
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
NRI College of Pharmacy, Pothavarappadu, Agiripalli, Eluru.
Pneumonia is a serious lung infection that remains a significant global health issue, claiming nearly 4 million lives each year. One of the most concerning pathogens in this context is Acinetobacter baumannii, which has gained notoriety as a multidrug-resistant organism. This bacterium is often associated with pneumonia acquired in hospitals and those linked to ventilators. The patterns of resistance it exhibits complicate treatment options, underscoring the urgent need for new therapies to enhance patient outcomes. One exciting possibility is Zosurabalpin, a groundbreaking experimental antibiotic currently being studied. This first-of-its-kind drug is part of the macrolide-derived antimicrobial family and works through a distinctive mechanism. It specifically targets the LptB2FGC complex, a protein system that helps transport lipopolysaccharide across the outer membrane of Gram-negative bacteria. By blocking this transport pathway, Zosurabalpin disrupts membrane formation and leads to bacterial death. Its bactericidal effects are particularly potent against carbapenem-resistant A. baumannii, a pathogen for which treatment options are limited. From a pharmacological standpoint, Zosurabalpin shows promising safety and tolerability in both preclinical and early clinical trials. While mild elevations in liver enzymes have been noted, which suggests the need for monitoring liver function, it’s also important to assess renal function in patients with reduced clearance. The most frequently reported side effects include gastrointestinal issues like nausea, vomiting, and diarrhea, but the drug appears to have minimal effects on the central nervous and cardiovascular systems. Its pharmacokinetic profile indicates that it is administered intravenously, metabolized in the liver, and excreted through the kidneys.
DEFINITION: An infection of the lung parenchyma is known as pneumonia. Health care providers need to keep in mind that pneumonia is an umbrella term for a collection of illnesses brought on by a number of syndromes caused by a variety of organisms resulting in varied manifestations and sequelae[1].
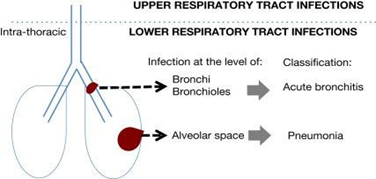
Fig 1: Schematic representation of pneumonia
EPIDEMOLOGY
Approximately 450 million individuals worldwide are affected by pneumonea annually, which is a prevalent respiratory infection[2]. The highest rates are found in children under five and adults over 75 years old. In the developed world, it is almost five times more prevalent than in the developing world [3].Despite being responsible for the death of more than 4 million people each year, pneumonia still remains a significant factor in global mortality, with over half (4.7 million) affected individuals[4,5].
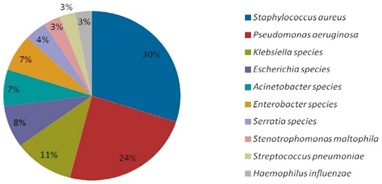
Fig2: Epidemology of Pneumonia
CLASSIFICATION
DRUG PROFILE
Generic name:- Zosurabalpin
Dosage form:- Parentral(I.V)
Drug class:-Macrolide Antibiotic
Category:-Anti-Pneumonia
Structure:-
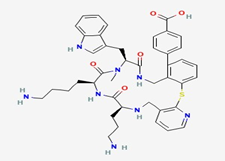
IUPAC Name: -4-[(11S,14S,17S)-14-(4-aminobutyl)-11-(3-aminopropyl)-17(1H-indol-3-methyl)-16-methyl-12,15,18-trioxo-2-thio 4,10,13,16,19pentazatricyclo[19.4.0.03,8]pentacosa-1(25),3(8),4,6,21,23-hexaen-22yl]benzoic acid.
Molecular formula:- C43H50N8O5S
Molecular Weight:- 791.0 g/mol
Background:- Zosurabalpin belongs to the macrolide class, but its unique characteristics make it a distinct antimicrobial. In contrast to traditional antibiotics, it operates in a distinct manner. Consider bacteria as miniature fortifications surrounded by an outer wall. Zosurabalpin targets this wall, which hinders the construction of lypo-polysacharides (LPS), making them susceptible to infection and death without proper LPS shielding. The clinical trials of Zosurabalpin are currently being conducted to evaluate its safety and effectiveness in humans, but it must be monitored for long-term effectiveness to prevent the development of future resistance.
Pharmacodynamics:
The mechanism of action of Zosurabalpin, a novel antibiotic that uses macrocyclic peptides, is unique in its ability to combat Carbapenem-resistant Acinetobacter baumannii (CRAB).By targeting the LptB2FG complex, it hinders the delivery of lipopolysaccharide (LPS) and causes the accumulation of toxic LPS, leading to bacterial cell death.The target of Lipid lipoprotein D (LptD) is the transport protein.
Action:- Bactericidal (kills bacteria). A narrow spectrum is present in the vicinity of Gram-negative bacteria, particularly baumannii time or Concentration-Dependent. Appears to have concentration-dependent killing[6].
Resistance Mechanism:- Understanding traditional resistance pathways (deficient in –lactamases) but susceptible to their effects. The prolonged suppression of bacteria after antibiotics, despite decreasing drug levels, is demonstrated by the Post-antibiotic effect (PAE).
Mechanism of Action (MOA)
Zosurabalpin is a novel antibiotic that works by inhibiting the transport of Lipopolysaccharide (LPS) in Gram-negative bacteria, specifically targeting theLptB2FGC complex. This blockage prevents LPS from reaching the bacterial outer membrane, causing it to accumulate inside the cell and ultimately leading to bacterial death [7,8].
Zosurabalpin administered systemically (e.g., IV)
↓
Drug reaches Gram-negative bacterial infection site
↓
Zosurabalpin targets the LptB2FGC complex
↓
Inhibition of Lpt (Lipopolysaccharide Transport) pathway
↓
Blocks transport of Lipopolysaccharide (LPS) from inner membrane to outer membrane
↓
Disruption of outer membrane biogenesis
↓
Loss of outer membrane integrity in Gram-negative bacteria
↓
Increased susceptibility to host immune response and other antimicrobials
↓
Cell death due to membrane destabilization
↓
Antibacterial effect achieved
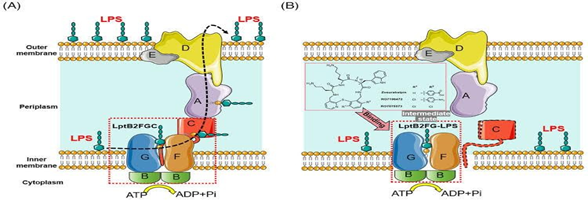
Fig3:Mechanism of Zosurobalpin
PHARMACOLOGICAL ACTIONS
The first-in-class antibiotic against Acinetobacter baumannii, specifically MDR and CRAB strains, is Zosurabalpin. By inhibiting the LptD protein, which is essential for the biogenesis of Gram-negative bacteria's outer membrane, it functions. This action disrupts the transport of lipopolysaccharides (LPS), resulting in the death of bacteria. Despite its primary pharmacological effect being antibacterial, zosurabalpin may have secondary effects on human organs due to off-target interactions, metabolic burden, or toxicological pathways observed in preclinical and early clinical studies.
Liver (Hepatic System):
Kidneys (Renal System):
Pharmacological Action: Zosurabalpin excretes in part via the kidneys. The pharmacokinetics of renal dysfunction may be modified. A few individuals have demonstrated slight elevations in serum creatinine due to organ effects. There was no evidence of nephrotoxicity in early-phase human trials, but animal studies indicated possible renal tubular changes at high doses. Monitor renal function (creatinine, BUN) by adjusting the dose in cases of moderate to severe renal impairment as part of clinical consideration.
Gastrointestinal Tract:
Central Nervous System (CNS):
The blood-brain barrier (BBB) doesn't allow for great penetration, making it less than ideal for treating CNS infections. Preclinical tests show no signs of neurotoxicity.
Lungs :
Therapeutic levels can be reached in pulmonary infections, especially in cases of ventilator-associated pneumonia (VAP). It works well against respiratory pathogens like A. baumannii.
Cardiovascular System :
There have been no observations of QT prolongation or significant cardiac toxicity. The hemodynamic profile remains stable in preclinical trials.
Hematologic System :
No major effects on bone marrow or blood cell production have been noted. So far, there have been no significant cases of anemia, leukopenia, or thrombocytopenia reported.
PHARMACOKINETICS:
1. Absorption:
The chemical characteristics of Zosurabalpin would dictate its absorption. Intravenous administration, taking into account patient-specific factors such as gastrointestinal health.
2. Distribution:
The distribution of Zosurabalpin would be affected by factors such as capillary permeability, blood flow, and protein binding .Antibiotics that are soluble in water and do not cause inflammation tend to be more readily available.
3. Metabolism:
As with most drugs, Zosurabalpin's metabolism likely would occur in the liver through certain enzymes, such as cytochrome P450, which would convert it into more water-soluble metabolites for easier removal from the body.
4. Excretion:
The primary mode of excretion for Zosurabalpin is likely urine, with the potential for it to be expelled through other means like bile and faeces.
The experimental antibiotic Zosurabalpin is being developed to combat infections caused by carbapenem-resistant Acinetobacter baumannii (CRAB). Although there are no detailed contraindications available in zosurabalpin clinical trials, potential precautions and risks are discussed.
Side effects:
Side effects include itching, difficulty breathing, rash and/or low blood pressure. The use of a vein-based tube can result in symptoms such as chills, fever (chicken), nausea, headache, blood pressure problems, fast heart rate, flushing or itching and breathlessness. Side effects, including itchiness, pain, and redness, may occur at the injection site.
REFERENCES

Dr. Garlapati Usha Kiran, Prasanna Thumpati, Siva Gowri Tanuja Ramanadham, Pavithra Gadde, Nandini Rompicharla, Veeranki Meghana, Zosurabalpin as The Primary Focus in Pneumonia Pharmacological Actions, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 116-121. https://doi.org/10.5281/zenodo.17018083
 10.5281/zenodo.17018083
10.5281/zenodo.17018083