Shree Venkateshwara College of Paramedical Sciences, College of Pharmacy, Gobi, Tamil Nadu 638455.
This article provides a comprehensive overview of dapagliflozin and bisoprolol, two pharmacologically distinct drugs used to manage type 2 diabetes, hypertension, and cardiovascular risks. Dapagliflozin, a selective SGLT2 inhibitor, enhances glycemic control by promoting urinary glucose excretion, while bisoprolol, a cardioselective ?1-blocker, reduces blood pressure and cardiac workload. Their combination offers synergistic benefits in patients with coexisting diabetes and cardiovascular diseases. The article explores their chemical profiles, pharmacokinetics, therapeutic uses, contraindications, and adverse effects. Analytical methods including RP-HPLC, IR spectroscopy, TLC, and solubility/melting point studies are discussed, with chromatographic methods optimized for simultaneous estimation. A robust, precise, and validated TLC method, in line with ICH Q2 (R2) guidelines, is proposed for quantitative analysis in bulk and tablet formulations. Forced degradation studies confirm the stability profile of both drugs. This study supports the clinical and analytical potential of dapagliflozin–bisoprolol combinations in therapeutic and pharmaceutical applications.
Dapagliflozin and bisoprolol and medication used to manage different aspects of cardiovascular and metabolic health[1]. Dapagliflozin + bisoprolol contain two ingredients, namely dapagliflozin helps the heart by removing excess salt ( sodium ) and water via urine, reducing its workload. Bisoprolol slows down the heart rate and decreases the force exerted by heart muscles during each beat reducing the amount of energy the heart use, bisoprolol is a beta – blocker that helps to lower the blood pressure and heart rate, while dapagliflozin is a SGLT2 inhibitor that helps to control blood sugar level in type II diabetes[2].
When they are used together it can be treated for hypertension and diabetes [3].Which are often co-occurring condition and contribute to cardiovascular risk. This mediation can provide a synergistic effect for patients with both hypertension, type II diabetes and cardiovascular risk[1][3].
Bisoprolol (chemically aryloxyl propanolamine derivative) chemically,(RS)-1-[4-[[2-(1-methylethoxy)ethoxy]methyl] phenoxy]-3-[(1-methylethyl) aminopropan-2ol.Bisoprolol fumarate is the most potent beta, selective beta blocker.it has highest power of selective beta-activity and by blocking the beta –adrenergic receptor it reduces the heart rate, and contraction of the heart thus lowers the blood pressure. The molecular formula of bisoprolol fumarate C18 H31 NO4 and molecular weight is 325.443g/mol. Bisoprolol available in fumarate salt form, bisoprolol fumarate - (C18 H31 NO4)2 . C4 H4 O4, molecular weight- 767g/mol[3].
The dapagliflozin (DAPA) is a undoable, dynamic and particular inhibitor of sodium-glucose co-transporter2(SGLT2)[3]. Dapagliflozin works by the reabsorption of glucose from the liver, resulting in more glucose excretion in the urine, thereby increasing glycemic control in individual with type- 2 diabetes mellitus, it is defined in chemical terms as[1S]-1,5 anhydro-1-C[4-chloro-3-[(4-ethoxy phenyl methyl)].D-glucoside.This is anethanol, dimethylsulfoxide and dimethyl-formamide soluble white crystalline powder[4].

Fig(1):BISOPROLOL FUMARATE AND DAPAGLIFLOZIN PROPANEDIOL MONOHYDRATE[2].
HISTORY:
Dapagliflozin was discovered at Bristol-Myers Squibb and developed in partnership with AstraZeneca. It was approved by FDA in 2014, and it is marketed in three formulations,
Bisoprolol was developed by the German pharmaceutical company in 1986 by Merck KGaA. And later received approval in many countries around the world, including the US and UK[2].
DISCOVERY AND DEVELOPMENT:
Dapagliflozin, in early 2000s the SGLT2 inhibitor was found to regulate the blood glucose level and particularly for the patient with type II diabetes[3].
Bristol-Myers Squibb and AstraZeneca are two major pharmaceutical companies that were discovered and developed the dapagliflozin[1].
Bisoprolol, is developed by the world health organization list of essential medicines, and available as a generic medication. Bisoprolol was patented in 1986, approved by the medicinal use in the United States in 1992[5].
FDA APPROVED:
Bisoprolol was first approved in 1992 by U.S Food and drug administration [6].
Dapagliflozin was first approved in 2014by U.S Food and drug administration [7].
DRUG PROFILE:
Dapagliflozin is a sodium- glucose-co-transporter -2(SGLT2) inhibitors used in the treatment of patients with type II diabetes. An aryl glycoside with significance effect as glucose-lowering agent, dapagliflozin also has indication for patients with heart failure and chronic kidney disease[7].
CHEMICAL NAME : (1S)-1,5-anhydro-1-C-[4-chloro-3-[(4 ethoxy phenyl ) methyl]- phenyl-1]-D-g1ucitol.
CHEMICAL FORMULA: C21 H25 ClO6.
MOLECULAR WEIGHT: 502.98g/mol.
CHEMICAL STRUCTURE :
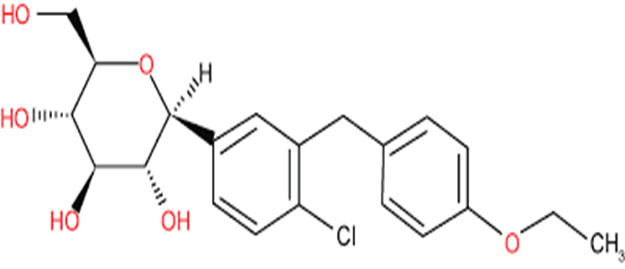
Fig(2): STRUCTURE OF DAPAGLIFLOZIN[7].
PHYSICAL PROPERTIES[2][8]:
USES
ADVERSE EFFECT[8]:
IN VITRO STUDIES: DAPAGLIFLOZIN
ABSORPTION: Dapagliflozin has good oral bioavailability is around 78% and is well absorbed across a wide dose range. while food lower its peak concentration (Cmax) and delay the time to peak (T max), it doesn’t effect the overall drug exposure (AUC) or its glucose -lowering effect therefore food has no clinically significant impact on dapagliflozin efficacy[7].
DISTRIBUTION: Dapagliflozin shows extensive tissue distribution (VSS 118L )and is about 91% protein -bound,with binding unaffected by diabetes or kidney / liver functions.
METABOLISM: Dapagliflozin is mainly metabolized by into glucuronide forms, with the parent drug and its major metabolite making up most of the plasma content. Despite reduced UGT2B7 activity in T2DM,UGTIA9 activity.
ELIMINATION: Dapagliflozin has a half life of about 13 hours and is mainly cleared through urine, with less than 2% excreted unchanged..most of the drugs (96%) is recovered after dosing – 75% in urine and 21% in feces, with some unchanged drug in feces[2][8].
Fig(3):API OF Dapagliflozin
BISOPROLOL:
Bisoprolol is cardio selective β?- adrenergic blocking agent used to treat high blood pressure. It is considered a potent drug with a long- half life that can be used once daily to reduce the need for multiple doses of anti-hypertensive drugs[20].
CHEMICAL NAME: 1-[4-[[2-(1-methyl ethoxy)ethoxy]methyl]phenoxy]-3-[(1-methylethyl)amino]-2-propanol.
CHEMICAL FORMULA: C18 H31 NO4.
MOLECULAR WEIGHT: 325.4 g/mol.
CHEMICAL STRUCTURE:
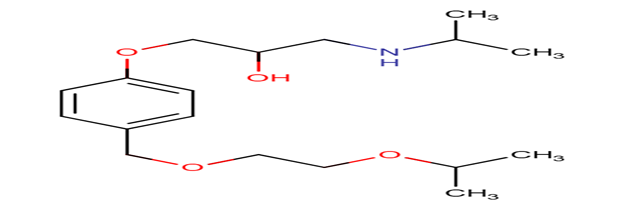
Fig(4):STRUCTURE OF BISOPROLOL[6]
PHYSICAL PROPERTIES [6]:

USES
ADVERSE EFFECTS [8].
INVITRO STUDIES: BISOPROLOL[8][9]
ABSORPTION:
DISTRIBUTION:

METABOLISM:
Primarily metabolized BY CYP3A4/ with minor involvement CYP2D6. No significant impact from CYP2D6 polymorphisms. Approximately 50% undergoes hepatic metabolism to inactive metabolites; low first-pass metabolism (20%).
EXCRETION:
50% excreted unchanged in urine Remaining 50% eliminated as inactive metabolites via kidneys Fecal excretion negligible (<2%).

Fig(5): API OF BISOPROLOL FUMARATE
MECHANISM OF BIOSPROLOL:
BISOPROLOL: Bisoprolol helps to manage high blood pressure mainly by blocking specific receptors in the heart called β1-receptors.These receptors usually respond to stress hormones like adrenaline, which increase heart rate and blood pressure. By blocking them, bisoprolol slows the heart down, reduces how hard it has to work, and lowers its need for oxygen[10]. It also helps by reducing the amount of renin released by the kidneys a hormone that normally raises blood pressure. In addition, bisoprolol may act on the brain to reduce nerve signals that increase blood pressure and heart rate[11].
PHARMACODYNAMICS: Bisoprolol decreases heart rate, decreases contractility and reduces blood pressure. The result of various clinical studies indicate that bisoprolol reduces cardiovascular mortality and all-cause mortality in patient with heart failure and decreased cardiac ejection fraction (EF)[12].
CONTRAINDICATION OF BISOPROLOL:
Bisoprolol, a cardioselective beta -1 blocker,is contraindicated in the following conditions:
THEREAPAUTIC USES [9]:
CONTRAINDICATION OF DAPAGLIFLOZIN [9] [13]:
THERAPEUTIC USES [1] [7]:
ANALYTICAL DEVELOPMENT METHOD:
SELECTION OF WAVELENGTH: Dapagliflozin and bisoprolol were scanned between 200-400 nm against diluents. Absorbance maxima of dapagliflozin &bisoprolol have detected at 270[4]. Chromatogram was taken at 270 nm,both drugs give good peak height and shape. So,270 nm was selected for simultaneous estimation of dapagliflozin & bisoprolol in their formulations[8].
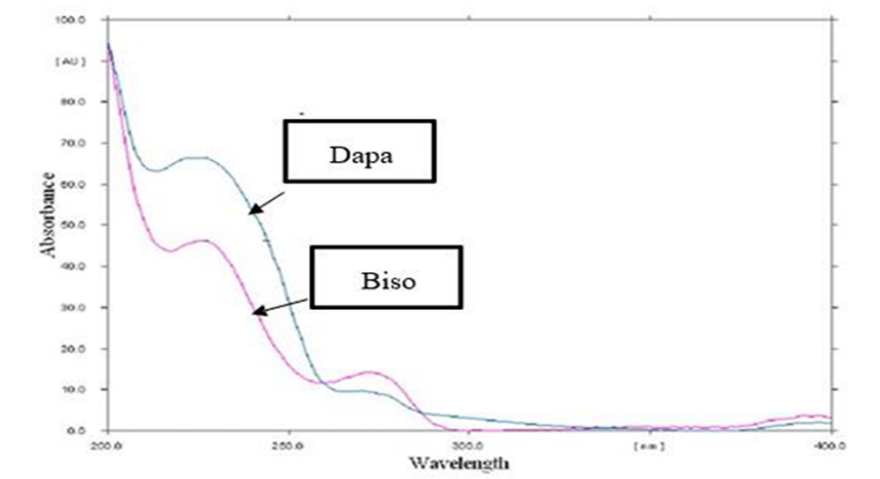
Fig (6): wavelength of dapagliflozin and bisoprolol[8]
SELECTION OF COLUMN:
For RP-HPLC Method, various columns are available but based on literature survey C-18(id4.6 250mm 5 ) was selected over the other columns[15].
SELECTION OF MOBILE PHASE: A mixture of acetonitrile and water in a volume ratio of 75:25 was used as the mobile phase toachieveoptimal separation[8][2].
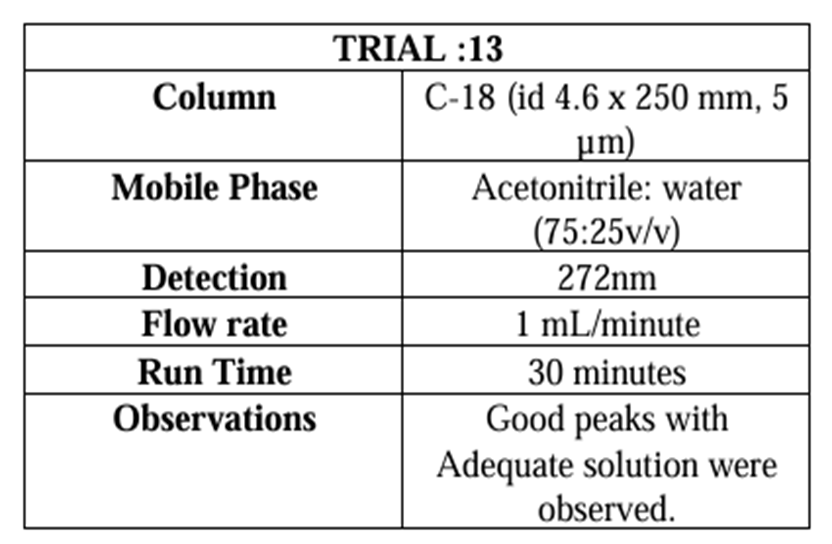
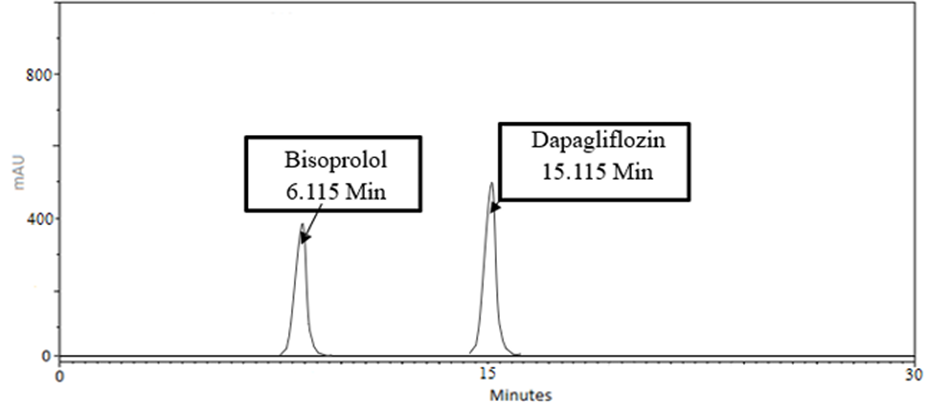
Fig(7): Chromatogram of dapagliflozin and bisoprolol acetonitrile: water(75:25v/v)[15]
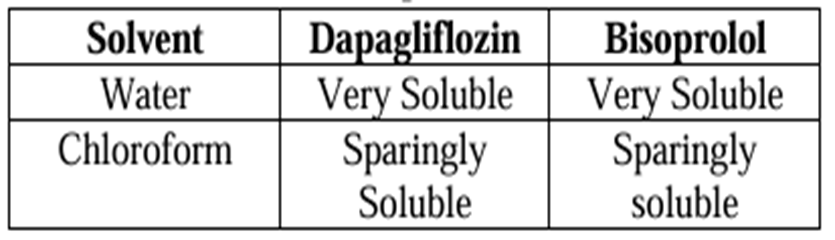
SOLUBILITY:
Accurately weighed 100mg of each drug substance was transferred into 100 ml volumetric flasks. Appropriate amount of solvent was added to each flaskdepending on the study design. flasks were shaken manually or using a mechanical shaker for a few minutes at room temperature to facilitate dissolution[4][8].
MELTING POINT:
Melting point of Dapagliflozin & Bisoprolol hydrochloride has been determined.
The melting points of the compoundswere taken by open capillary method[15][16].
Table(2): solubility
IR SPECTROSCOPY:
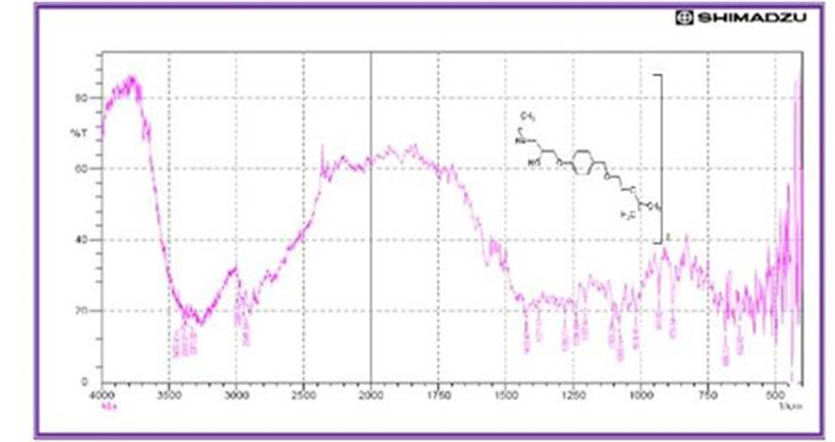
The IR spectra of dapagliflozin with its functional group identification, were shown in the following graph. IR spectra scanning of sample: dapagliflozin and bisoprolol[17][3].
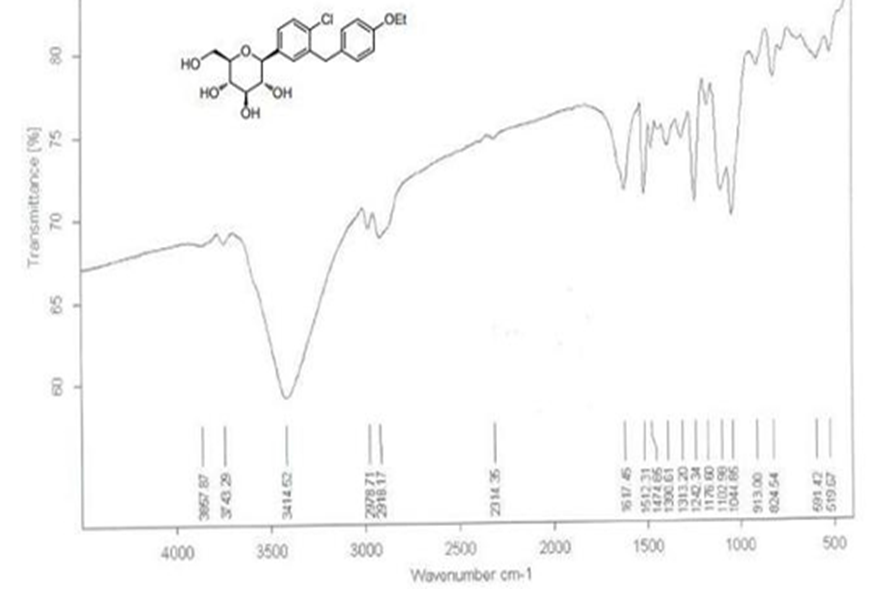
Fig(8):IR spectra of standard dapagliflozin[17]
Fig(9): IR spectra of standard bisoprolol[17]
THIN LAYER CHROMATOGRAPHY:
The combination of dapagliflozin propanediol monohydrate and bisoprolol fumarate is indicated for patients with type 2 diabetes mellitus with blood pressure or cardiovascular risks and has been approved by the Central Drugs Standard Control Organization (CDSCO)[17][18].
SELECTION OF STATIONARY PHASE:
A polar stationary phase consisting of precoated silica gel G60 F254 aluminum sheet (10 × 10 cm, 0.2 mm layer thickness) and a mobile phase consisting of a mixture of methanol?ethyl acetate?25% ammonia (0.5:6:0.3, V/V) were selected[18][22].
WAVELENGTH OF DAPAGLIFLOZIN AND BISOPROLOL:
Peaks of both drugs were obtained at RF values of 0.24 and 0.46 for dapagliflozin propanediol monohydrate and bisoprolol fumarate, respectively, at an analytical wavelength of 223 nm[8]. The method was observed to be linear in the range of 800?3200 ng/band for dapagliflozin propanediol monohydrate and 400?1600 ng/band for bisoprolol fumarate with a correlation coefficient (R2) of 0.9998 for dapagliflozin propanediol monohydrate and 0.9986 for bisoprolol fumarate[19][20].Fractional factorial design was employed to assess the robustness of the optimized method.
Forced degradation was performed to study the intrinsic stability of both drugs in acidic, basic, oxidation, thermal, and light conditions. Bisoprolol fumarate showed significant degradation in acidic and oxidative conditions, while dapagliflozin propanediol monohydrate showed stability in all conditions applied. The proposed method validated as per the International Council for Harmonisation (ICH) Q2 (R2) guideline and was found to be robust, accurate, precise, reproducible, and specific for the simultaneous quantification of both drugs in bulk and tablet[21][23].
CONCLUSION:
This method is well suited for simultaneous estimation in synthetic mixture.it can be easily conveniently adopted for routine analysis of semi solid dosage form[24].The methodology of dissolution and quantification were validated and developed from the requirements of ICH and USP.
This work presents a simple, selective, precise, and accurate stability-indicating instrumental thin-layer chromatography (TLC) method for the simultaneous quantification of dapagliflozin propanediol monohydrate and bisoprolol fumarate in bulk and tablet[23]. The proposed method was validated as per the International Council for Harmonisation (ICH) Q2 (R2) guideline and was found to be robust, accurate, precise, reproducible, and specific for the simultaneous quantification of both drugs in bulk and tablet[24][26]].
REFERENCES

K. S. S. Chakravarthi, K. B Ilango, S. Jeevitha, S. Kamalakannan, S. Kesavan, S. Sanjaya krishnan, M. Snega, Dapagliflozin and Bisoprolol: A Brief Review, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 2027-2037. https://doi.org/10.5281/zenodo.17153762
 10.5281/zenodo.17153762
10.5281/zenodo.17153762
