Department of Pharmaceutics, KCTs R G Sapkal College of Pharmacy, Anjaneri, Nashik- 422212 (M.S.) India
Due to their incapacity to confine and localize the system at specific parts of the gastrointestinal tract, formulation scientists have faced difficulties in developing oral controlled release systems. A well-characterized dosage form that regulates medication intake into the body within the parameters of the intended release profile has been created using a variety of physical and chemical techniques. The most dependable method for delivering drugs under control is thought to be osmotic pumps. Drug release from ODDS is regulated and not influenced by the dissolution medium's pH or thermodynamics. Drug release from ODDS occurs according to zero order kinetics. Numerous formulation criteria, including solubility, the osmotic pressure of the core components, the size of the delivery orifice, and the type of rate-controlling membrane, affect how quickly a medication releases from an osmotic system. The medicine, osmogens, and excipients are contained in the core of the controlled porosity osmotic pump (CPOP), which is coated with a semipermeable membrane containing water soluble additives. Water soluble additives in CPOP dissolve when they come into contact with water, causing an in situ microporous membrane to develop. This paper provides an overview of osmosis, CPOP, its constituent parts, and its assessment.
Of all the routes investigated for systemic drug delivery via pharmaceutical products with varying dosage forms, oral drug delivery is the one that is most frequently used. Because of its affordability, patient acceptance, and simple administration, the oral route is thought to be the most natural, practical, and safe [1]. The oral route offers the largest active surface area of any drug delivery method when it comes to the administration of different medications [2].
The majority of pharmaceutical products intended for oral administration are traditional drug delivery systems or instant-release types, which are made to release the medication immediately for quick absorption [1]. Therapeutic plasma concentrations fluctuate as a result of conventional dosing patterns, which might occasionally cause noticeable adverse effects. Furthermore, a variety of circumstances can affect the rate and degree of medication absorption from standard dose forms [2]. The excipients employed, the active ingredient's physicochemical characteristics, the gastrointestinal tract's physiology and pH, the rate of stomach emptying, and GI motility are some of the variables that influence how quickly and fully a medication enters the systemic circulation after administration [3].
Uncontrolled rapid drug release can be hazardous to the stomach or the entire body. As a result, different strategies are used when creating formulations to get around the drawbacks of traditional dosage forms, such as the sustained or controlled drug delivery system. Oral, intravenous, and transdermal systems are the three primary categories of controlled-release drug delivery methods. Osmotic pressure is used by oral osmotically controlled release (CR) delivery systems to distribute active drugs in a controlled manner [2]. The release characteristics of drugs from these systems can be controlled by adjusting the qualities of both the drug and the system. The release of the drug is largely independent of pH and other physiological parameters [3].
The net movement of water due to pressure across a selectively permeable membrane is known as osmosis [3]. One of the most sophisticated drug delivery systems is the osmotic drug delivery system (ODDS), which uses osmotic pressure as a propellant to deliver medications in a regulated manner. To keep drug concentration within the therapeutic window, the drug dose and dosing interval in ODDS are optimized [4]. By maintaining plasma concentration within the therapeutic range after absorption, ODDS offers a consistent concentration of the drug at the site of absorption, minimizing adverse effects and lowering the frequency of administration [5]. An osmotic gradient is created and the release of the medication is regulated when water diffuses into the center of an osmotic system through the micro porous membrane. [4]
DEVICES OF OSMOTIC DRUG DELIVERY
The following categories can be applied to osmotic drug delivery systems based on their design and current state of use:
An implantable osmotic pump that distributes drugs to a patient consists of an osmotic engine, a substantially toroidal compartment arranged at least partially around the osmotic engine, and a piston located within the compartment. When the pump is placed in an aqueous environment, the osmotic engine is used to propel the piston through the compartment and discharge the active substance. Implantable osmotic systems include the Rose and Nelson pump, the Higuchi Theeuwes pump, and the Higuchi Leeper pump, while implantable Mini osmotic pumps include the Alzet and Duros Mini osmotic pump [4].
An oral osmotic pump is an osmotic device that delivers an active component into the patient's mouth cavity. The osmotic device consists of a semi-permeable membrane that surrounds a compartment containing an active substance that is insoluble to very soluble in aqueous fluid. The path via the semi-permeable membrane connects the device's exterior to the compartment housing the active agent, which is then delivered from the device into the oral cavity [2]. The oral osmotic pump is categorized as single chamber osmotic pumps, such as the elementary osmotic pump (EOP), multi chamber osmotic pumps, such as the push pull osmotic pump (PPOP), and osmotic pumps with nonexpanding second chambers [4].
A number of osmotic pump systems, including the liquid OROS/liquid oral osmotic system, the osmotic bursting osmotic pump (OBOP), and the controlled porosity osmotic pump (CPOP), have been developed recently. (e.g. L OROS hard cap, L OROS soft cap, delayed liquid bolus delivery system, telescopic capsule, OROS CT, sandwiched osmotic tablets (SOTS), monolithic osmotic system, osmat, multiparticulate delayed release systems (MPDRS), pulsatile delivery via expandable orifice, pulsatile delivery via a series of stops, and lipid osmotic pump.[4]
CONTROLLED POROSITY OSMOTIC TABLET
The core compartment of the controlled porosity osmotic pump tablet is filled with medication and coated in an asymmetric insoluble membrane that contains some water-soluble additives. The membrane only allows water to pass through it selectively. The aqueous environment causes water-soluble additives to dissolve and leak out of the system, causing the membrane to develop micropores that give it a sponge-like texture. The resulting microporous wall is thus permeable to both water and the medication when it is dissolved. Among the pore-formers that are used are urea, sodium chloride, and sorbitol.
Beneficial materials are those that can form 5–95% pores with pore diameters between 10 and 100?m.
Numerous investigations have been carried out to examine the mechanism of drug release in situations where solubility ranges from moderate to high. Additionally, various solubility modulators are being examined. The solubility of the drug in the tablet core, the coating thickness, the amount of leachable pore-forming agent(s), and the osmotic pressure difference across the membrane all affect how quickly drugs escape from a controlled porosity osmotic pump [2]. The medication release rate from this system is dependent on the coating surface area, osmotic pressure, drug solubility, and thickness of the soluble component. On the other hand, neither pH nor physiological circumstances affect this system [3].
ADVANTAGES [1, 4]
DISADVANTAGES [1, 4]
MECHANISM OF DRUG RELEASE
The water soluble additives dissolve and create a microporous structure in the coated membrane when the controlled porosity osmotic pump tablets are in an aqueous environment. The micropores that form in SPM have the potential to be continuous with microporous lamina, connected by winding routes with both regular and irregular geometries [6].
Additives for pore formation with concentrations between 5% and 95% result in pores with sizes between 10A? and 100 lm. Drugs that are water soluble, partially water soluble, and water insoluble can all be treated using this method. When the semi-permeable membrane comes into contact with water, it becomes the shape of a sponge. Water permeates semi-permeable membranes, creating a medication solution that is discharged via the pores. The kind and concentration of osmogent determine the rate of water entry, and the size and quantity of pores as well as the hydrostatic pressure generated by the incoming water determine the release of drugs [7].
Different osmotic pump principles for drug delivery systems employ water as a solvent. For actuation, the solvent flow is delivered by each pump across the semi-permeable membrane. The drug utilized as an osmotic agent dissolves when solvent flows through the membrane into the osmotic device, dislodging the saturated drug solution through outlets. Equation (1) expresses the volume flow of solvent into the core reservoir.
dvdt=AhL(?d?-dp)
dmdt=dvdtC
Where, C is the drug's concentration in the distributed fluid and dm/dt is the solute/drug delivery rate.
The reflection coefficient is taken into account when there is medication leakage via the membrane. When the SPM is perfect, no solute can travel through it, and ? is almost equal to unity. A large enough aperture will result in very little hydrostatic pressure, which eventually approaches nil. Thus, Eq. (1) becomes
dvdt=AhL?d?
Since osmotic pressure in gastrointestinal fluids is much lower than in core, d? is used in place of ?, and a constant K is used in place of L ?. As a result, the equation becomes
dvdt=AhK?
Thus, the drug pumping rate from the core can be represented as follows:
dmdt=AhK?C
This basic formula works for controlled porosity osmotic pump tablets as well as all osmotically driven pumps [4].
IMPORTANT COMPONENTS OF CONTROLLED POROSITY OSMOTIC PUMP TABLETS
Drug
Only this system can be used to design a medication that is naturally water soluble. Drugs with a brief biological half-life (two to six hours), long-acting medications (glipizide, nifedipine, etc.), and extremely powerful medications can be developed for this system [4].
Osmogent
An crucial component of osmotic formulations are osmogenes. They keep the membrane's osmotic gradient intact. Osmogenes dissolve in biological fluid that has entered the osmotic pump through a semipermeable membrane. This causes an increase in osmotic pressure inside the pump and forces medication out of the pump through a delivery orifice. They also help to keep the medicine consistent in the hydrated formulation and provide a driving force for the uptake of water. An osmogene could be a medication that dissolves in water. The choice is made in accordance with the drug's solubility as well as the quantity and pace at which the drug will be released from the pump. Drugs that have minimal solubility will exhibit zero order release, albeit slowly. Osmotic agent is added to the formulation in order to improve the release rate [1].
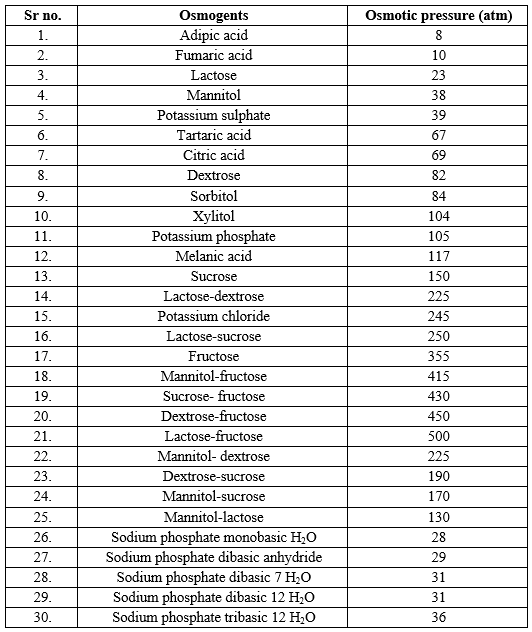
Table no: 1 Osmotic agents with their osmotic pressure [1-4, 13].
Semipermeable membrane (SPM)
Other names for semi-permeable membranes are differentially permeable, partially permeable, and selectively permeable [4]. Solvent and certain chemicals or ions can move through SPM membranes through diffusion or specialized assisted diffusion. SPM is present in CPOP as the outer layer. The medication and other components contained in the compartments cannot travel through the membrane [8].The membrane needs to be stable in the device's internal and external conditions [9]. The membrane is biocompatible with the other chemicals in the formulation and is inert, maintaining its dimensional integrity to provide a steady osmotic pressure during drug administration [8]. The other group of polymers that create SPMs includes polyamides, polyurethanes, cellulose acetate ethyl carbamate, cellulose acetate, and acetaldehyde dimethyl cellulose acetate. For the semi-permeable membrane to resist the pressure inside the device, it is typically 200–300 lm thick.
Ideal properties of Semi- permeable membrane [9]
Coating Solvents
The majority of cellulose acetate is utilized in the creation of different CPOP tablets. Cellulosic polymers such cellulose ethers, cellulose esters, and cellulose ester-ether are involved in the synthesis of SPM. The polymeric solutions that are used to create the osmotic device wall can be made with coating solvents. Both inorganic and organic inert solvents are a part of it. Carbon tetrachloride, water, cyclohexane, methylene chloride, acetone, methanol, ethanol, isopropyl alcohol, butyl alcohol, ethyl acetate, etc. Are among the solvents used for coating solvents [10]. Acetone-methanol (80:20), acetone-ethanol (80:20), acetone-water (90:10), methylene chloride-methanol (79:21), methylene chloride-methanol-water (75:22:3), and other solvent combinations are among them [11].
Emulsifying agents
These work especially well when combined with wall-forming materials. They create an integral composite that is helpful in activating the device's wall. They function by controlling the surface energy of constituents to enhance their assimilation into the composite and preserve their integrity in the drug release milieu. Utilizing self-emulsifying agents, certain patented innovations enable the distribution of liquids from osmotic delivery systems. Typical surfactants have been utilized for this purpose, including polyoxyethylenated glyceryl ricinolate, polyoxyethylenated castor oil with ethylene oxide, glyceryl laureates, and glycerol (sorbiton oleate, stearate, or laurate) [4,8].
Flux regulating agents
The wall-forming materials are mixed with agents that control, enhance, or decrease flow. It helps control the flux's fluid permeability through the wall. The liquid flux can be adjusted in advance by choosing this particular agent. They also make the lamina more porous and flexible. In contrast to hydrophobic materials like phthalates substituted with an alkyl or alkoxy (e.g., diethyl phthalate or dimethoxy ethyl phthalate), hydrophilic substances like polyethethylene glycols (300 to 6000 Da), polyhydric alcohols, polyalkylene glycols, and the like tend to improve the flux. For this aim, materials that are essentially water-impermeable, such as insoluble oxides or salts, can also be employed [12, 13].
Wicking agents
Water can be drawn into the delivery device's porous network by the wicking agent. It is possible for the wicking agent to be swellable or nonswellable. It is capable of going via physisorption with water. Vanderwaal interactions between the wicking agent's surface and the absorbed molecule allow solvent molecules to cling loosely to their surfaces during physisorption, a type of absorption. The purpose of the wicking agent51 is to transport water to the surfaces inside the device's core and form a network or channels with a greater surface area. Wicking agents include sodium lauryl sulphate, bentonite, colloidal silicon dioxide, kaolin, titanium dioxide, alumina, niacinamide, and polyvinyl pyrrolidone [14].
Plasticizers
Plasticizers improve the workability, flexibility, and permeability of the fluids while lowering the temperature of the wall's second order phase transition or elastic modulus. Typically, one hundred parts of wall-forming materials are mixed with 0.001 to 50 parts of a plasticizer or mixture of plasticizers. High solvent power, compatibility with the materials throughout the processing and temperature range, permanence—as evidenced by the materials' strong tendency to stay in the plasticized wall—flexibility, and nontoxicity are all characteristics of suitable solvents. Dibenzyl, dihexyl, or butyl octyl phthalates, triacetin, epoxidized tallate, or tri-isoctyl trimellitate, alkyl adipates, citrates, acetates, propionates, glycolates, myristates, benzoates, and halogenated phenyls are examples of exemplary plasticizers. These plasticizers aid in modulating and achieving the necessary release rate in the design of osmotic controlled release systems [15].
Pore forming agents
When the system operates, the pore-forming chemicals leach into the membrane, creating a microporous structure that is typically utilized for medications that are poorly soluble in water. Prior to the system operating, the pores in the wall might be created by chemical reactions in the polymer solution or by gas production caused by the volatilization of components [4]. Both organic and inorganic materials can be used as pore formers. Alkaline metal salts (sodium chloride, sodium bromide, potassium chloride, potassium sulphate, potassium phosphate, etc.), alkaline earth metals (calcium chloride, calcium nitrate, etc.), and carbohydrates (sucrose, glucose, fructose, mannose, lactose, sorbitol, mannitol, diols, polyols, etc.) are examples of substances that can form pores [15].
Barrier layer formers
Various materials are employed as barrier layers to keep water out of specific areas of the delivery system and to keep the drug layer and osmotic layer apart. Hydrophilic polymers make up the water-permeable covering of a multilayered reservoir. On the other hand, latex compounds like polymethacrylates are used to create layers that are impenetrable to water. Moreover, a barrier layer made mostly of fluid-impermeable substances, such as high-density polyethylene, wax, rubber, and the like, can be positioned between the drug layer and the osmotic composition [13].
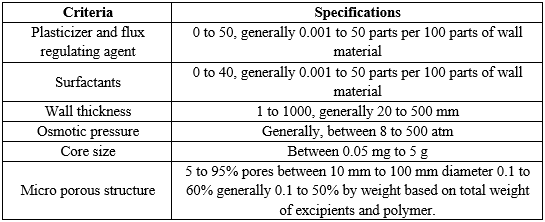
Table no2: Criteria and specifications of controlled porosity osmotic pump [4]
COMPATIBILITY STUDIES
Fourier transform infrared spectroscopy (FTIR)
By examining the notable variations in the form and location of the absorbance bands, the Fourier Transform Infrared (FTIR) approach can be used to highlight the implications of the various functional groups of drugs and excipients. Using this procedure, individual samples and the drug and excipient mixture were completely crushed and mixed with potassium bromide (1:100) for three to five minutes in a mortar. Then, the discs were compacted into discs by applying five tons of pressure for five minutes in a hydraulic press. The pellet was placed in the sample holder and the FTIR spectrophotometer was used to scan it from 4000 to 400 cm1. Then, all sample characteristics and combination characteristics peaks were found. Then, pure medication and excipients were compared to the peaks of the improved formulation. It was deemed compatible if there was no interaction between the drug's peak and the optimized formulation's excipients [16].
Differential scanning calorimetry (DSC)
By employing differential scanning calorimetry, the drug's compatibility with the excipients employed in the formulation development process was evaluated. Drug and specific excipient physical mixes in a 1:1 ratio were prepared and subjected to DSC analysis. In a DSC pan, individual samples and a physical combination of the medication and excipients were weighed to a maximum of 5 mg. The sample pan was scanned in the 50–300 ?C temperature range after being crimped for efficient heat conduction. A 20 ?C min heating rate was employed, and the thermogram that was produced was examined for signs of interaction. Subsequently, the thermograms were contrasted between optimal formulation and pure samples [17].
EVALUATION OF OSMOTIC PUMP TABLETS
Angle of repose (?)
The heap's creation technique has a significant impact on the angle of repose test. Measurements of heap shapes can be used to determine the angle of repose. It is possible to measure the angle of repose using the traditional approach. The following formula is used to determine the powder heap's diameter and angle of repose.
tan?=2h/d
?=tan-1(2h/d)
Where, d is the circular support's diameter in centimeters, h is the heap's height in centimeters, and ? is the angle of repose [18].
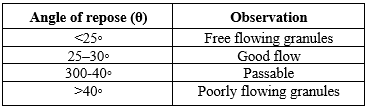
Table 3: Angle of repose and its observations
By positioning an initialization tube on the support with an internal diameter equal to the support diameter, the angle of repose may be precisely monitored. The initialization tube rises at a steady 5 mm/s once the powder sample is manually filled into it. This causes the powder to pour out of the tube and collect in a mound on the cylindrical support. This support slowly revolves on its axis. The heap is captured in images by a CCD camera in various orientations. In order to obtain the outcomes shown in the following Section 8, 22.5? rotationally separated photos were captured. All of the geometrical information was retrieved in this manner. The algorithm determines the location of the powder/air interface by image analysis from each heap picture. The isosceles triangle, whose surface area is equal to that of the heap, has an angle of repose (?). The optimum heap shape is represented by the isosceles triangle [18].
Bulk density (eb)
Pouring the granules into a graduated cylinder allows one to calculate the bulk density. The granules' mass (m) and bulk volume (Vb) are calculated. The following formula [19] is used to determine the bulk density.
Bulk density (eb) = Mass of granules (m)/ Bulk volume of granules (Vb)
Tapped density (et)
For a predetermined amount of time, the measuring cylinder holding a known mass of granule blend is tapped 1000 times. Measurements are made of the mass of the granules (m) and the minimum volume occupied in the cylinder (Vt). The following formula is used to calculate the tapped density [20].
Tapped density (et) = Mass of granules (m)/Tapped volume of granules (Vb)
Compressibility index (Carr’s index)
The flow property properties of the granules generated by Carr are determined by the compressibility index. The potential powder arch and stability can be directly determined by looking at the % compressibility of the granules. The formula [4] can be used to compute the Carr's index.% Compressibility= (Tapped density – Bulk density) / (Tapped density) X 100
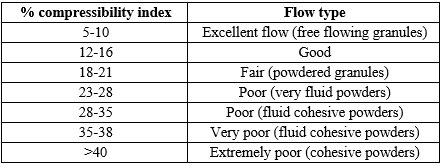
Table 4 : Relationship between powder flowability and % compressibility range.
Hausner’s ratio The granule flow characteristics are determined using Hausner's ratio. The ratio can be computed by dividing the bulk density by the tapped density ratio. As can be shown in Table [17].
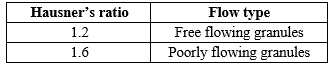
Table 5: Hausner’s ratio and its flow types.
Thickness
A vernier caliper is used to measure the thickness of individual tablets, providing an accurate measurement of thickness. It gives details on how the thickness of osmotic pump pills varies. Typically, mm is used as the measurement unit for thickness. Every tablet has a maximum thickness deviation of ±5% [21].
Hardness
The Monsanto hardness tester may be used to measure tablet hardness, which is expressed in kg/cm2 [22].
Friability
A Roche friabilator was used to test the friability of tablets. After being first weighed (W0) as a group, ten pills were added to the chamber. The tablets experienced the combined impacts of shock and vibration since the plastic chamber containing them dropped them at a distance of six inches with each revolution and abrasion during the 100 revolutions of the friabilator. After that, the pills are weighed again and dusted (W).The following formula was used to determine the percentage of friability.
%Friability=F=(1-WoW)×100
Where, W0 and W are the tablets' pre-test and post-test weights, respectively. The proportion of friability must exceed 0.5% to 1% [23].
Weight variation
To perform the weight variation test, each of the twenty tablets is weighed separately, the average weight is determined, and the weights of each tablet are compared to the average. After calculating the % weight deviation, the results were compared to the USP requirements. If no tablet deviates from the percentage restriction by more than twice and if no tablet differs by more than twice the age limit, then the tablets pass the USP test. Table 6 displays it [24].
Weight variation of nth tablet= (|w-wn|)w×100%
Where, the tablet weights are w1, w2, w3.... wn ...., w20, and the average tablet weight is w
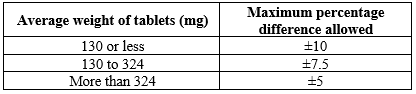
Table:6 USP: specifications for weight variation of tablets.
Disintegration test
In the disintegration test apparatus, the basket rack assembly is placed in a 1-liter beaker of water, simulated gastric fluid, or simulated intestinal fluid at 37 °C±2 °C so that the tablet stays 2.5 cm from the bottom of the beaker. The disintegration time of tablets is then measured by placing tablets in each tube. The basket is moved up and down by a conventional motor at a frequency of 28 to 32 rpm (cycles per minute) over a distance of 5 to 6 cm. If all of the pills break down and the particles pass through the #10 mesh screen in the allotted amount of time, the USP disintegration test will pass [23].
Uniformity of drug content test
Ten dosage units are separately tested for content in this USP method using the procedure outlined in the specific monograph. The standards for content uniformity are satisfied, unless otherwise specified in the monograph, if the standard deviation is less than 6% and the amount of active ingredient in each dosage unit falls between 85 and 115% of the label claim. Additional testing as outlined in the USP are necessary if one or more dosage units do not meet these requirements [25].
In vitro dissolution studies
To conduct an in vitro dissolution investigation, USP Type I apparatus (basket type) is used. The tablet is stored in 900 ml of phosphate buffer buffer with a pH of 7.4, 0.1 N HCl, or simulated gastric fluid. The temperature of the dissolution media is maintained at 37 ± 0.5 ?C using a stirrer that rotates at a set speed. Five milliliters of samples extracted at various intervals were substituted with new medium and subjected to analysis in a UV-visible spectrophotometer to determine absorbance using an appropriate blank solution. Lastly, a suitable equation is used to calculate the drug release rate [26].
Scanning electron microscopy (SEM)
A scanning electron microscope was used to look at studies of surface-coated tablets both before and after dissolving in order to observe the process of drug release from the generated formulations. Membranes were placed between wax paper sheets in a desiccator and dried at 45 °C for 12 hours before being examined. The samples, or membranes, were adhered to a brass stub using double-sided tape, and a sputter coater vacuum-coated them in gold. In a SEM equipped with an ion sputtering apparatus, scans were obtained at an excitation voltage of 20 KV. By comparing the porous morphology of the coated membrane of the optimum formulation film coating before and after dissolution, the porogen and drug release capabilities may be assessed [27].
CONCLUSION
Osmotic pressure provides the push that propels drug release in the Control Porosity Osmotic Pump. The medication exits the system due to an increase in internal pressure brought on by water imbibition. The ability to precisely manage zero-order or other patterned release over an extended period of time is one of the main benefits; consistent release rates may be attained regardless of the environmental conditions at the delivery site. Osmotic systems for controlled delivery also lessen the side-effect profile by reducing the blood plasma peaks that are common in conventional dosage forms (such quick release). Additionally, trough plasma levels can be avoided throughout the dosing period since effective plasma levels are maintained longer in osmotic systems.
REFERENCES





Saba R. Shaikh*, Pradnya Gangurde, Shradha Kandalkar, Kajal Choursiya, Sheetal Gondkar, Rishikesh Bachhav, An Overview on Controlled Porosity Osmotic Tablet, Int. J. of Pharm. Sci., 2024, Vol 2, Issue 5, 1181-1193. https://doi.org/10.5281/zenodo.11245201
 10.5281/zenodo.11245201
10.5281/zenodo.11245201
