
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1Department Of Pharmacy Practice, Hindu College of Pharmacy.
2,3,4,5Acharya Nagarjuna University.
Superficial dermatophyte infections show characteristic scaly and red ring-shaped lesions which expand outward from their edges while their centres clear and medical professionals rely on these physical signs to establish a diagnosis. The diagnosis of Tinea incognito (TI) or incognita refers to superficial fungal infections whose appearance differs from normal skin because of topical or systemic corticosteroid usage. Recent associations have been made between the development of this condition and the use of other immunosuppressive agents such as calcineurin inhibitors, tumor necrosis factor inhibitors, and fumaric acid esters for psoriasis treatments. Applying topical corticosteroids (TCS) to fungal infections produces unusual and complex manifestations which can result in extensive presentations difficult for clinicians to diagnose. This review aims to present a detailed examination of the causes behind Tinea Incognito and its clinical features alongside diagnostic methods and treatment strategies.
Topical Immunosuppressive agents or Systemic steroids create atypical presentations of dermatophyte infections which are then classified as Tinea Incognito (TI)5. Topical corticosteroids serve as the main cause of TI because they are commonly prescribed for existing skin conditions by medical professionals or wrongly self-administered for Fungal infections that have not been diagnosed6. The fungal infection spreads progressively while presenting symptoms similar to multiple skin disorders which results in inaccurate diagnoses and treatment delays or failures7. Steroid-modified Tinea describes TI which has emerged as a growing medical concern8. The word "Incognito" describes how clinical indicators for a Fungal infection remain hidden9. Dermatophytosis represents a fungal infection which attacks the skin alongside hair and nails with Trichophyton rubrum being the most common source10. The condition typically begins with a scaly skin rash that creates a round area with a raised edge. The infection’s characteristic appearance reduces when Steroids are used to treat it which results in Tinea Incognito11. Tinea Incognito commonly manifests on facial and hand areas12, as documented in section. The early detection of the condition enables proper treatment to be delivered and stop further transmission13. Tinea Incognito differs from standard fungal infections by extending its reach beyond the usual circular shape. As the scaly border progresses, it can vanish and red patches might develop at the center or edges which adds to the difficulty of identifying the condition14. Misdiagnosis happens often because these hallmark fungal traits do not exist15. At first application steroids diminish inflammation which creates the illusion of infection improvement. Immune suppression from prolonged treatment leads to rapid fungal growth that produces the unusual appearance of tinea incognito. Patients might mistake lesions for typical fungal infections and reapply corticosteroids because they remain different from typical infections even after treatment cessation. Diagnosis is confirmed through microscopic examination of skin scrapings16, though testing should be performed after discontinuing corticosteroids for a few days to improve accuracy17. Treatment involves stopping corticosteroid use and applying antifungal creams for mild cases. Severe cases may require oral antifungal medications like Terbinafine or Fluconazole18. If bacterial infection occurs in open lesions, antibiotics may be needed19. Tinea incognito was first identified in 1968 by UK dermatologists Dr. Adrian Ive and Dr. Ronnie Marks21. They noticed patients with skin conditions resembling eczema, rosacea, and psoriasis that didn’t respond to standard treatments. In some cases, classic ringworm signs were present22. Further investigation revealed that steroid use had masked the fungal infection, leading to the term “Tinea Incognita23. Some experts suggest “Tinea atypica” as an alternative name24.
Causes
Motives
Although even modest TCSs can induce the illness, the most prevalent cause of Tinea incognito (TI) is the use of topical corticosteroids (TCSs), especially strong ones25. Additionally connected to TI24 include systemic steroids, various immunosuppressants, and topical calcineurin inhibitors26. Although doctors often advise TCSs, their broad availability without a prescriptionresults in self-administration. TCSs can be used under the direction of unqualified quacks or for cosmetic purposes including skin whitening. These steroids can first help with inflammation, but when taken on fungal infections they can momentarily hide the symptoms, which causes more and bigger lesions upon stopping. TI may be misinterpreted as eczema in the absence of a documented history of steroid usage, which could result in more steroid treatment and worsen the condition. TI may also develop as a result of frequent usage of combination creams that contain strong steroids like betamethasone and clotrimazole along with antifungals. Tinea incognito (TI) and the chronicity of superficial fungal infections can be caused by a number of reasons27. The dermatophyte strain's pathogenicity is crucial28; less invasive variants result in milder, persistent dermatitis, whereas more aggressive strains cause pustules and vesicles. Additional elements that may influence the formation of TI include glandular structures, vellus hairs, and anatomical folds close to orifices29. External factors that can affect fungal growth and the inflammatory response include sun exposure, tight clothes, extensive washing, and warm, humid climates30. Fungal infections might sometimes show up atypically at first, prompting the administration of immunosuppressive medications like steroids, which can thereafter cause TI. Antifungal resistance can make diagnosis and therapy more difficult31. Fungal cultures can occasionally produce poor results, which leads to poor management and the use of immunosuppressants. Numerous fungal species, including anthropophilic (like Trichophyton rubrum), geophilic (like Microsporum gypseum), and zoophilic (like Trichophyton verrucosum) species, have been connected to TI32.
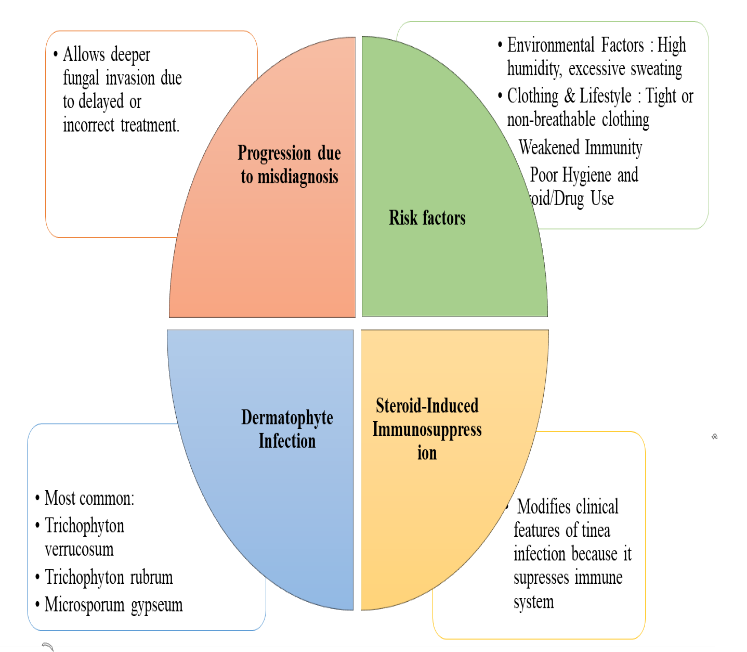
Fig-1:
Epidemiology
Because of underreporting and misinterpretation, the epidemiology of TI, which makes up around 40% of dermatophytosis, is still poorly understood33. Initially documented in 1968, the number of cases has increased recently, with tropical and subtropical countries having a higher prevalence because of the warm, humid climate34. All ages and genders are affected, although several studies have found that children are diagnosed with the disorder more often35. males are more likely to get infected, and people with diabetes mellitus or weakened immune systems are more vulnerable36, especially to onychomycosis and tinea pedis. Because of their restricted use, calcineurin inhibitors are less harmful; yet, the incidence of TI has grown due to the growing use of topical corticosteroids. Furthermore, the risk of infection is increased by elements including excessive sweating, skin abrasion, and unsanitary living conditions.
Pathogenesis
1. Initial Dermatophyte Infection
2. Normal Host Immune Response
3. Misdiagnosis and Corticosteroid Use
4. Immunosuppression Alters Fungal Growth
5. Progression to Severe Infection
The mechanism of topical or systemic glucocorticoids on tinea infection may relate to its effects on the immune system. Field, H. We should feel comfortable using topical or systemic glucocorticoids without concern for tinea infections. These corticosteroids target antigen-presenting (APCs), inhibiting IL-12 production and decreasing MHC-II expression. Corticosteroids enhance the secretion of cytokines such as IL-6, IL-10 and TNF-α by dendritic cells through TLR2 activation, which, in turn, suppresses Th1 cell activation. This migrates the immune response from a Th1 dominant reaction to a Th-2 dominant reaction. Corticosteroids also inhibit IL-12 receptor expression in T cells and NK cells and block IL-12 production. IL-12 can inhibit TH17 cell differentiation and function via inhibited IL-23, IL-6 and IL-17 secretion. Additionally, corticosteroids upregulate the production of cytokines with anti-inflammatory actions, such as IL-4, IL-10, and IL-13, while downregulating the activity of proinflammatory cytokines (IL-1β and TNF-α). Finally, corticosteroids reduce the recruitment of macrophages and neutrophils and inhibit the release of IL-1 and IFN-γ by macrophages. This immune suppression makes it easier for fungal infections like tinea to spread and become more severe.
Clinical Manifestation of TineaIncognio
Because tinea incognito presents clinically differently from other dermatophyte diseases, it can be difficult for medical professionals to make an appropriate diagnosis without a thorough patient history.
Clinical Manifestations:
Symptoms of tinea incognito (TI) are different from those of common dermatophyte infections, which manifest as distinct, ring-shaped, scaly lesions. Rather, TI presents as broad, poorly defined erythematous or hyperpigmented areas that frequently resemble dermatitis or eczema. Because the characteristic annular pattern associated with typical tinea infections is usually absent and scaling may be mild or nonexistent, TI is more difficult to diagnose and is frequently mistaken for other inflammatory skin disorders.
Lesions and Spread
As TI progresses, the patches may form and appear on other body parts, often imitating other skin conditions. The scalp, limbs, face, and trunk are frequently affected. When the infection is treated with steroids or immunosuppressants, the redness, itching, and scaling may disappear, making the infection seem less severe. Because the typical symptoms of a fungal infection become less noticeable, the infection may go undetected, delaying detection.
Vesicles and Pustules
Pustules or vesicles, which are unusual in ordinary tinea infections, can form in tinea incognito, particularly when aggressive fungal strains or steroid use are involved. Diagnosing these fluid-filled lesions can be difficult since they can resemble impetigo, acne, or folliculitis. Discomfort grows with their severity, making identification more difficult and perhaps resulting in a misdiagnosis.
Clinical Manifestations and Associated Complications
vesicles, which are uncommon in common tinea infections Diagnosing these fluid-filled lesions can be difficult since they may resemble impetigo, acne, or folliculitis. The discomfort grows with their severity, making When strong fungal strains or steroid usage are implicated, tinea incognito can develop pustules or identification more difficult and sometimes resulting in a misdiagnosis.
Misdiagnosis And Diagnostic Challenges
Since tinea incognito frequently mimics psoriasis or eczema, it can be difficult to diagnose, particularly in the absence of a history of steroid use. The infection may progress as a result of a misdiagnosis and ongoing steroid treatment. Since TI doesn't have obvious clinical symptoms like other fungal infections, treatment is delayed. Although they are helpful, diagnostic procedures like fungal cultures and KOH microscopy aren't always definitive. Its look can be further changed by elements including dampness, frequent washing, and tight clothing, which makes diagnosis more difficult.
Differential diagnosis
It's important to recognize tinea incognito because it can mimic other skin disorders. Since steroids often help eczema, TI might be suspected if symptoms worsen instead. Unlike TI, which can manifest asymmetrically with steroid usage, rosacea usually appears with symmetrical pustules, whereas lupus, psoriasis, and granuloma annulare have unique characteristics that aid in their differentiation. The most accurate diagnostic method is fungus culture, however it takes time. KOH microscopy or a skin biopsy are quicker alternatives. Although they require specific knowledge, newer instruments such as handheld confocal microscopy provide non-invasive detection.
Treatment:
Stopping topical steroids or other immunosuppressive medications is usually the first step in managing this illness since it enables the immune system to react properly. Using the right antifungal medication to treat the underlying fungal infection is another aspect of proper treatment.
Non-pharmacological therapy
They are being advised to wash their clothes in hot water, wear loose and breathable cotton clothing and to iron their garments before wearing. They also shouldn’t share personal items, such as clothing, footwear, towels and bed linens, to decrease the risk for fungal transmission35. Anticholinergics with topical administration or salts of aluminum serve hyperhidrosis by their excessive sweating.
Pharmacological treatment
Depending on the type of fungus causing the infection and its severity and extent, treatment options may involve Topical or Oral antifungals, or a combination of both. To prevent resistance several antifungal groups should be combined.
Topical antifungals: Miconazole clotrimazole, ketoconazole, and terbinafine are imidazole-based treatments that should be applied twice daily for two to four weeks in mild instances34.
Oral antifungals: Systemic antifungal medication is often required in cases of more severe or resistant infections, however standard antifungal treatment should be given. Depending on the severity and clinical response, oral antifungal drugs such itraconazole or Terbinafine (250 mg daily) may be needed for two to four weeks if the rash is extensive or inflammatory.33. To relieve associated symptoms such as itching, bland antipruritic lotions can be used. in cases where the infection has become more extensive. While many cases resolve within two weeks, more severe or widespread infections may require an extended treatment period of up to three to four months. Ultimately, effective management of tinea incognito involves stopping immunosuppressive therapies and initiating antifungal treatment, selecting either topical or systemic options based on the severity and extent of the condition.
CONCLUSION:
Tinea incognito (TI) often presents with unusual and variable symptoms, making it challenging to diagnose and treat32. The lesions may not resemble typical fungal infections, and the use of topical steroids or immunosuppressive drugs can make the skin more fragile, increasing the risk of injury or secondary bacterial infections. Misdiagnosis can delay treatment, leading to complications and higher healthcare costs. Therefore, TI requires a high level of suspicion, and diagnostic tests such as skin scrapings or cultures may be needed to confirm the infection. Early diagnosis is essential for preventing the spread of infection and ensuring effective antifungal treatment.
REFERENCES




Dr. D. Krishna Priyanka*, Joanna Grace Pullagura, D. Gayathri, SK. Asfiya Sharmeen, D. V. Krishna Reddy, Tinea Incognito: A Comprehensive Review of Steroid-Modified Dermatophytosis and Its Pharmacotherapeutic Challenges, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 4, 2257-2265 https://doi.org/10.5281/zenodo.15239339
 10.5281/zenodo.15239339
10.5281/zenodo.15239339