angiogenesis. Some preclinical studies show renal function preservation after MSC therapy.
Diabetic Retinopathy: Retinal damage due to capillary loss can be alleviated by endothelial progenitor cells (EPCs) and MSCs, which can home to ischemic retinal areas and restore vascular integrity. [16]
These therapies remain mostly in preclinical or early clinical trial phases, but they hold promise for tackling diabetes beyond glucose regulation.
Bioengineering & Tissue Scaffolds
To overcome challenges like immune rejection and graft failure, bioengineering approaches are being integrated with stem cell therapies.
Encapsulation Techniques for Immune Protection
Encapsulation involves enclosing beta cells in semi-permeable biomaterials, allowing nutrient and insulin exchange while blocking immune cells. Materials such as alginate hydrogels are commonly used.
Encapsulated stem cell-derived beta cells (e.g., ViaCyte’s PEC-Encap) are currently in clinical trials. However, fibrotic overgrowth and material biocompatibility remain major challenges. [17]
3D Bioprinting of Pancreatic Tissues
The use of 3D bioprinting has opened up avenues for recreating the complex architecture of the pancreas. Using stem cells embedded in bio-inks, researchers can fabricate islet-like structures with vascular networks, mimicking the in vivo environment more closely.
This technique enables the controlled spatial organization of different cell types—beta cells, endothelial cells, and immune-modulating cells—which could enhance cell survival and function post-transplant.
Current Clinical Trials & Case Studies
This section discusses key current and recent clinical trials of stem?cell (or cell?based) therapy in diabetes, noteworthy case studies (both triumphs and failures), and regulatory / approval challenges. [18]
Ongoing Global Trials Using Stem Cells for Diabetes
Vertex / ViaCyte - VX?880 (aka zimislecel)
This is an allogeneic stem cell-derived, completely differentiated islet cell treatment for Type 1 Diabetes (T1D) patients who have poor hypoglycemia awareness and severe hypoglycemic episodes.
The Phase 1/2 study commenced after the FDA authorized the IND in early 2021.
According to results reported in 2025 (FORWARD study), 12 participants showed restoration of endogenous insulin secretion (measured via C?peptide), elimination of severe hypoglycemia, achieving HbA1c targets (<7%), time in range >70%, and huge reduction in external insulin use (mean ~92%), with 10 out of 12 stopping exogenous insulin entirely. The experiment is proceeding into Phase 3, intending to recruit ~50 people.
GIOSTAR - DT2?SCT For Type 2 Diabetes (T2D), utilizing autologous mesenchymal stem cells. In November 2024, the FDA authorized the IND for a Phase 2 study.
The objective is to employ stem cells from the patients themselves to heal diabetes damage. Trial length projected to be 12?18 months.
AlloStem™ (Creative Medical Technology Holdings)
An allogeneic cellular treatment (from perinatal tissue-derived cells) for newly diagnosed Type 1 Diabetes. The FDA authorized an IND for the “CELZ?201” study in November 2022.
Throne Biotechnologies - Stem Cell?Educator Therapy
This is a form of hybrid immunomodulatory approach: patient immune cells are “educated” by cord blood?derived multipotent stem cells, then returned to the patient. Not stem cells replacing β cells per se, but meant to control autoimmune and restore β cell function.
In April 2024, their medicine acquired RMAT (Regenerative Medicine Advanced Therapy) classification from the FDA.
Other trials
A thorough assessment (until Sept 2024) revealed ~143 clinical studies in stem cell therapy for diabetes, spanning 31 countries.
The majority are Phase I?II; only a tiny minority have proceeded to Phase III or IV. Many are continuing, some have been finished, and several have been discontinued. [20]
Success Stories and Failures / Case Studies Successes:
FORWARD trial (VX?880 / zimislecel): As indicated above, the 12 patients in Phase 1/2 had outstanding results in terms of recovering insulin production, avoiding severe hypoglycemia, establishing glycemic control, and many obtaining insulin independence.
China / Peking University reprogrammed stem cells case: In a “world first”, a lady with T1D got ~1.5 million reprogrammed islet clusters generated from chemically reprogrammed pluripotent cells put into the abdominal muscle. Within 2.5 months, she started manufacturing enough insulin on her own and continued for almost a year. [21]
Limitations / Failures:
Many early studies, notably using MSCs, demonstrate improvements in glycemic indices but not complete insulin independence. Meta?analyses find moderate HbA1c reductions, but inconsistency in outcomes, short follow-ups, and variances in study design.
Safety problems in certain settings: For stem cell treatments requiring immunosuppression (e.g., islet infusions, ESC/PSC derivatives), hazards include infection, rejection, graft failure, and concerns regarding tumorigenicity or uncontrolled development. [22]
Regulatory hold/inertia: Not all promising medicines move to further stages, owing to manufacturing, scale, pricing, or safety barriers.
7.3 FDA Approvals & Regulatory Hurdles
Lantidra (donislecel): In June 2023, the U.S. FDA authorized Lantidra, the first allogeneic pancreatic islet cellular treatment for T1D. It is for adult patients who are unable to attain goal HbA1c due to frequent severe hypoglycemia.
Mechanism: infusion of donor islet cells into the hepatic portal vein; in some individuals, these donor cells generate enough insulin that external insulin injections/infusions are no longer necessary.
IND clearances: VX?880 gained FDA IND approval in 2021.
AlloStem got an IND from the FDA to commence a study in individuals with newly diagnosed T1D. [23]
GIOSTAR’s DT2?SCT also got IND for Phase 2 study in Type II diabetes.
Special designations: Thorne’s Stem Cell Educator treatment gained RMAT certification, which is aimed to fast?track regenerative therapeutics.
Regulatory barriers/ challenges: Immunosuppression / immunological rejection: Many cell replacement treatments involve life?long or long?term immunosuppressive regimens, which pose hazards and restrict usefulness. Also, immunological rejection remains a fundamental design difficulty (leading to encapsulation or immune?evasive engineering). [25]
Scaling/manufacturing: Producing stem cell-derived islets or beta?cells under GMP, in numbers suitable for general usage, with consistent quality, purity, and safety, is challenging and costly.
Safety & tumorigenicity: ESC/iPSC derivatives involve the danger of remaining undifferentiated cells or aberrant growth. Regulatory authorities demand thorough preclinical safety data.
Long-term efficacy: Many studies are early-stage, with brief follow-up. Durability of the treatment (how long transplanted or modified cells remain operating) is a critical concern.
Ethical / donor supply issues: For allogeneic donor islets (as in Lantidra), donor supply is restricted. For ESCs, ethical considerations in certain countries might hinder authorization or trials. [26]
Cost & access: Even with regulatory permission, cost may be exorbitant; likewise, necessity of immunosuppression, hospitalization, etc., may restrict real?world application.
SUMMARY & OUTLOOK
The area has made major recent advances: first FDA cell treatment approval (Lantidra), highly promising Phase 1/2 outcomes for stem?cell-derived islet therapies (VX?880), innovative case studies (reprogrammed islets into abdominal muscle), and immunomodulation techniques.
However, many medicines are still in early phases, with safety, immunological difficulties, cost, and long-term results being important impediments. [27]
Regulatory agencies are more supportive (INDs, RMAT, etc.), but widespread use will need achieving those safety and effectiveness standards, plus addressing manufacturing and health economics.
While stem cell-based therapies for diabetes hold transformative potential, several critical challenges remain that limit their widespread clinical use. These challenges span ethical, biological, immunological, and economic domains.
Ethical Concerns – Especially with Embryonic Stem Cells (ESCs)
The use of embryonic stem cells (ESCs), which are derived from early-stage embryos, has long raised ethical concerns, particularly in countries and cultures with strict views on the moral status of the embryo. Although ESCs have the advantage of unlimited proliferative capacity and pluripotency, their derivation involves the destruction of a human embryo, which some consider morally unacceptable. These concerns have led to legal restrictions or funding limitations in certain jurisdictions, affecting research progress and availability of ESC-derived therapies. In contrast, induced pluripotent stem cells (iPSCs) offer a more ethically acceptable alternative, as they are reprogrammed from adult somatic cells. However, iPSCs may still share some of the same biological risks as ESCs, such as tumorigenicity.[28]
Tumorigenicity and Genetic Instability
A major safety concern in stem cell-based therapy is tumorigenicity—the risk of stem cell-derived tissues forming tumors, particularly teratomas. This risk is highest when undifferentiated or partially differentiated cells remain in the final cell product. ESCs and iPSCs are inherently pluripotent, and without stringent purification and quality control, even small populations of residual undifferentiated cells can give rise to unwanted growths. Furthermore, during the reprogramming and expansion of iPSCs, genetic and epigenetic instability can occur, increasing the risk of mutations that may contribute to oncogenesis. Long-term safety data from clinical trials are still limited, making regulatory agencies cautious about approving stem cell-derived products for widespread use.[29]
Immune Rejection and Autoimmunity
In patients with Type 1 diabetes, where autoimmunity is the root cause of beta-cell destruction, introducing new insulin-producing cells—whether derived from stem cells or donors—faces two major immune barriers. First is allogeneic immune rejection, in which the host immune system attacks foreign cells. Second, and more uniquely to T1DM, is recurrence of autoimmunity, where the patient’s immune system may target newly introduced beta-like cells, even if they are autologous (from the patient’s own cells). To prevent rejection, some therapies require immunosuppression, which carries risks of infection and other complications. Newer approaches, such as immune-evasive cell engineering or encapsulation technologies, are under development but are not yet proven at scale.[30]
Cost and Large-Scale Application Barriers
The complexity of stem cell therapy development makes it cost-intensive. Manufacturing clinical-grade stem cell products requires strict adherence to Good Manufacturing Practice (GMP) standards, with extensive quality control, cell characterization, and batch-to-batch consistency. These processes are labor-intensive and expensive. Additionally, individualized therapies—such as autologous iPSC-derived treatments—pose further logistical and financial challenges, making them impractical for large populations. Even scalable allogeneic approaches, like those pursued by companies such as Vertex and ViaCyte, will face hurdles in reducing costs enough for broad access, especially in low- and middle-income settings. Reimbursement, regulatory delays, and high upfront investment may also limit commercial viability.[31]
FUTURE PERSPECTIVES
The area of stem cell-based therapeutics for diabetes is fast-growing, and numerous promising developments promise to push the limits of what’s presently achievable. From sophisticated genetic engineering methods like CRISPR-Cas9 to hybrid technologies like an artificial pancreas and highly specialized therapies via personalized regenerative medicine, the future of diabetes care may become more accurate, durable, and perhaps curative.
Genetic Engineering—CRISPR-Cas9 and Stem Cells
One of the most powerful tools in biomedical research today is CRISPR-Cas9, a gene-editing system that allows for precise change of DNA. In the context of diabetes, CRISPR is being utilized to increase the safety and functioning of stem cell-derived beta cells. For example, scientists may knock off genes important in immune recognition, rendering the cells “invisible” to the immune system and minimizing the need for immunosuppression following transplantation. [32]
Moreover, CRISPR may fix genetic abnormalities in patient-derived iPSCs before development into beta cells, making it especially beneficial for treating monogenic types of diabetes, such as MODY (Maturity Onset Diabetes of the Young). It also enables the insertion of safety switches, such as suicide genes, that may be triggered in the case of aberrant cell activity, minimizing the danger of cancer.
Although still in preclinical or early clinical phases, the combination of CRISPR with stem cell technology provides a next-generation method to generate safer, more immune-compatible, and possibly curative medicines. [33]
Artificial Pancreas Using Stem Cells
An intriguing field of research is the creation of a bioartificial pancreas, which combines stem cell-derived beta cells, biosensors, and microfluidic devices to duplicate the endocrine activities of the natural pancreas. [34]
These systems are being created to:
In essence, this would be a closed-loop, implanted device needing no external insulin injections or continuous glucose monitoring.[35] Startups and research teams are busy building prototypes, employing breakthroughs in biosensor technology, 3D bioprinting, and nanomaterials to make these devices biocompatible, responsive, and long-lasting. The incorporation of AI to handle real-time data from biosensors is also being researched to fine-tune insulin release algorithms. [36]
Though technical difficulties remain (e.g., oxygen supply, fibrosis, long-term sensor accuracy), the artificial pancreas offers a confluence of stem cell biology and biotechnology, possibly enabling a lasting and autonomous treatment.
Personalized Regenerative Medicine Approaches
As the knowledge of diabetes pathophysiology gets more detailed, there is increased interest in tailored regenerative therapy. This entails adapting stem cell-based therapy to an individual’s specific genetic, immunologic, and metabolic profile.[37]
For example:
Additionally, multi-omics methods (e.g., genomics, proteomics, and metabolomics) are being employed to improve patient classification and optimize medication timing and type, especially in the early stages of diabetes.
As these technologies evolve, stem cell-based treatment might change from a “one-size-fits-all” approach to a tailored, precision medicine paradigm.[39]
CONCLUSION
Stem cell-based therapeutics offer one of the most promising avenues in the treatment—and eventual cure—of diabetes. By facilitating the replacement of lost or malfunctioning beta cells, regulating the immune response, and repairing diabetes-related vascular damage, stem cells provide a multimodal treatment approach.[40] Clinical developments, such as stem cell-derived beta cell transplants and the creation of immunoprotective delivery methods, have demonstrated positive outcomes, including restoration of insulin independence and better glycemic control in early studies.
Moreover, integration with technologies like CRISPR-Cas9 and bioengineering platforms extends the potential of these treatments, opening the door for tailored and lasting remedies. Despite these developments, major obstacles remain, including immunological rejection, tumorigenicity hazards, ethical problems, and high costs associated with large-scale deployment. [41]
To fully achieve the therapeutic promise of stem cell treatment in diabetes, ongoing research, long-term clinical trials, and regulatory reform are necessary. Robust validation is essential to ensure safety, effectiveness, and accessibility across varied patient groups.[42]With continued scientific and clinical effort, stem cell-based medicines may soon transcend from experimental treatments to transformational solutions in diabetes management.[43]
REFERENCES

Dharati More, Samiksha Ghatage, Snehal Magdum, Rutika Chougule, Stem Cell-Based Therapeutic Strategies in Diabetes Mellitus, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 10, 189-204. https://doi.org/10.5281/zenodo.17244062
 10.5281/zenodo.17244062
10.5281/zenodo.17244062
