Department of Pharmacy Practice, N.E.T. Pharmacy College, Raichur, Karnataka, India
The advancement of digital health technologies has significantly transformed pharmaceutical care, contributing to the rapid adoption of telepharmacy. This cross-sectional study assessed the knowledge, attitude, and experience of registered pharmacists toward telepharmacy in North Karnataka, India. A total of 150 pharmacists participated using a structured and validated questionnaire comprising demographic details and 58 items across knowledge, attitude, and experience domains. Descriptive statistics and Spearman’s correlation tests were used for analysis. Overall, pharmacists demonstrated a high level of knowledge regarding telepharmacy, particularly the need for information and communication technology (96.7%), the use of video conferencing tools (95.3%), and digital health applications (93.3%). However, knowledge related to electronic prescribing of controlled substances was comparatively lower (narcotics 65.3%, psychotropics 58.7%). Attitudes were predominantly positive, with most participants agreeing that telepharmacy improves accessibility (84%), saves time (84.5%), and enhances communication with pharmacists (83.3%). Nevertheless, concerns remained regarding the confidentiality of patient data (72.2%). Experience levels were moderate, with telephonic counselling being the most common form (53.3%), followed by messaging applications (39.3%). Engagement via video conferencing and digital health apps remained limited (<30> 0.05), indicating that strong conceptual understanding and positive perceptions have not yet translated into routine practice. The study highlights the need for enhanced training, curriculum integration, and supportive regulatory frameworks to strengthen telepharmacy implementation in India.
The evolution of technology in healthcare services has transformed how patient care is delivered. In the field of pharmacy, this transformation is shaped by the concept of telepharmacy, which refers to the provision of pharmaceutical care when pharmacists and patients are not in the same location but interact through information and communication technologies. Telepharmacy services include drug selection, order review and distribution, patient counselling and monitoring, and the provision of clinical pharmacy services.¹?²
The National Association of Boards of Pharmacy defines telepharmacy as “the provision of pharmacological treatment to patients at a distance using information and communication technology.” While several studies report that hospital pharmacists demonstrate a high level of preparedness for telepharmacy, pharmacy students often show limited awareness and practical understanding. This highlights the need to evaluate students’ knowledge, attitudes, and readiness toward telepharmacy and to integrate structured training through simulations and experiential learning to enhance future pharmacy practice.³????
However, traditional pharmacy education has not yet fully incorporated the competencies required for effective telepharmacy service delivery. Consequently, students and pharmacists may experience difficulty adapting face-to-face communication skills to digital environments that require different interaction techniques and technological proficiency. Evidence suggests that in the absence of formal telepharmacy training, students perform better in conventional consultations than in telepharmacy-based interactions, contributing to the low adoption of telepharmacy in many countries, particularly in low- and middle-income settings even prior to the COVID-19 pandemic.?
Telepharmacy offers a patient-centered approach by enabling personalized counselling, medication adherence assessment, and comprehensive medication review.? Assessing pharmacy students’ preparedness and identifying existing educational gaps are therefore essential to strengthen telepharmacy education and support the effective implementation of telepharmacy services in contemporary healthcare systems.
MATERIALS AND METHODS
STUDY DESIGN: A questionnaire-based cross-sectional study was conducted to assess the knowledge, attitude, and experience regarding telepharmacy among registered pharmacists. The target population included registered pharmacists across North Karnataka. A total of 150 registered pharmacists were selected as participants for the study. The study was conducted over a period of six months, from January 2025 to June 2025.
Study Tool:
The instrument used in the study is structured and validated questionnaire. The questionnaire comprised a total of 58 questions, categorised into 4 demographic questions, 15 knowledge questions, 13 attitude questions, and 26 experience questions. Section A is about the demographic data of the pharmacy students; Section B is about knowledge regarding telepharmacy; Section C is about attitude based questions and Section D is about experience based questions on telepharmacy. Respondents could choose between “true” and “false” for knowledge questions. Meanwhile, attitude questions offered answer choices of “strongly agree,” “agree,” “disagree,” and “strongly disagree”. Experience questions were answered with “ever” or “never”.
Data were collected using a structured and validated questionnaire. Prior permission to use the questionnaire was obtained from the original author (Llma DL et al.) via e-mail communication.
Sample Size:
The sample size was calculated using Slovin’s formula with a 5% margin of error.
With an estimated population of 240 pharmacists, the required sample size was:
n=2401+240 0.052
= 150
Thus, a sample of 150 pharmacists was considered adequate for the study.
Inclusion Criteria:
Exclusion Criteria:
Statistical Analysis:
All collected data were entered into Microsoft Excel and analyzed using IBM SPSS Statistics (Version 26) and Microsoft Excel. Descriptive statistics such as frequency, percentage, mean, were used to summarise demographic characteristics and responses for knowledge, attitude, and experience domains. Each knowledge item was scored as 1 for a correct response and 0 for an incorrect or “don’t know” response. Attitude statements were measured using a four-point Likert scale, ranging from 1 (strongly disagree) to 4 (strongly agree), and experience items were coded as 1 for “ever” and 0 for “never.” Composite domain scores for knowledge, attitude, and experience were calculated as the mean of all respective item scores for each respondent. The relationships among knowledge, attitude, and experience scores were examined using Spearman’s rank correlation coefficient (ρ) to determine the strength and direction of association between variables.
RESULTS
The survey was distributed to 150 registered pharmacists meeting the eligibility criteria.
The Data was analysed based on the following parameters
Table 1: Gender wise distribution of Participants (n=150)
|
Gender |
No of participants (n=150) |
Percentage (%) |
|
Male |
102 |
68 |
|
Female |
48 |
32 |
Out of the 150 registered pharmacists included in the study, 102 (68%) were male and 48 (32%) were female, resulting in a male-to-female ratio of 17:8, which indicates a predominance of male participants in the study population and the majority (80.67%) belonged to the 19–28 years age group, followed by 29–38 years (15.33%), 39–48 years (1.33%), and 49–58 years (2.67%). This age distribution resulted in a mean age of 26.1 ± 6.18 years, indicating that the study population was predominantly younger. Data were shown in Table 1 & fig.1
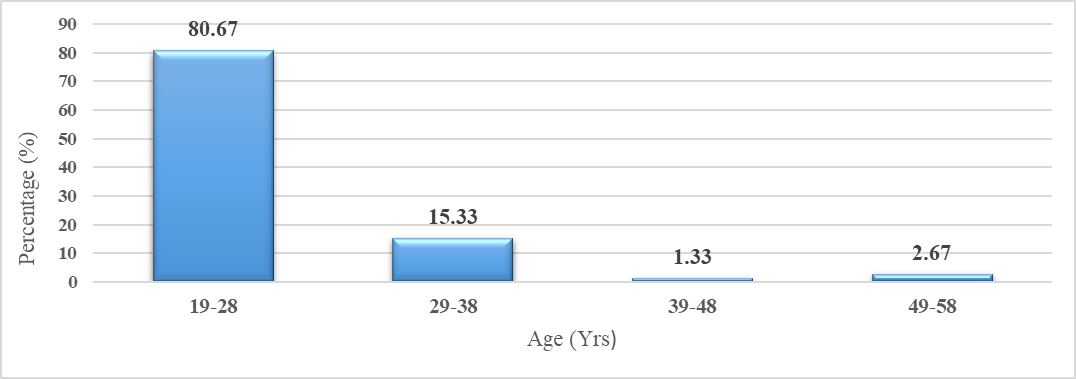
Fig. 1: Age-wise distribution of Participants
Table 2: Educational Background (n=150)
|
Qualification |
Frequency |
Percentage (%) |
|
Pharm.D |
68 |
45.33 |
|
B.Pharm |
39 |
26.00 |
|
M.Pharm |
23 |
15.33 |
|
D. Pharm |
20 |
13.33 |
The educational background of the participants revealed that the majority were Pharm.D graduates, comprising 68 out of 150 participants (45.33%). This was followed by B.Pharm graduates, accounting for 39 participants (26.00%), M.Pharm graduates representing 23 participants (15.33%), and D.Pharm graduates comprising 20 participants (13.33%), as shown in Table 2.
Table 3: Length of Practicing Pharmaceutical Care (Years) (n=150)
|
Length of Practicing Pharmaceutical Care (Years) |
No of Participants (n=150) |
Percentage (%) |
|
< 1 |
83 |
55.33 |
|
1-3 |
32 |
21.33 |
|
4-6 |
18 |
12 |
|
> 6 |
17 |
11.33 |
significant proportion, 83 participants (55.33%), reported having less than one year of experience. This was followed by 32 participants (21.33%) with 1 to 3 years of experience, 18 participants (12%) with 4 to 6 years, and 17 participants (11.33%) with more than 6 years of practice. These results indicate that the majority of respondents were relatively new to the practice of pharmaceutical care, reflecting a younger or early-career demographic within the sample population. Details were shown in Table 3.
Table 4: Knowledge-based questions (n=150)
|
Questions |
Average scores (%) |
|
Pharmacists and patients meet face to face on telepharmacy |
80.7 |
|
Knowledge related to information and communication technology (telecommunications) is needed by pharmacists to conduct telepharmacy |
96.7 |
|
Telepharmacy can be done using video conference (e.g zoom atau Google Meet) |
95.3 |
|
Telepharmacy can be done using digital health applications (e.g halodoc, alodoc, etc) |
93.3 |
|
Purchases of narcotic drugs can be served by electronic prescription |
65.3 |
|
Purchases of psychotropic drugs can be served by electronic prescription |
58.7 |
|
Telepharmacy allows pharmacists to confirm electronic prescriptions with doctors |
92.7 |
|
Telepharmacy allows pharmacists to provide recommendations for overcoming drug-related problems in electronic prescriptions to doctors |
93.3 |
|
Pharmacists can not gather patients' information by telepharmacy |
74.7 |
|
Monitoring patients' medications can be done by telepharmacy |
91.3 |
|
Drug counselling can be done by telepharmacy |
94.0 |
|
Providing information on drugs and medical devices can be done by telepharmacy |
94.7 |
|
Telepharmacy increases access to pharmacy services in areas with a limited number of pharmacists |
94.0 |
|
Telepharmacy reduces the number of direct patients visit to pharmacy service facilities |
93.3 |
|
Telepharmacy is a legally recognized pharmacy service |
93.3 |
Average scores for knowledge-based questions were calculated. Pharmacists demonstrated high knowledge of telepharmacy, especially its technological requirements (96.7%) and communication tools like video conferencing (95.3%) and digital health apps (93.3%). However, understanding of electronic prescriptions for controlled substances was lower (narcotics 65.3%, psychotropics 58.7%). Data were depicted in Table 4.
Table 5: Attitude-based questions (n=150)
|
Questions |
Average scores (%) |
|
Telepharmacy allows me to get access to pharmacy services |
84.0 |
|
I can use telepharmacy anytime and anywhere as long as I have a telecommunications or internet signal |
86.5 |
|
I feel I can have good communication with pharmacists via telepharmacy |
83.3 |
|
Telepharmacy allows to improve the quality of my communication with the pharmacists |
81.7 |
|
I can save time on visits to pharmacy service facilities if I use telepharmacy |
84.5 |
|
I can save on medical costs if I get pharmacy services via telepharmacy |
78.8 |
|
The confidentiality of my information can be maintained through telepharmacy |
72.2 |
|
Telepharmacy makes it possible to increase the quality of the pharmacy services that I receive |
78.0 |
|
Telepharmacy may improve my medication adherence |
76.2 |
|
In my opinion, pharmacists' knowledge of information and communication technology (telecommunications) is important for telepharmacy |
88.7 |
|
In my opinion, it is important to provide knowledge related to telepharmacy to pharmacy students to help utilise telepharmacy in the future |
77.5 |
|
I need adequate electronic equipment (e.g cellphone) for telepharmacy |
79.7 |
|
I think that the existing laws and regulations are sufficient to regulate the technical implementation of telepharmacy |
75.5 |
As shown in Table 5, attitudes were generally positive, with 84% acknowledging improved access to pharmacy services and 86.5% confident in telepharmacy use via internet. Time savings (84.5%) and enhanced communication (83.3%) were recognized, though concerns about data confidentiality were lower (72.2%). Most agreed on the importance of information and communication technology knowledge (88.7%) and telepharmacy education (77.5%).
Table 6: Experience-based questions (n=150)
|
Questions |
Average scores (%) |
|
I received drug counselling by the phone from the pharmacist |
53.3 |
|
I received drug counselling via video conference (eg. Zoom or Google Meet) from the pharmacist |
30.0 |
|
I received drug counselling via a messaging service application (e.g WhatsApp) from the pharmacist |
39.3 |
|
I received drug counselling via a digital health service application (halodoc, alodoc, etc.) from the pharmacist |
26.7 |
|
I received medication monitoring by the phone from the pharmacist |
38.7 |
|
I received medication monitoring via video conference (eg. Zoom or Google Meet) from the pharmacist |
24.7 |
|
I received medication monitoring via a messaging service application (e.g WhatsApp) from the pharmacist |
32.0 |
|
I received medication monitoring via a digital health service application (halodoc, alodoc, etc.) from the pharmacist |
25.3 |
|
I received information regarding medication by the phone from the pharmacist |
45.3 |
|
I received information regarding medication via video conference (eg. Zoom or Google Meet) from the pharmacist |
30.7 |
|
I received information regarding medication via a messaging service application (e.g WhatsApp) from the pharmacist |
35.3 |
|
I received information regarding medication via a digital health service application (halodoc, alodoc, etc.) from the pharmacist |
22.0 |
|
I asked the pharmacist for drug-related information by the phone |
45.3 |
|
I asked the pharmacist for drug-related information via video conference (eg. Zoom or Google Meet) |
30.0 |
|
I asked the pharmacist for drug-related information via a messaging service application (e.g WhatsApp) |
36.7 |
|
I asked the pharmacist for drug-related information via a digital health service application (halodoc, alodoc, etc.) |
24.7 |
|
I asked the pharmacist for general health information (other than medications) by the phone |
40.0 |
|
I asked the pharmacist for general health information (other than medications) via video conference (eg. Zoom or Google Meet) |
27.3 |
|
I asked the pharmacist for general health information (other than medications) via a messaging service application (e.g WhatsApp) |
36.0 |
|
I asked the pharmacist for general health information (other than medications) via a digital health service application (halodoc, alodoc, etc.) |
24.7 |
|
I bought medicine with an electronic prescription |
35.3 |
|
I bought medicine without a prescription (over the counter-medication) via telepharmacy |
33.3 |
|
I bought medical equipment (such as a thermometer, oxygen mask, etc.) via telepharmacy |
38.0 |
|
I bought other medical materials (such as masks, handscoons, etc.) via telepharmacy |
34.7 |
|
I provided adequate electronic equipment (e.g cellphone) for telepharmacy |
38.7 |
|
I studied the laws and regulations related to telepharmacy |
32.7 |
Table 6 highlights that experience levels were moderate, favouring phone-based counselling (53.3%) over video or app-based interactions (below 40%). Only 38.7% had adequate electronic devices, and 32.7% were familiar with telepharmacy regulations.
Table 7: Correlation of level of knowledge, attitude, and experience of registered pharmacists related to telepharmacy (n=150)
|
Variables |
|
p-value |
||
|
Knowledge to Attitude |
0.011 |
0.908 |
||
|
Attitude to Experience |
0.032 |
0.754 |
statistically significant (p < 0.05)
The correlation analysis between the three domains revealed no statistically significant association. The Spearman’s rank correlation coefficient showed a very weak positive correlation between knowledge and attitude (ρ = 0.011, p = 0.908) and between attitude and experience (ρ = 0.032, p = 0.754). These findings indicate that although participants demonstrated high knowledge levels and positive attitudes toward telepharmacy, these factors did not significantly influence their actual experience or engagement in telepharmacy practices. Data were shown in Table 7.
DISCUSSION
In the current study, the mean knowledge score exceeded 90% for most questions, reflecting a strong understanding of telepharmacy’s technological components, such as video conferencing and digital health applications. However, a comparatively lower understanding was observed for the legal aspects related to electronic prescriptions of controlled substances (65.3% for narcotics and 58.7% for psychotropics). Similar findings were reported by Llma et al. (2024) in Indonesia, where pharmacy students demonstrated good knowledge about telecommunication tools but lacked awareness of regulatory frameworks. Likewise, Ahmed et al. (2023) reported that hospital pharmacists in Saudi Arabia showed high readiness but had limited understanding of policy and legal aspects governing telepharmacy. This suggests that while the conceptual and technical awareness of telepharmacy is well established, formal education about regulatory and ethical issues remains insufficient. Regarding attitudes, the participants in this study exhibited a favourable perception of telepharmacy, with an average agreement level above 80%. Most respondents believed that telepharmacy improves accessibility, saves time, and enhances communication between pharmacists and patients. This positive outlook aligns with studies conducted in Saudi Arabia (Alsultan et al., 2024) and Indonesia (Alfian et al., 2023), which also reported that students recognized the importance of incorporating telepharmacy into future practice and education. However, the current study also revealed that only 72.2% of participants were confident about maintaining confidentiality during telepharmacy consultations. A similar concern regarding privacy and data protection was highlighted by Elhadi et al. (2021), emphasizing the need for standardized cybersecurity training and digital ethics in pharmacy curricula.
In terms of experience, the findings indicate moderate involvement in telepharmacy-related activities, with the majority reporting engagement through phone-based counselling (53.3%), while fewer used video conferencing or digital applications (< 40%). These results are comparable to those of Ghozali et al. (2024), who found that young pharmacists in rural Indonesia had limited hands-on telepharmacy experience, primarily restricted to basic telecommunication tools. Similarly, Brown et al. (2022) observed that patient satisfaction with telepharmacy was high during the COVID-19 pandemic, yet the service delivery relied mostly on simple communication modes rather than integrated telehealth systems.
The correlation analysis in this study revealed no significant association between knowledge, attitude, and experience (p > 0.05). This suggests that although pharmacists are knowledgeable and hold positive attitudes toward telepharmacy, these do not necessarily translate into actual practice. Similar findings were reported by Llma et al. (2024) and Ahmed et al. (2023), who noted weak correlations between knowledge and readiness for telepharmacy implementation. These results collectively imply that high awareness and favourable perceptions alone are not sufficient to promote practice without adequate exposure, institutional encouragement, and regulatory facilitation.
CONCLUSION
The present study concludes that pharmacists in North Karnataka exhibit excellent knowledge and positive attitudes toward telepharmacy; however, their practical exposure and implementation remain limited. Although pharmacists recognize the benefits of digital healthcare and demonstrate conceptual readiness, this has not yet translated into consistent practice due to infrastructural, regulatory, and training constraints. Strengthening telepharmacy education, integrating digital health components into pharmacy curricula, and establishing supportive national policies are crucial to bridge this gap and promote effective adoption. Future efforts should prioritize the inclusion of structured telepharmacy modules in undergraduate and postgraduate pharmacy programs, along with continuous professional development initiatives aimed at improving digital competence. Additionally, the creation of standardized operational frameworks and accessible technological infrastructure will empower pharmacists to confidently implement telepharmacy services, thereby enhancing patient access and optimizing pharmaceutical care in India’s evolving healthcare system.
CONFLICTS OF INTEREST
The author declares no conflicts of interest related to this research work. The study was conducted independently, without any financial or personal relationships that could have influenced the outcomes or interpretations of the results.
REFERENCES



Binu K M*, Doddayya H, Aniket D M, Keerthi J, Rajesh B, Telepharmacy Knowledge, Attitude, And Experience Among Pharmacists in North Karnataka: A Cross-Sectional Study, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 896-905. https://doi.org/10.5281/zenodo.18207305
 10.5281/zenodo.18207305
10.5281/zenodo.18207305
