
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmacology, SET’s College of Pharmacy, Dharwad, Karnataka - 580002.
Gout, also known as gouty arthritis, is a chronic inflammatory disease marked by the buildup of monosodium urate crystals in joints as a result of hyperuricemia, or increased serum uric acid levels. Gout, which was formerly thought of as a "disease of kings," is now understood to be a common metabolic ailment that is becoming more commonplace globally, especially as a result of contemporary lifestyle variables like poor food, obesity, and sedentary behavior. The pathogenesis, clinical characteristics, preventative measures, and developing treatment approaches of gouty arthritis are all examined in this review. Uric acid metabolism and the inflammatory cascade brought on by urate crystal deposition are covered in the first section of the review. Risk factors are investigated, including dietary variables, comorbidities like diabetes and hypertension, and genetic predisposition. The article focuses on clinical diagnosis, including symptomatology, test results, and imaging, to distinguish between acute and chronic tophaceous gout. Current treatment options include pharmacological medications like NSAIDs, colchicine, corticosteroids, and uric acid-lowering pharmaceuticals like allopurinol and febuxostat, as well as non-pharmacological strategies including dietary changes, weight management, and hydration. Early intervention and patient education are key preventive treatments, particularly for at-risk populations.
Gout, a chronic inflammatory condition of the joints, has been known for centuries. Previously, gout was considered a harmless illness caused by excessive eating or alcohol consumption. Subsequent study confirmed that it is a metabolic disease caused by urate crystal deposits in the kidney, joints, skin, and other tissues1. Gout is caused by hyperproteinaemia, or an excess of uric acid in the body, which is influenced by metabolic, genetic, and environmental variables. Localized uric acid saturation occurs when monosodium urate (MSU) crystal precipitates and gout develop in particular bodily areas, usually the joint. Gout is characterized by recurrent episodes, which result in acute arthritic symptoms2. Chronic uncontrolled gout contributes to progressive joint damage, disability, and reduced quality of life. In addition, hyperuricemia has been associated with increased cardiovascular risk, metabolic syndrome, and renal impairment, underlining its significance as a systemic disorder3. Gout epidemiology varies significantly with sex, age, ethnicity, and lifestyle. Men are disproportionately impacted, especially beyond the age of 40, but women are relatively unaffected until menopause, when lowering estrogen levels diminish uric acid excretion4. Certain ethnic groups, such as those from the Pacific Islands, have the greatest prevalence rates of up to 10%, compared to less than 1% in other Asian communities. Lifestyle considerations also play an important impact. Diets high in purine-rich foods like red meat and seafood, combined with alcohol and fructose-sweetened beverages, dramatically increase the risk of gout. Rising obesity rates, older populations, and widespread metabolic problems have all contributed to the global increase in gout incidence4. Even with its widespread recognition, gout still presents difficulties in diagnosis and treatment. Disease progression and a lower quality of life are caused by misdiagnosis, inadequate therapy, and noncompliance with long-term management techniques. The management landscape has changed, providing more efficient and customized care options due to recent advancements in pharmacological therapies, including new urate-lowering medicines, and a rising emphasis on lifestyle changes. In order to inform clinical practice and future research, this review attempts to give a thorough overview of the underlying mechanisms, clinical characteristics, diagnostic complexity, and changing management options of gout. RISK FACTORS: Alcohol, meat, fruit juice, shellfish, and sweetened corn syrup with high fructose corn content all promote DNA growth 5-6. Nuts, oatmeal, asparagus, lentils, and mushrooms7.
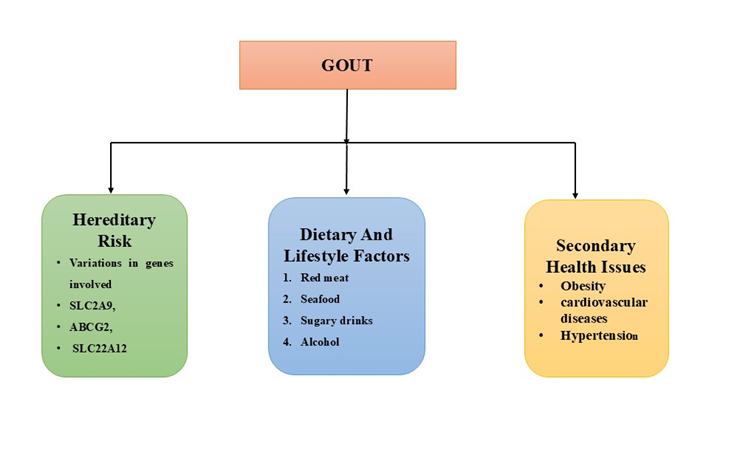
FIG NO :1 Illustration showing key risk factors contributing to gout.
PATHOPHYSIOLOGY OF GOUT:
Gout is a metabolic condition characterized by the deposition of monosodium urate (MSU) crystals in joints and soft tissues as a result of chronic hyperuricemia, which is commonly defined as serum urate levels greater than 6.8 mg/dL. The ultimate product of purine metabolism is uric acid, which can accumulate due to excessive synthesis, reduced renal excretion, or both8. When uric acid concentrations rise above the solubility threshold, MSU crystals form and deposit in synovial fluid and surrounding tissues. These crystals produce a strong inflammatory reaction. Macrophages internalize MSU crystals and activate the NLRP3 inflammasome, which releases pro-inflammatory cytokines such as IL-1β and TNF-α. This cascade activates neutrophils and causes acute joint inflammation, which appears clinically as abrupt, intense pain, swelling, and erythema. Tophaceous gout, which is characterized by the development of tophi—aggregates of MSU crystals encircled by granulomatous inflammation—can result from persistent and frequent flare-ups of gout. Bone degradation, joint deformity, and functional impairment are all exacerbated by these deposits. Furthermore, concomitant conditions like hypertension, chronic renal disease, and cardiovascular illnesses are linked to persistent hyperuricemia2. The development of gout is also influenced by genetic predispositions. Serum urate levels and renal urate transport are impacted by variations in genes such as SLC2A9 and ABCG2. Purine- rich meals, alcohol consumption, and obesity are examples of environmental factors that worsen hyperuricemia and raise the chance of developing gout9.
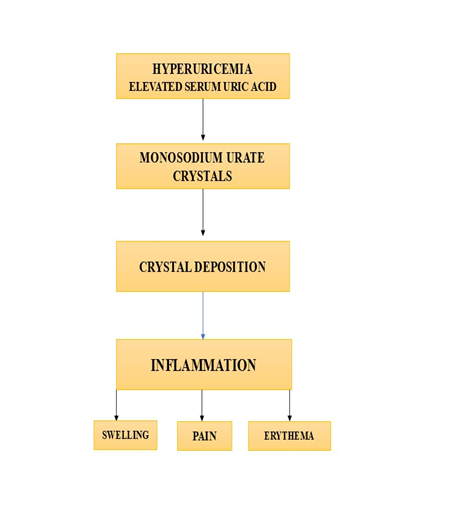
FIG NO :2 Pathogenesis of Gout
Symptoms and indicators
Intercritical gout is a surprisingly silent period that occurs in between the flaming flare-ups of acute gout. The storm appears to have passed during this asymptomatic period, but the threat subtly persists. Patients may feel completely fine at this time and show no outward symptoms of inflammation. However, monosodium urate crystals are still silently building up in the joints beneath the surface, preparing the way for more flares. Acute gout attacks are easily recognized by their high fever, leukocytosis, and skin discoloration surrounding the injured joint, which can be difficult to diagnose because they frequently resemble cellulitis. The metatarsophalangeal joint, which is traditionally referred to as podagra, is usually the focus of the initial blow. A flare is characterized by severe pain, dramatic swelling, and possibly red, glossy skin. However, once the flare has subsided, the body enters a calm. This intercritical phase could extend weeks, months, or even years. Some see it as a temporary respite, while others see it as an extended period of silence. However, the sickness is not idle. Without correct therapy, these quiet intervals shorten with time, and attacks become more frequent, severe, and extensive, eventually leading to chronic tophaceous gout, which is characterized by joint injury and persistent inflammation10.
Clinical Features and Diagnosis:
Gout is an inflammatory arthritis caused by the deposition of monosodium urate crystals in joints and soft tissues due to persistent hyperuricemia. It is becoming more common. A correct diagnosis and understanding of the clinical range are crucial for optimal prevention and management 11.
Hyperuricaemia acute
Asymptomatic hyperuricaemia is the first sign of gout, which develops into four stages. When evaluating SUA (serum level larger than 7 mg/dL), people are usually discovered inadvertently at this point, when they don't exhibit any symptoms or indicators. However, certain patients with hyperuricaemia may experience acute gout attacks 12.
Acute gout attack
Acute gout attacks typically occur in monoarthritic joints and involve intense inflammation, including redness, heat, discomfort, swelling, and loss of function. Skin signs are uncommon in major joints such as the knees and ankles, although pain and swelling can be severe. The following joints may be affected: tarsal and metatarsal joints, ankles, knees, wrists, MCPs, and interphalangeal joints of the hands. Arthritis can affect multiple joints simultaneously. MSU crystals can cause septic arthritis in a gouty joint, hence addressing such patients requires extreme caution. However, mild gout attacks with low-grade inflammation are possible 13.
Intercritical Gout
Intercritical Gout refers to the symptom-free interval between bouts. Although the joint appears normal, urate crystals can induce subsequent attacks if not controlled13.
Chronic Tophaceous Gout
The illness progresses to joint deterioration and palpable tophi if treatment is not received. A tophus is a mass composed of several crystals that have been gathered. It happens when untreated chronic gout persists. It could be present in the subcutaneous tissue, the epidermis, or the area surrounding the ear joints. It is a sign of chronicity and uncontrolled sickness. On a macroscopic level, tophi include a white, chalky material. Tophi can cause joint injury and deformity14.
Stage of Gout
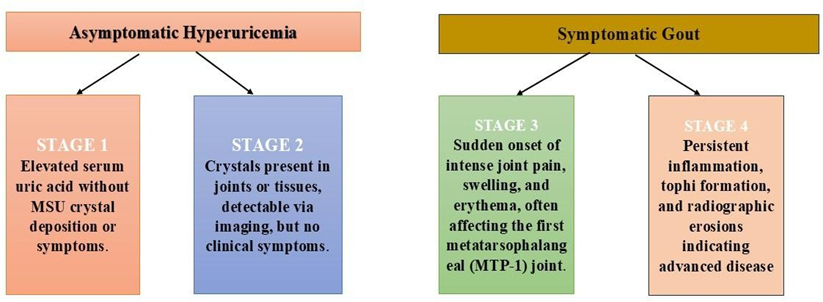
FIG NO 3 STAGES OF GOUT
Treatment for gout
Gout treatment is based on two basic pillars: non-pharmacological and pharmacological therapies. The choice and intensity of these methods are determined by the patient's clinical stage acute, intercritical, or chronic as well as individual characteristics like flare frequency, radiographic abnormalities, and concomitant risk profiles.
Non-pharmacological therapies for gout management
Nonpharmacological management relies heavily on patient education. Sedentary lifestyles and obesity are closely linked to higher serum uric acid levels and an increased risk of gout flares. Cohort studies show that patients who receive organized education on dietary choices, physical activity, and hydration have much better management of blood urate levels and a lower flare frequency.
Uric acid levels are affected by diet. Dietary and lifestyle modifications can reduce uric acid levels by up to 18%15.
Pharmacological therapy
Acute gout flares usually affect the first metatarsophalangeal joint and are characterized by abrupt, severe joint pain, swelling, and inflammation. In order to alleviate symptoms and avoid complications, prompt treatment is crucial. Rapidly reducing joint inflammation and removing discomfort are the goals of pharmaceutical treatment for acute bottom. If medication is not administered, the species flare takes three days to two weeks. Generally speaking, anti-inflammatory medications have to be started as soon as feasible, preferably within 12 to 24 hours of the bottom's severe flare-up.
Table no 1: drugs used for acute gout treatment
|
Drug |
Dose |
Adverse Effect |
Contraindication |
|
NSAIDs (e.g., Indomethacin) |
50 mg three times per day |
Nephropathy, GI irritation |
End-stage renal disease (ESRD), peptic ulcer |
|
Colchicine |
1.2 mg initially 0.6 mg after 1 hr 0.6 -1.2 mg/day |
GI symptoms Nausea, vomiting, diarrhea |
Server renal /hepatic impairment, CYP3A4/P- gp inhibitors |
|
corticosteroids |
30-35 mg daily |
Cushing syndrome, increased HCl secretion hyperglycaemia |
Hepatic failure Uncontrolled diabetes |
B. Treatment for chronic gout17-18
Reversing TOPHUS formation, eliminating any urate deposits, and stopping the growth of DNA and outbursts should be the main goals of treatment for chronic DNA. International guidelines advise lowering uric acid levels to much below the solubility limit of 6.8 mg/dl in order to prevent deposits.
Table No 2: Drug used for chronic gout
|
Drug |
Dose |
Adverse Effect |
Contraindication |
|
Xanthine oxidase inhibitors: Allopurinol |
Initially 50 to 100 mg/ day; increase to max. 800 mg/day |
Diarrhea, Nausea, Vomiting |
Known hypersensitivity to allopurinol |
|
Febuxostat |
Initially 80 mg/day, increase to 120 mg/day if necessary |
Diarrhea, Hepatic dysfunction, headache |
Contraindicated in patients receiving azathioprine (Imuran) and mercaptopurine |
|
Probenecid |
250 mg two times per day initially; titrate up to 2 g per day |
Irritation of gastrointestinal tract, Allergy to skin, anorexia |
Renal failure |
Future Prospects of Gout Management
Advances in diagnostic imaging, next generation treatments, precision medicine, precision medicine and preventative measures hold great promise for the management of gout in the future. When combined this development could less the burden of disease, maximize treatment.
Better Instruments for diagnostics
Recent developments in imaging, especially dual-energy computed tomography (DECT), have revolutionized non-invasive urate crystal deposition detection. Even in the earliest stages, DECT provides great sensitivity and specificity for the detection of monosodium urate crystals and corresponds with the severity of the disease and flare risk in the future. DECT can also stratify prognosis, track therapy response, and measure tophus burden. This method is becoming more widely accepted as an adjunct to conventional clinical evaluation.
Advanced Drugs:
New drugs may more successfully and with fewer adverse effects target inflammation and the generation of uric acid. For example, medications such as pegloti case and febuxostat show promise for people who don't react well to conventional treatments (like allopurinol).
Genetic and Precision Medicine:
Developments in genomics and genetics are illuminating the ways in which certain gene variants impact the metabolism of uric acid. This could result in individualised therapies that are more successful and have fewer adverse effects by being based ona patient's genetic profile.
Lifestyle and Preventive Approaches:
Preventive care is becoming more important as people become more aware of the lifestyle factors (such as nutrition and weight control) that contribute to gout. This could lessen the Like lihood of consequences like kidney stones or joint damage, lessen the frequency of gout attacks, and require fewer drugs.
CONCLUSION
Gout is a significant health concern despite its well-established aetiology and risk factors. Numerous risk factors, including hyperuricemia, genetics, diet, alcohol use, metabolic syndrome (which includes obesity and hypertension), diuretic use, and renal disease, have now been identified by prospective epidemiological studies as contributing to the development of gout in both men and women. The prevalence of chronic gout is expected to continue increasing due to increased obesity rates, an ageing population overall, and an increase in associated comorbidities. Long-term disease outcomes for chronic gout seem to be improved by newer research and guidelines on the significance of careful disease monitoring and efficient intervention to reach appropriate serum uric acid targets, as well as new pharmacologic treatment options, particularly in patients who are resistant to conventional therapy. There is an urgent need to reduce exposure to risk factors, raise awareness, implement strong preventative measures, alter lifestyle, identify indicators for early diagnosis, and create optimal treatment plans and policies in order to reduce the global health burden and enhance patient quality of life.
ACKNOWLEDGEMENT
The authors are sincerely thankful to the Institute of SET`S College of Pharmacy, Dharwad for providing the necessary infrastructure and academic support throughout the course of this research. We express our heartfelt gratitude to the principal, our research guide, and the dedicated faculty and group members of the Department of Pharmacology for their invaluable guidance and encouragement during the preparation of this manuscript. We also extend our deepest appreciation to our families for their unwavering support, patience, and motivation throughout this journey.
REFERENCE


Patil Arati S.*, Preeti V. Kulkarni, Understanding Gout: Mechanism, Clinical Presentation, and Therapeutic Strategies, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 3618-3625 https://doi.org/10.5281/zenodo.17231663
 10.5281/zenodo.17231663
10.5281/zenodo.17231663