1,2,3,4,5 Adichunchanagiri College of Nursing, Adichunchanagiri University, B G Nagara, Nagamangala, Mandya, Karnataka, India-571448
6 Sri Adichunchanagiri College of Pharmacy, Adichunchanagiri University, B.G. Nagara, Mandya, Karnataka, India - 571448
Hypertension is known to be a major contributor to cardiovascular diseases worldwide, and an ever-growing body of evidence shows therapeutic nutrition to be an important and viable measure in the prevention and long-term management of hypertension. From the dietary modifications available, the ones most thoroughly studied and documented have been the DASH (Dietary Approaches to Stop Hypertension) diet, which can result in a significant decrease in systolic and diastolic blood pressures. The diet derives its action from a nutrient-rich framework of fruits, vegetables, whole grains, low-fat dairy, lean protein, nuts, and legumes, and limits sodium, saturated fat, red meat, and added sugars. Additional nutritional strategies like directed sodium reduction, potassium enrichment, adherence to Mediterranean and plant-forward diets, and potassium-enriched salt substitutes have evidenced complementary effects on blood pressure regulation in different populations. From a systems-biology perspective, these dietary patterns act on individual antihypertensive pathways that are interrelated physiologically. Important mechanisms include modulation of neurohormonal systems such as renin–angiotensin–aldosterone signalling, modifying renal sodium excretion and fluid balance, and regenerating endothelial function via an increase of nitric oxide bioavailability. A disproportionate contribution to vascular tone is being made by dietary reduction of oxidative stress, low-grade inflammation, and sympathetic overstimulation. More recent evidence implicates gut microbiota in such modulation, whereby fiber-rich, plant-based diets promote metabolites that support vascular and metabolic homeostasis. All these findings put therapeutic nutrition as one of the major evidence-backed methods for hypertension control and designate it for incorporation into precision dietary frameworks tailored to individual cardiometabolic profiles.
Hypertension, colloquially known as "the silent killer", imperceptibly increases the pressure in the arteries and forces the heart to work more, thereby raising the risk of cardiovascular, renal, and neurologic conditions [1]. More than a billion people are affected worldwide while causing the greatest burden of mortality less than the age of 70 among all diseases. Most cases are found in low- and middle-income countries where risk factors are still increasing (Figure 1).
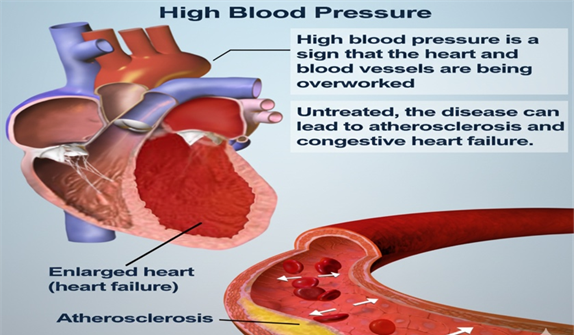
Figure 1: Effects of Chronic High Blood Pressure on the Heart and Blood Vessels
DEFINITION
Hypertension (HTN) is characterized as a chronic condition associated with sustained elevated arterial blood pressure-a systolic blood pressure ≥130 mm Hg and/or a diastolic blood pressure ≤80 mm Hg, in accordance with contemporary clinical guidelines[2, 3]. It reflects a sustained increase in vascular resistance or cardiac output and is a major modifiable risk factor for most cardiovascular, renal, and cerebrovascular diseases (Figure 2). Hence, a diagnosis of hypertension is established through repeated standardized blood pressure measurements in either clinical or ambulatory conditions to verify persistently above-normal readings rather than on isolated ones.
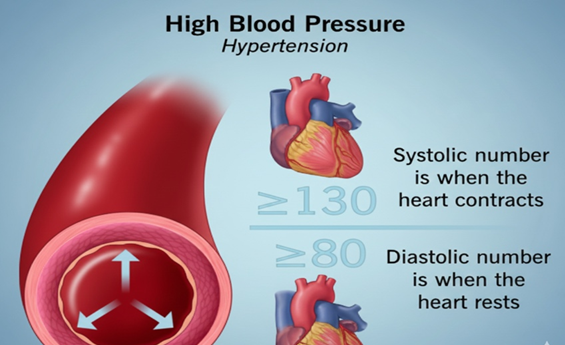
Figure 2: Hypertension: Systolic and Diastolic Blood Pressure
STAGES AND TYPES OF HYPERTENSIONS
Table 1: Classification of Blood Pressure Categories Based on Systolic and Diastolic Levels
|
Blood Pressure Category |
Systolic (mm Hg) |
Diastolic (mm Hg) |
|
Normal |
Less than 120 |
Less than 80 |
|
Elevated |
120–129 |
Less than 80 |
|
Hypertension Stage 1 |
130–139 |
80–89 |
|
Hypertension Stage 2 |
140 or higher |
90 or higher |
|
Hypertensive Crisis (consult doctor immediately) |
Higher than 180 |
Higher than 120 |
Blood Pressure Classification
Blood Pressure Classifications. Blood pressure categories are plotted based on reading as systolic blood pressure (SBP), which reflects arterial pressure during cardiac contraction, and diastolic blood pressure (DBP) during cardiac relaxation (Table 1). The categories serve as help for clinicians in assessing cardiovascular risk, guiding treatment choice, and monitoring the progression of hypertension [4].
Normal Blood Pressure:
This category entails persons having an SBP of less than 120 mm of Hg and a DBP of less than 80 mm of Hg. These values suggest normal arterial pressure with minimal risk for hypertensive complications.
Elevated Blood Pressure:
Elevated blood pressure presents an SBP of 120 to 129 mm Hg and a DBP of <80 mm Hg. This state puts the subject at greater risk and predisposed to developing overt hypertension, barring any changes in lifestyle, with some degree of assurance.
Hypertension – Stage 1:
Stage 1 hypertension may be defined as an SBP of 130-139 mm Hg or a DBP of 80-89 mm Hg. Lifestyle interventions may be required for these individuals but may also require pharmacological therapy depending on their cardiovascular risk profile.
Hypertension – Stage 2:
This stage represents significant elevation with SBP ≥140 mm Hg or DBP ≥90 mm Hg. Those patients would normally require prompt initiation of treatment with antihypertensive drugs, together with lifestyle changes.
Hypertensive Crisis (Medical Emergency):
A condition wherein SBP is >180 mm Hg and/or DBP is >120 mm Hg is known as a hypertensive crisis. It warrants immediate medical evaluation since such an emergency will result in acute target-organ damage, right from stroke, myocardial infarction, renal injury, or heart failure.
Types of Hypertension
The hypertension can be viewed in multiple ways, categorized on the basis of different mechanisms as well as modes of clinical presentations and therapies [5]. All end up causing high blood pressure, whose distinct pathways of causation necessitate accurate classification for proper management (Figure 3).
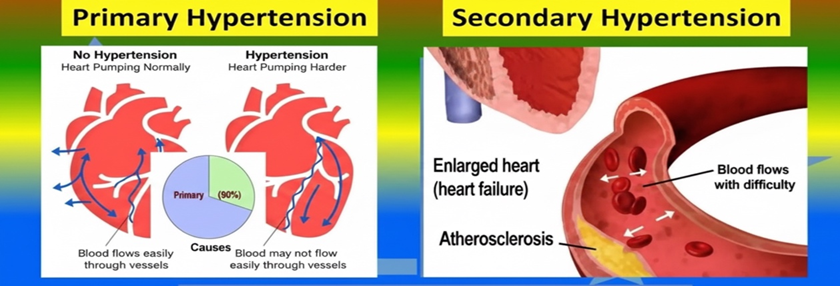
Figure 3: Causes of Hypertension: Primary vs. Secondary
1. Primary (Essential) Hypertension
Primary hypertension is the commonest variant, along with accounting for nearly 90-95% of all cases. It is gradually developed over the years and does not have any one identifiable cause [6-8]. Instead, it arises from complex interactions of genetic predisposition, environmental influences, neurohormonal dysregulation, and vascular remodelling. The diagnosis shows blood pressure readings consistently above 130/80 mm Hg. Typically not symptomatic, in some individuals nonspecific manifestations such as headaches, fatigue, palpitations, shortness of breath, or visual disturbances may develop.
2. Secondary Hypertension
Secondary hypertension is due to some underlying identificable and usually reversible condition, for example, renal artery stenosis, chronic kidney disease, endocrine disorders (e.g., hyperthyroidism, Cushing's syndrome, primary aldosteronism), obstructive sleep apnea, or medicines. It is often abrupt in onset and may be disproportionately severe [9, 10] compared with primary hypertension. Corrective measures for the underlying pathology usually improve blood pressure or return it to normal.
3. Resistant Hypertension
Resistant Hypertension Defined as blood pressure remaining above 140/90 mm Hg with the concurrent use of three or more optimally dosed antihypertensive drugs, including a diuretic, resistant hypertension poses increased risks for cardiovascular events, stroke, and renal impairment. Thorough investigation for poor medication adherence, secondary causes, and lifestyle factors must be conducted in suspected cases.
4. Malignant (Accelerated) Hypertension
Malignant hypertension is a rapid, severe elevation in blood pressure, generally accompanied by diastolic levels exceeding 120 mm Hg, associated with acute damage to target organs such as retinal hemorrhages, encephalopathy, or renal failure. It eventually occurs in patients with uncontrolled primary hypertension, and it requires immediate medical intervention.
5. Portal Hypertension
Portal hypertension refers to elevated pressure in the portal venous system, which is most commonly caused by liver cirrhosis, portal vein thrombosis, or other structural disorders of the liver. In addition, normal venous flow between the gastrointestinal organs and the liver about puts increased pressure and gives rise to the following: ascites, variceal bleeding, and splenomegaly. Although distinct from that of systemic hypertension, this is still clinically relevant in hepatology.
6. Isolated Systolic Hypertension (ISH)
Isolated systolic hypertension is defined as a clinical state with an elevated systolic pressure (≥130–140 mm Hg) with normal diastolic readings (<80 mm Hg). It occurs commonly in the elderly and is largely due to age-related arterial rigidity with lesser vascular compliance and higher pulse-wave velocity. ISH greatly increases the risk of myocardial infarction, stroke, and heart failure.
Causes of Hypertension
Hypertension results from a combination of genetic, environmental, physiological, and pathological variables [11-14]. Broadly, it may be classified into primary (essential) hypertension and secondary hypertension according to its origins.
Primary or essential hypertension accounts for approximately 90% of all hypertension cases and develops insidiously over many years. It has no single identifiable etiology, although a strong hereditary predisposition is implicated. Genetic factors affect renal sodium handling, vascular tone, hormonal regulation, and sympathetic nervous system activity, all of which may contribute to the chronically raised blood pressure. There is no cure for primary hypertension, but lifestyle changes and medications can be employed to control it effectively and thus reduce long-term risk for cardiovascular disease.
In the minority of instances, secondary hypertension occurs in less commonly, due to a distinct and identifiable condition. Examples of such conditions include kidney disease, endocrine disorders (such as hyperaldosteronism, thyroid disorders, and Cushing syndrome), obstructive sleep apnea, congenital vascular anomalies, and some drugs (like NSAIDs, oral contraceptives, and steroids). Unlike primary hypertension, once the underlying cause is addressed, blood pressure is frequently brought significantly down, if not normalized.
Risk Factors of Hypertension
Hypertension is commonly referred to as a "silent killer" as it proceeds insidiously but greatly increases the risk of stroke, myocardial infarction, heart failure, and other kidney diseases. Several risk factors are well-known, and it is essential to know them for prevention and effective management. Those classified as non-modifiable risk factors are:
Non-Modifiable Risk Factors
These risk factors are not modifiable; nonetheless, these help in detecting susceptibilities in persons at risk (Figure 4).
Figure 4: Non-Modifiable Risk Factors (Age, Genetics, Ethnicity, Sex)
Genetics
Family history of hypertension especially among first-degree relatives at less than age 60 contributes enormously to one's risk. Genetic factors affect vascular reactivity, the activity of the renin-angiotensin-aldosterone system, and salt sensitivity; such risk gets much worse if several family members are involved [15, 16].
Age
As individuals grow older, the likelihood of a rising blood pressure becomes more considerable [17]. The age-related changes, such as increased stiffness of arteries, endothelial dysfunction, and reduced elasticity due to age, would weaken the arteries' ability to expand and contract and elevate systolic pressure over the years.
Sex
Men and women may also influence the patterns of their hypertension come later in life when they mature. Although men develop hypertension earlier in adulthood, the prevalence among women sharply increases at and after 60 years of age. Changes associated with post-menopause, including altered hormonal levels mostly estrogen and other changes in the vasculature's physiology, account for that shift in women.
Ethnicity
Certain ethnic groups like blacks and persons of African and Black Caribbean descent have been shown to suffer from hypertension more and probably more severe forms. This genetic predisposition towards salt sensitivity might make one's systolic blood pressure increase by approximately 5 mm Hg with a small increase in salt intake of about 1 g per day. This may further potentiate the cause through other environmental and socioeconomic factors.
Modifiable Risk Factors of Hypertension
Modifiable risk factors are elements associated with lifestyle and behavior which an individual can change in order for him to develop hypertension (Figure 5). Modifiable risk factors are those very important in primary prevention of the high blood pressure condition and in determining treatment responses among those already diagnosed with hypertension.
Figure 5: Modifiable Risk Factors (Body Weight, Salt Intake, Smoking, Exercise)
• High Salt Intake
Dietary salt in excess quantity has been one of the most eminent reasons for having an elevated blood pressure. Although health guides prescribe a restricted salt intake of 6 grams/day, many adults such as those in the UK average about 8 grams daily. A high sodium intake helps in increasing blood volume due to the retention of water, which subsequently raises blood pressure and adds strain on the cardiovascular systems.
Generally high sodium foods include the following:
Sodium restriction has been shown to reduce systolic and diastolic blood pressures significantly in every age group.
• Body Weight
More body weight increases the workload of the heart as well as associated complications such as insulin resistance, systemic inflammation, and vascular dysfunction, all resulting in increased blood pressure. Studies suggest that reducing by 10kg in body weight would on average reduce systolic blood pressure by 5-20 mmHg which means the significant effects of weight loss on cardiovascular health.
• Smoking
A strong and active inciter on blood pressure elevation is smoking. According to studies, one cigarette raises systolic blood pressure by about 5 to 10 mmHg because of nicotine's dictating effect on this important function; it produces some stimulatory effect on the heart and vasoconstriction. To make the conditions worse, chronic smoking speeds up stiffening of the arteries and damages the endothelium, thereby increasing risk for persistent hypertension and cardiovascular events [18-20].
• Physical Inactivity
Regular physical activity improves cardiac efficiency, enhances vascular elasticity, and inhibits excessive stimulation of the sympathetic nervous system. The recommended dosages of 150 minutes of moderate activity, such as brisk walking, or 75 minutes of vigorous activity, such as running, have been shown to lower blood pressure by 5-8 mmHg. Irregular physical activity helps people maintain their weight in a healthy range while also decreasing levels of stress, which aids in supporting optimal blood pressure control.
Hypertension Diet Management
Dietary changes, among the key non-pharmacological measures for hypertension management, comprise one of the most scientifically validated interventions: the Dietary Approaches to Stop Hypertension (DASH) diet. Originally developed via NIH-supported clinical research, the DASH diet was designed to prevent, reduce, and manage high blood pressure while improving lipid profiles and cardiometabolic health [21, 22].
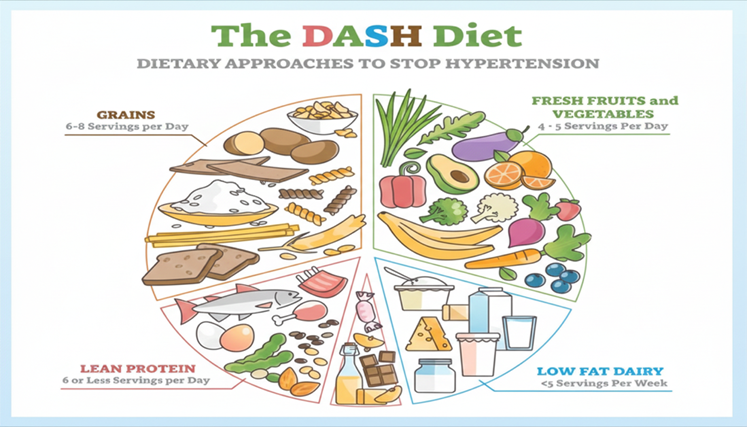
Figure 6: The DASH Diet: Dietary Approaches to Stop Hypertension
What is the DASH Diet?
The DASH diet is an evidence-based eating pattern that shows nutrient-dense foods naturally containing high contents of potassium, magnesium, and calcium, three vital minerals important in vascular relaxation, sodium equilibriums, and endothelial function and, consequently, blood pressure regulation [23, 24].
It promotes a dietary pattern containing:
At the same time, the diet excludes those elements known to worsen hypertension, such as:
DASH Diet and Salt (Sodium) Intake
Systolic and diastolic blood pressure declines due to decreased vascular stiffness, oxidative stress, and raas activation coupled with improvement in LDL cholesterol levels, taking it to significant cardiovascular disease and stroke risks decline.
DASH Diet and Salt (Sodium) Intake
The low sodium intake component featured really prominently in the DASH dietary strategy. The general DASH guidelines recommend:
This other, but intensive variant is recommended for those who have hypertension, diabetes, kidney diseases, or increased risk of CVD:
Clinical evidence indicates that this reduction would produce significantly greater declines in blood pressure, particularly in salt-sensitive people. Patients will determine which plan of the two will work for them depending on personal health conditions, blood pressure goals, and tolerance. Patients are thus advised to schedule a visit with a healthcare provider or nutrition specialist to determine the ideal level of sodium restriction.
DASH Diet: What to Eat (Elaborated Explanation)
The DASH (Dietary Approaches to Stop Hypertension) diet is a scientifically proven dietary modelfor lowering high blood pressure and promoting cardiovascular health [25]. It promotes a balanced, nutrient-rich, and sustainable diet, according to which flexibility allows easy adoption by people across all cultures and socioeconomic levels. A basic tenet of DASH is eating foods high in potassium, magnesium, calcium, fiber, and high-quality protein-all of which have been shown to help regulate vascular tone, enhance endothelial function, reduce arterial stiffness, and oppose excess sodium. Through several ways, these nutrients work together to lower blood pressure by promoting equilibrium of fluid regulation, reducing systemic inflammation, and improving insulin sensitivity, thus maintaining normal cardiac function.
The DASH diet encourages whole grains, colourful vegetables and fresh fruits, lean meats, legumes, nuts and seeds, and low-fat dairy. People are advised to cut back on sodium, saturated fats, trans fats, added sugars, and processed foods. Therefore, the DASH approach is not an exclusive one; rather, it comprises heart-healthy eating behaviours that can be sustained and adapted to meals prepared at home, in restaurants, or from commercial food outlets.
DASH Diet: Suggested Servings (Highly Elaborated Explanation)
The DASH diet provides structured daily and weekly serving recommendations to help individuals meet their nutrient requirements without exceeding caloric limits [26, 27]. These serving sizes guarantee the diet is balanced, realistic, and adaptable to various age groups, body weights, and activity levels. For example, the standard guidelines of a 2000-calorie/day diet include:
1. Grains – 6 to 8 servings per day
Grains are the basic energy source in DASH diet, especially whole grains like whole-wheat bread, brown rice, quinoa, millet and oats. Complex carbohydrates, fiber, B-vitamins, and essential minerals are afforded by these sources.
One serving equals:
Whole-grain foods help to keep a healthy blood sugar level, prolong satiety, boost digestive health, and may lower systolic blood pressure through better metabolic functioning.
2. Vegetables – 4 to 5 servings
Vegetables provide potassium, magnesium, antioxidants as well as dietary fiber that are needed for vasodilation and lessened oxidative stress.
One serving equals:
Some of the particularly good article for reducing blood pressure are leafy greens (spinach, kale), cruciferous (broccoli, cauliflower), and colored (carrots, bell peppers).
3. Fruits - 4 to 5 servings in a day
Fruits supply vitamins, antioxidants, fiber, and naturally occurring minerals, especially potassium, which influence sodium balance.
One serving equals:
Healthy arteries are better for cholesterol levels and take their roots from these fruits, e.g., bananas, oranges, melons, berries, and apples.
4. Fat-Free or Low-Fat Dairy – 2 to 3 servings daily
Dairy products are very potent sources of calcium and protein, both linked with improved elasticity and reduced stiffness in blood vessels.
One serving equals:
Low-fat helps prevent high amounts of saturated fat consumption, which is a protection from atherosclerosis.
5. Lean Meats, Poultry, and Fish – up to 6 small servings daily
Protein is a prerequisite for muscle repair, enzyme production, and metabolic health, and DASH recommends the consumption of lean sources such as skinless poultry, fish, and small amounts of red meat.
One serving equals:
Salmon and mackerel are the types of fish that are high in omega-3 fatty acids; hence they reduce further inflammation and cardiovascular risk.
6. Pulses nuts, and seeds- 4 -enough 5 servings per week.
Foods in these groups furnish plant protein, healthy fats and fiber as well as magnesium; Per equal serving:
Regular intake improves the lipid profile, stabilizes blood glucose, and supports long-term weight control.
7. Fats and Oils - 2 to 3 servings per day
Healthy fats help hormone balance, nutrient absorption, and anti-inflammatory pathways.
One serving equals:
DASH diet emphasizes that fats, especially monounsaturated and polyunsaturated sources mostly from vegetable oils, nuts, seeds, and fish, are more acceptable than saturated and trans fats.
8. Sweets and Added Sugars - restricted to 5 servings or fewer per week.
Sugar-rich foods lead to weight gain, insulin resistance, and increased blood pressure when consumed in excess.
One serving equals:
The DASH approach encourages occasional consumption in small amounts to maintain adherence without feeling deprived.
DASH Diet: Alcohol and Caffeine
While following the DASH food pattern, consider lifestyle changes regarding alcohol and caffeine consumption since this is crucial for an individual with hypertension. High blood pressure, endothelial dysfunction, and adverse cardiovascular outcomes are all consequences of heavy drinking. In accordance with the Dietary Guidelines for Americans, women should consume no more than one drink per day and men should consume no more than two drinks a day. If you exceed these amounts, the blood-pressure-lowering effects of the DASH diet could be compromised or lead to greater weight problems, arrhythmias, or increased triglycerides. In clinical judgment, stricter limits may recommend for those patients already diagnosed with hypertension.
There are no specific limitations in the DASH diet concerning caffeine however, studies indicate that caffeine does raise blood pressure temporarily by stimulating the sympathetic nervous system; this particularly occurs in caffeine-sensitive individuals or huge caffeine consumers. While habitual long-term consumption of caffeine may not affect the baseline blood pressure in most, people with uncontrolled hypertension and those who present alterations in health status using caffeine should thus limit their intake. A healthcare professional should be consulted to determine if moderation of caffeine is necessary depending on the individual's blood pressure responses.
Strategies Employing the DASH Diet to Reduce Salt:
DASH naturally has a very low sodium content, so it is a good method to go low on overall salt without jeopardizing nutrition adequacy. Further, the following additional deliberate approaches may assist individuals in reaching the recommended sodium intake of 1,500–2,300 mg daily:
Practical Salt Reduction
Such strategies help maintain sodium intake within recommended limits while promoting the cardiovascular health objective of the DASH diet as a whole.
REFERENCES






Asha Siddabhovi, Shobha Rajanna, Sreelakshmi Veerendra, Shashikala Krishnamurthy, Rachana Giriswamy, Pavan Kumar Chikkavalli Muddanna, Therapeutic Nutrition in Hypertension: A Systems-Biology Perspective on Diet-Induced Vascular Regulation, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 1878-1889. https://doi.org/10.5281/zenodo.17883273
 10.5281/zenodo.17883273
10.5281/zenodo.17883273
