
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmaceutical Chemistry, Narasaraopeta Institute of Pharmaceutical Sciences, Narasaraopet, Andhra Pradesh, 522601, India.
Guillain-Barré Syndrome (GBS) is an uncommon but serious immune-mediated disorder in which the body’s defense system targets the peripheral nerves. It represents a leading global cause of acute flaccid paralysis. The condition usually begins with symmetrical weakness in the lower limbs that ascends and, in severe instances, can lead to respiratory failure. Despite its low incidence, GBS demands urgent medical intervention to prevent life-threatening complications. GBS can be triggered by SARS-CoV-2 (virus that causes COVID-19) in some individuals, a para-infectious or post-infectious condition where the nerves are more likely to be attacked by the immune system. This article provides an in-depth review of GBS including epidemiology, etiology, immunopathogenesis, clinical presentation, diagnostic strategies, management protocols, outcomes, and current research trends.
Guillain-Barré Syndrome (GBS) is an uncommon autoimmune neuropathy in which the immune system erroneously targets components of the peripheral nervous system, leading to muscle weakness and sometimes paralysis. This attack disrupts nerve signals, causing symptoms like numbness, tingling, muscle weakness, which can progress rapidly. Guillain Barré syndrome is also known as “Landry’s paralysis”. The syndrome was first recognized during world war I by Guillain, Barré and Strohl, who observed acute paralysis accompanied by elevated cerebrospinal fluid (CSF) protein without corresponding pleocytosis . The disease typically follows an infection, trauma, or vaccination and is characterized by symmetric weakness and hyporeflexia or areflexia. GBS is likely to be seen in SARS-CoV-2 post-infectious patients based on ongoing investigations. Due to its rapid progression, early recognition and prompt initiation of therapy are essential for a favorable outcome. [1][2][3]
Epidemiology
GBS can occur at any age, though it is somewhat more frequent men than in women. There are 1,00,000 new cases of GBS every year. Seasonal variations are described and spikes of GBS have been reported following infectious outbreaks, most notably in relation to Campylobacter jejuni and Zika virus and a recent studies state that GBS can occur in individuals with post corona virus infection. Surveillance data from different countries highlight variation in clinical subtypes and outcomes, possibly reflecting genetic, environmental, and healthcare access differences. Old people are more commonly affected (peak of GBS is between 50 and 70 years of age) and the male: female ratio is 1.5:1. [5][6]
Etiology And Risk Factors
GBS is most commonly preceded by an infection. In nearly two-thirds of patients, the onset of GBS follows a recent respiratory or gastrointestinal infection. Key etiological agents include:
Beyond infectious triggers, vaccinations have gained attention as potential precipitants of GBS, but with a notably lower attributable risk compared to infectious etiologies. Certain vaccines, including those against influenza and certain strains of influenza-like illness, have been associated with a slight but noteworthy increase in GBS risk, prompting ongoing surveillance and risk assessment efforts. [1][7]
Immunopathogenesis
The disease mechanism is primarily driven by an abnormal immune reaction involving molecular mimicry, where antibodies directed against infectious antigens cross-react with neural components, in which the immune system becomes activated in response to infectious antigen with structural similarity to the myelin or axonal components, resulting in tissue-specific peripheral nerve and nerve root injury in specific individuals. Antibodies generated against infectious agents cross-react with components of peripheral nerve tissue, especially gangliosides like GM1, GD1a, and GQ1b.
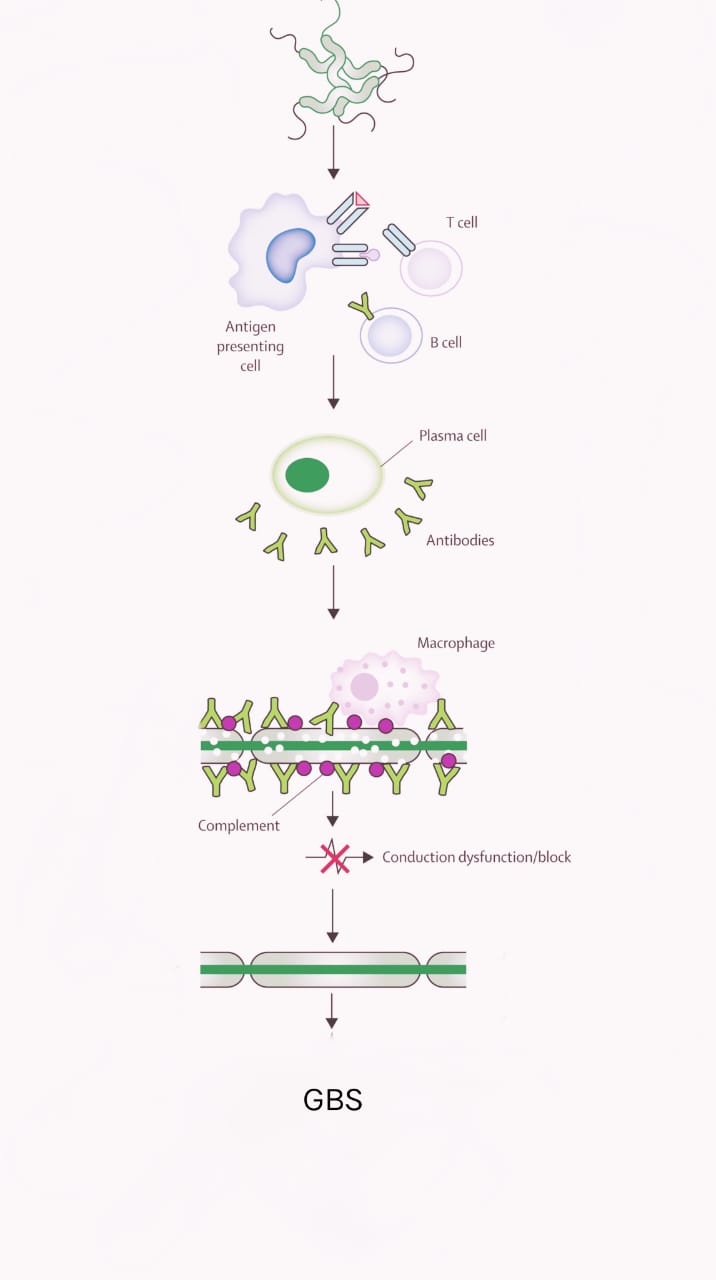
This leads to:
GBS Variants
Clinical Manifestations
Clinical features usually evolve within several days to weeks and may include:
Miller Fischer Syndrome (MFS), a recognized variant, is classically defined by the triad of impaired eye movements, loss of coordination, and absent reflexes. [8][9]
Diagnostic Evaluation
Early recognition is very important for timely management of GBS. Diagnostic criteria is as follows:
Differential diagnoses include transverse myelitis, botulism, myasthenia gravis, and spinal cord compression. [6][10]
Treatment
There is no proper cure is possible but therapy regarding immune system and some supportive care parameters can be taken for the improvement in recovery process.
Immunotherapies:
Supportive care parameters:
Rehabilitation:
Other therapies:
These therapies are equally effective but combining them doesn’t yield any additional benefit. Early initiation within 2 weeks of symptom onset provides the best outcomes. [1][11]
Prognostication And Future Outlook
The full recovery is possible in majority of the patients, but it may take several months. Most of the patients are able to walk independently by six months. Although most of them are recover fully, approximately 15% are not able to recover fully. There are chances of mortality that ranges from 3-7% due to failure of autonomic nervous system or sepsis.
Adverse prognostic factors are as follows:
Rehabilitation plays a key role in restoring the ability to function independently and includes physiotherapy, occupational therapy and psychosocial support. [7][12]
Current Research and Advances
One of the recent researches GBS made is to therapeutic advance:
Therapeutic advances:
Diagnostic and Prognostic improvements:
Root cause and Activators:
Role Of Pharmacists and Healthcare Professionals
Pharmacists and healthcare workers are integral to multidisciplinary management of GBS:
CONCLUSION
Guillain-Barré Syndrome is a rapidly evolving autoimmune disorder that needs early recognition and it causes a wide range of different outcomes for the prevention. Most of the patients are able to recover within a year, but on the other hand some of the patients are not able to recover for a longer time. A very small group of patients die due to the complications of this syndrome. Recently, the association between GBS and COVID-19 infection (caused by corona virus) as well as some vaccines has been identified. But the exact mechanism is not known and the research is still under process. This is GBS’s normal changing epidemiology. Currently, Intravenous immunoglobulin (IVIg) and Plasma exchange are preferred as cornerstone of treatment. Basically, GBS is still a diagnostic challenge for medical staff, and the future research that considers patient immunotherapy, biomarkers, and long-term rehabilitation for the better outcomes of the patient is required.
REFERENCES






M. Kasthuri*, J. N. Suresh Kumar, P. Priya Reethika, Sk. Nazma, M. Sai Maneeswar, P. Sai Krishna, N. Siva Gopi, Guillain Barré Syndrome: A Comprehensive Review of Immunopathogenesis, Diagnostic Evaluation and Treatment, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 231-236 https://doi.org/10.5281/zenodo.17038019
 10.5281/zenodo.17038019
10.5281/zenodo.17038019