Valmik Naik College of Pharmacy, Telwadi, Kannad, Chh. Sambhajinagar
Dysmenorrhea or painful menstruation, is among the most prevalent gynecological disorders affecting women of reproductive age and poses a significant global public health concern. It is classified into primary and secondary forms, with primary dysmenorrhea resulting from excessive uterine prostaglandin production in the absence of pelvic pathology, and secondary dysmenorrhea arising from identifiable conditions such as endometriosis, adenomyosis, or uterine fibroids. The condition manifests as cyclic lower abdominal pain often accompanied by systemic symptoms including nausea, headache, and fatigue, leading to substantial impairment in daily activities, academic performance, and emotional well-being. The pathophysiology involves elevated prostaglandin synthesis, vasopressin release, and inflammatory mediator activity, which induce uterine hyper contractility and ischemia. Risk factors include early menarche, prolonged or heavy menstrual flow, stress, sedentary lifestyle, and genetic predisposition. Management requires a comprehensive, multidisciplinary approach integrating pharmacological and non-pharmacological interventions. Nonsteroidal anti-inflammatory drugs (NSAIDs) remain the first-line treatment, while hormonal contraceptives, antispasmodics, and gonadotropin-releasing hormone agonists serve as effective alternatives in resistant cases. Adjunctive therapies such as heat application, exercise, yoga, and dietary modifications provide additional relief. Raising menstrual health awareness, promoting early diagnosis, and encouraging holistic care can significantly improve quality of life for women affected by dysmenorrhea.
Dysmenorrhea is one of the most prevalent gynecological disorders affecting women of reproductive age, characterized by recurrent, cramping pain localized to the lower abdomen during menstruation [1]. It is a leading cause of absenteeism from school or work among young women and can significantly affect physical, emotional, and social wellbeing [2]. Although commonly perceived as a normal aspect of menstruation, dysmenorrhea can lead to severe discomfort and functional disability, necessitating clinical attention. The pain generally begins shortly before or at the onset of menstruation and may radiate to the lower back, thighs, or groin. Frequently, women also report associated systemic symptoms such as nausea, vomiting, diarrhea, headache, and fatigue [2]. Despite its benign nature, the recurrent and chronic characteristics of dysmenorrhea can profoundly influence mood, productivity, and interpersonal relationships [3].
Dysmenorrhea is broadly categorized into primary and secondary forms. Primary dysmenorrhea occurs in the absence of any identifiable pelvic pathology and is particularly common in adolescents and young women, usually developing within one to two years after menarche when ovulatory menstrual cycles become established [4]. Pain intensity often peaks during late adolescence and early adulthood and typically decreases with age or after childbirth [5]. Pathophysiologically, primary dysmenorrhea is linked to excessive production of uterine prostaglandins, especially prostaglandin F2α (PGF2α) and prostaglandin E2 (PGE2), synthesized from arachidonic acid under progesterone influence during the luteal phase [6]. The withdrawal of progesterone at menstruation triggers endometrial breakdown and prostaglandin release, which stimulate strong uterine contractions, vasoconstriction, and reduced uterine blood flow, culminating in ischemic pain [6]. Additional mediators— including vasopressin, leukotrienes, and endothelin’s—further enhance myometrial contractility and pain perception [7]. Hormonal imbalances, psychological stress, and genetic predisposition also modulate the severity and frequency of primary dysmenorrhea[8].
Secondary dysmenorrhea, on the other hand, arises due to identifiable pelvic pathologies such as endometriosis, adenomyosis, uterine fibroids, pelvic inflammatory disease, intrauterine adhesions, or the presence of intrauterine devices [9]. It generally appears later in life, often after the age of 25, and is frequently associated with additional gynecological symptoms including menorrhagia, metrorrhagia, dyspareunia, or infertility [9]. Pain may precede menstruation, persist throughout, and occasionally continue afterward [9]. Unlike primary dysmenorrhea, it does not typically diminish after childbirth and usually requires targeted management of the underlying condition [9]. Diagnostic approaches include pelvic examination, ultrasonography, magnetic resonance imaging (MRI), and, in selected cases, laparoscopy to identify structural or inflammatory abnormalities [10].
The global prevalence of dysmenorrhea varies widely, with estimates ranging from 45% to 95% depending on diagnostic criteria, age group, and cultural perceptions of menstrual pain [11]. Severe dysmenorrhea affects approximately 10–20% of menstruating women, resulting in substantial functional limitations and reduced quality of life [12]. Among adolescents, it is a leading cause of recurrent short-term school absenteeism, decreased concentration, and poor academic performance [7]. In adults, it contributes to work absenteeism, decreased productivity, and increased healthcare costs [12]. Chronic menstrual pain is also associated with psychological disturbances such as anxiety, depression, and somatization [7]. Despite its prevalence and impact, dysmenorrhea is often underdiagnosed and undertreated due to cultural taboos, normalization of menstrual pain, and limited awareness of effective management strategies [13].
Although dysmenorrhea is not life-threatening, its public health significance is substantial. The recurrent pain, interference with daily functioning, and associated psychological stress create a cumulative impact on women’s health and socioeconomic participation [12]. In low- and middle-income countries, limited access to menstrual health education and healthcare services exacerbates the problem [13]. Given its potential to affect reproductive and mental health outcomes, there is a pressing need for increased awareness, early diagnosis, and evidence-based management strategies [11].
Effective management of dysmenorrhea requires a multidimensional approach integrating pharmacological, non-pharmacological, and psychological interventions [16]. NSAIDs remain the first-line therapy due to their inhibition of prostaglandin synthesis [16], whereas hormonal contraceptives—including combined oral contraceptives, progestin-only formulations, and intrauterine systems—reduce ovulation and menstrual flow [16]. Nonpharmacological interventions such as heat therapy, exercise, relaxation techniques, transcutaneous electrical nerve stimulation (TENS), and dietary modifications have shown varying degrees of efficacy [17]. Complementary and alternative therapies, including acupuncture, herbal remedies, and yoga, are gaining attention for their potential benefits without significant side effects, although robust clinical evidence is still required [18].
Given its high prevalence, chronicity, and multidimensional impact, dysmenorrhea represents a major yet often overlooked public health concern. Comprehensive understanding of its etiology, pathophysiology, risk factors, and management is essential for effective prevention and treatment. This review provides an updated overview of current knowledge on dysmenorrhea, emphasizing recent advances in understanding mechanisms, diagnostic approaches, and therapeutic options, with a focus on promoting holistic care for affected women.
PATHOPHYSIOLOGY
Figure. 1
The pathophysiology of primary dysmenorrhea is mainly associated with excessive and dysregulated production of uterine prostaglandins, particularly prostaglandin F2α (PGF2α) and prostaglandin E2 (PGE2), synthesized from arachidonic acid under progesterone regulation [1]. Normally, progesterone maintains endometrial stability during the luteal phase, suppressing inflammatory mediators. During menstruation, the abrupt decline in progesterone triggers phospholipase A2 activation, releasing arachidonic acid, which is converted into prostaglandins via the cyclooxygenase (COX) pathway [2]. Elevated PGF2α and PGE2 increase uterine tone, high-amplitude rhythmic contractions, and reduce uterine blood flow, causing ischemic pain characteristic of primary dysmenorrhea [2]. Studies report that these contractions can generate intrauterine pressures exceeding 150–200 mmHg, contributing to severe pain [3].
Other mediators, including vasopressin, leukotrienes, interleukin-6 (IL-6), and tumor necrosis factor-alpha (TNF-α), augment uterine contractility and sensitization of nociceptive pathways [4,5]. Elevated vasopressin levels in women with severe pain suggest a synergistic effect with prostaglandins, inducing uterine hyperactivity and vasoconstriction, which further reduce uterine perfusion and amplify pain perception [4]. Inflammatory mediators promote crosstalk between immune and neuronal cells, heightening the intensity and duration of menstrual pain [5].
Secondary dysmenorrhea arises from identifiable pelvic pathologies that alter uterine structure or local biochemical environment. Endometriosis involves ectopic endometrial implants, overproducing prostaglandins and pro-inflammatory cytokines, leading to chronic inflammation and nociceptor sensitization [6]. Adenomyosis entails endometrial gland infiltration into the myometrium, causing uterine enlargement, elevated basal tone, and exaggerated contractions [7]. Structural anomalies like fibroids, cervical stenosis, or congenital malformations may obstruct menstrual flow or distort the uterine cavity, amplifying pain [8].
Neurological, hormonal, and psychological factors also modulate pain perception. Women with severe dysmenorrhea may develop central sensitization, increasing excitability of spinal neurons and altering supraspinal pain modulation, lowering pain thresholds [9]. Psychological stress, anxiety, and mood disturbances activate the hypothalamic–pituitary– adrenal (HPA) axis, increase cortisol levels, and disrupt endogenous pain inhibitory pathways, exacerbating uterine hyperactivity and pain perception [10]. Genetic predisposition and lifestyle factors, such as diet, physical activity, and sleep, further influence prostaglandin synthesis and pain sensitivity [8,14,15]. Collectively, dysmenorrhea is a multifactorial condition involving biochemical, structural, neuroendocrine, genetic, and psychosocial determinants [5,8,15].
CLINICAL FEATURES AND DIAGNOSIS
Clinical Features
Dysmenorrhea is primarily characterized by cyclical lower abdominal pain coinciding with menstruation, typically lasting 24–72 hours [1]. Pain is often cramping or colicky, radiating to the lower back, inner thighs, or groin [2]. Severity ranges from mild discomfort to severe incapacitating pain affecting routine activities and social life [2]. Systemic symptoms such as nausea, vomiting, diarrhea, headache, dizziness, sweating, and fatigue are common, primarily due to prostaglandin-induced uterine hypercontractility and effects on smooth muscle elsewhere [3]. Emotional irritability, anxiety, mood swings, and sleep disturbances may exacerbate pain perception [4].
Primary dysmenorrhea presents without structural abnormalities. Symptoms develop within 6–12 months post-menarche once ovulatory cycles are established. Pain peaks in late adolescence and early adulthood, often declining with age or after pregnancy [6].
Secondary dysmenorrhea typically begins after age 25 and is associated with pelvic pathology. Pain may precede menstruation, persist throughout, or continue post-menses. Additional complaints often include menorrhagia, irregular cycles, dyspareunia, infertility, or pelvic tenderness [9,10]
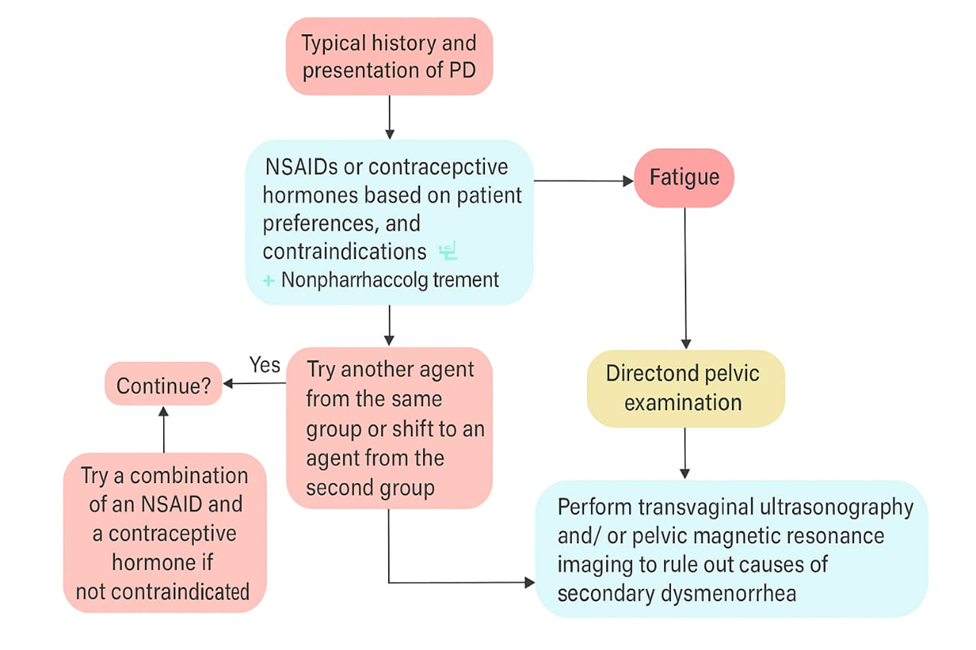
Diagnosis

figure. 2
Diagnosis involves differentiating primary from secondary causes, assessing severity, and evaluating impact on quality of life [11].
Effect on daily activities and prior response to therapy [12]
Physical examination includes abdominal palpation and pelvic exam (in sexually active women) to assess uterine size, mobility, and adnexal tenderness. Findings like uterine enlargement or nodularity may suggest adenomyosis or endometriosis [13].
Early and accurate differentiation between primary and secondary dysmenorrhea ensures timely management and prevents chronic pelvic pain or fertility issues [18].
Epidemiology and Risk Factors of Dysmenorrhea:
Dysmenorrhea is one of the most prevalent menstrual and gynecological disorders affecting women of reproductive age across the world. It is characterized by recurrent, cramping pain in the lower abdomen, often accompanied by nausea, headache, backache, and general malaise during menstruation. This condition significantly affects women’s quality of life, emotional well-being, and productivity, often leading to school or work absenteeism and reduced participation in daily activities. The global prevalence of dysmenorrhea varies considerably, ranging from 45% to 95%, depending on the definition used, population studied, and diagnostic criteria applied [1]. Despite being a common gynecological complaint, dysmenorrhea is often underdiagnosed and undertreated, as many women perceive menstrual pain as a normal part of the menstrual cycle rather than a medical concern that warrants evaluation and management.

Epidemiological studies across different continents demonstrate striking regional variations. In many Asian and African countries, prevalence rates have been reported as high as 84–94%, whereas in European and North American populations, estimates typically range from 50–75% [4,5]. In India, surveys indicate that approximately 70–80% of adolescent girls suffer from dysmenorrhea, with a significant proportion reporting that it adversely affects their academic performance, social interactions, and emotional health [6]. However, the true prevalence may be even higher, as many young women fail to seek medical advice due to cultural stigma, normalization of menstrual pain, and lack of awareness regarding treatment options [7]. In many societies, menstruation remains a taboo topic, leading to silence, embarrassment, and inadequate communication about menstrual health among adolescents.
The age of onset of dysmenorrhea typically coincides with menarche, and symptoms often become more pronounced in late adolescence or early adulthood. The condition tends to peak during the late teenage years and early twenties and may gradually subside with age or after childbirth [8]. This is thought to be related to hormonal and uterine changes following pregnancy, which may reduce uterine contractility and prostaglandin production. Primary dysmenorrhea is most common in women below 25 years of age and is not associated with any identifiable pelvic pathology, while secondary dysmenorrhea tends to occur in older women, particularly after the age of 30, and is often related to underlying conditions such as endometriosis, adenomyosis, uterine fibroids, or pelvic inflammatory disease [9]. Understanding these distinctions is crucial for accurate diagnosis and effective management.
RISK FACTORS
A wide range of biological, lifestyle, and psychosocial factors have been identified as influencing the onset, intensity, and duration of dysmenorrhea. Among the most well-established biological risk factors is early menarche, typically before the age of 12, which increases the cumulative exposure to prostaglandins and other mediators that stimulate uterine contractions [10]. Similarly, longer menstrual periods (greater than 7 days) and heavier menstrual flow are associated with a greater likelihood of dysmenorrhea, as excessive endometrial shedding leads to elevated prostaglandin synthesis and uterine ischemia [11]. In addition, women with shorter menstrual cycles (less than 27 days) are more prone to dysmenorrhea due to more frequent hormonal fluctuations and endometrial turnover.
Nulliparity, or the absence of previous childbirth, is another strong risk factor, as the uterus in nulliparous women tends to exhibit higher basal tone and stronger contractions during menstruation compared to parous women [12]. After childbirth, changes in uterine size, cervical dilation, and hormonal regulation are thought to alleviate pain symptoms in many women.
Lifestyle factors play an equally important role in modulating menstrual pain. Smoking has been consistently associated with increased severity of dysmenorrhea, possibly due to nicotine-induced vasoconstriction, which reduces uterine blood flow and exacerbates ischemic pain. Similarly, high caffeine consumption and alcohol use have been linked to elevated prostaglandin levels and hormonal imbalances [13]. Conversely, women who engage in regular physical activity tend to experience milder symptoms, likely due to improved blood circulation, reduced stress, and the release of endorphins, which act as natural pain suppressors. In contrast, sedentary behavior and obesity have been associated with higher incidence and intensity of menstrual pain [14].
Psychological and emotional well-being also have a significant impact on menstrual health. High levels of stress, anxiety, and depression can heighten the perception of pain through alterations in neuroendocrine and pain modulation pathways [15]. Women who experience chronic stress may have increased activation of the hypothalamic-pituitary adrenal (HPA) axis, leading to hormonal imbalances that intensify uterine contractions and pain sensitivity. Moreover, emotional distress often reduces adherence to healthy lifestyle behaviors and exacerbates fatigue, sleep disturbances, and irritability during menstruation.
Socioeconomic and cultural factors further influence both the prevalence and reporting of dysmenorrhea. Women from low socioeconomic backgrounds often face barriers such limited access to healthcare facilities, inadequate menstrual hygiene resources, and poor nutritional status, all of which can worsen symptoms [16]. Educational level also plays a pivotal role—women with greater awareness of menstrual physiology are more likely to seek medical advice, adopt healthy coping strategies, and use appropriate medications such as NSAIDs or hormonal contraceptives. Conversely, those with lower education levels may rely on traditional remedies, tolerate severe pain, or remain unaware of effective treatment options. Cultural taboos and societal restrictions surrounding menstruation also discourage open discussion, resulting in underreporting and delayed diagnosis.
Furthermore, genetic and familial predisposition has been suggested as a contributing factor. Studies have found that women with a family history of dysmenorrhea are more likely to experience similar symptoms, suggesting a hereditary component in pain sensitivity and prostaglandin regulation [17]. Nutritional factors, such as low intake of omega-3 fatty acids, vitamin D deficiency, and inadequate magnesium levels, have also been associated with an increased risk and severity of menstrual pain [18].
Collectively, these findings highlight that dysmenorrhea is a multifactorial condition, influenced by a complex interplay of biological, behavioral, psychological, and social determinants. Addressing these risk factors through education, lifestyle modification, and early intervention can play a pivotal role in reducing its burden. Recognizing the widespread prevalence and determinants of dysmenorrhea is essential not only for clinical management but also for the promotion of menstrual health awareness, especially among adolescent girls. Comprehensive school-based health education programs, community awareness campaigns, and improved access to reproductive healthcare services can contribute significantly to destigmatizing menstruation and empowering women to manage dysmenorrhea effectively.
PHARMACOLOGICAL TREATMENT OF DYSMENORRHEA
Dysmenorrhea, defined as painful menstruation, is one of the most common gynecological complaints among women of reproductive age. The intensity of pain can vary from mild discomfort to severe cramping that interferes with daily activities, work, and social functioning. Pharmacological therapy remains the primary method of management, particularly in primary dysmenorrhea, where no underlying pelvic pathology is identified. The goals of treatment include relieving pain, reducing uterine hypercontractility, improving quality of life, and, in cases of secondary dysmenorrhea, addressing the underlying disorder, such as endometriosis, adenomyosis, or pelvic inflammatory disease.
The main classes of pharmacological agents used for dysmenorrhea include nonsteroidal anti-inflammatory drugs (NSAIDs), hormonal contraceptives, antispasmodics, analgesics, gonadotropin-releasing hormone (GnRH) agonists, and androgenic agents. Additional emerging therapies, such as selective COX-2 inhibitors and nutraceuticals, are also being investigated for their potential roles in dysmenorrhea management.
NSAIDs are considered first-line therapy for primary dysmenorrhea due to their potent anti-inflammatory and analgesic properties. They primarily act by reducing the production of prostaglandins, which are key mediators of uterine contractions, ischemia, and pain during menstruation.
Mechanism of Action:
NSAIDs inhibit the enzyme cyclooxygenase (COX-1 and COX-2), thereby blocking the conversion of arachidonic acid into prostaglandins, specifically prostaglandin F2α (PGF?α) and prostaglandin E2 (PGE?). Reduced prostaglandin levels lead to decreased uterine muscle contractions, improved uterine blood flow, and diminished pain sensitivity.
Commonly Used NSAIDs:
Clinical Considerations:
NSAIDs are most effective when started 1–2 days before the expected onset of menses or at the onset of symptoms. They provide rapid relief and can significantly reduce pain intensity within the first 24 hours.
Advantages:
Side Effects:
Summary:
NSAIDs remain the cornerstone of primary dysmenorrhea therapy due to their targeted mechanism, rapid efficacy, and overall favorable safety profile when used short-term.
Hormonal contraceptives, including combined oral contraceptives (COCs), progestin-only pills, injectable progestin’s, and levonorgestrel-releasing intrauterine devices (LNG-IUS), are effective in women who either do not respond to NSAIDs or also desire contraception. These agents are particularly useful for moderate to severe dysmenorrhea and secondary dysmenorrhea associated with endometriosis or heavy menstrual bleeding.
Mechanism of Action:
Forms and Examples:
Benefits:
Adverse Effects:
Clinical Considerations:
Hormonal therapy is particularly effective in women with dysmenorrhea related to endometriosis, as it suppresses ectopic endometrial tissue and reduces inflammatory mediators. Continuous or extended-cycle regimens may provide superior pain relief compared to cyclic regimens.
Antispasmodics are used to relieve uterine smooth muscle spasms, thereby reducing pain and improving uterine blood flow. These drugs are generally reserved for patients who cannot tolerate NSAIDs or for those with concomitant gastrointestinal symptoms.
Common Agents:
Mechanism of Action:
Antispasmodics work either by inhibiting parasympathetic activity (anticholinergic effect) or by directly relaxing uterine smooth muscle. This reduces involuntary contractions that contribute to dysmenorrhea pain.
ADVERSE EFFECTS:
Clinical Considerations:
Antispasmodics can be used alone in mild cases or in combination with NSAIDs for more severe symptoms. However, their analgesic effect is usually less pronounced compared to NSAIDs or hormonal therapy.
Paracetamol may be used in women with mild dysmenorrhea or when NSAIDs are contraindicated (e.g., peptic ulcer disease, renal impairment, or NSAID allergy).
Mechanism of Action:
Paracetamol inhibits central prostaglandin synthesis in the hypothalamus and spinal cord, leading to decreased pain perception.
Advantages:
Limitations:
5. Gonadotropin-Releasing Hormone (GnRH) Agonists
Gnarl agonists, such as leuprolide acetate and goserelin, are used primarily in secondary dysmenorrhea, particularly when associated with endometriosis. These drugs create a hypoestrogenic state, leading to regression of ectopic endometrial tissue.
Mechanism of Action:
Side Effects:
Clinical Considerations:
GnRH agonists are often used in combination with “add-back” therapy (low-dose estrogen or progestin) to minimize hypoestrogenic side effects. They are highly effective for pain relief in endometriosis-related dysmenorrhea but are not suitable for long-term use due to risk of osteoporosis.
6. Androgenic Agents (Danazol)
Danazol is an androgenic steroid that suppresses the mid-cycle surge of LH and FSH, leading to endometrial atrophy. It is mainly reserved for women with severe endometriosis related dysmenorrhea who have not responded to other therapies.
Mechanism of Action:
Adverse Effects:
Clinical Considerations:
Danazol use has declined due to its androgenic side effects and the availability of better tolerated alternatives such as GnRH agonists and hormonal contraceptive
7. Emerging and Adjunctive Therapies
Recent studies are exploring additional pharmacological approaches, including:
Selective COX-2 inhibitors: Similar mechanism to NSAIDs but with reduced gastrointestinal side effects
Nutraceuticals and supplements: Omega-3 fatty acids, magnesium, vitamin B1, and herbal remedies (e.g., ginger, chamomile) may offer modest pain relief
Combination therapy: In cases of severe or refractory dysmenorrhea, a combination of NSAIDs and hormonal therapy may be more effective than monotherapy
SUMMARY
Pharmacological management of dysmenorrhea requires an individualized approach based on the type, severity of symptoms, underlying causes, and patient preferences. NSAIDs remain first-line therapy for primary dysmenorrhea due to their efficacy and rapid onset, whereas hormonal contraceptives are preferred for long-term relief and in patients with secondary dysmenorrhea related to endometriosis. Antispasmodics and analgesics serve as adjuncts or alternatives in mild cases, while GnRH agonists and androgenic agents are reserved for severe, treatment-resistant secondary dysmenorrhea. Emerging therapies continue to expand the options for effective, well-tolerated management, with the ultimate goal of improving quality of life and reducing the burden of menstrual pain in women worldwide.
CONCLUSION
Dysmenorrhea remains one of the most common and distressing gynecological disorders affecting women of reproductive age. Despite being a natural component of the menstrual cycle, the severity and recurrence of menstrual pain in dysmenorrhea can significantly impair daily activities, productivity, and overall quality of life. It is broadly categorized into primary and secondary dysmenorrhea, each with distinct underlying mechanisms and clinical implications. Primary dysmenorrhea occurs without identifiable pelvic pathology and is typically linked to increased uterine prostaglandin production, leading to uterine hypercontractility, ischemia, and pain. In contrast, secondary dysmenorrhea arises due to specific pelvic pathologies such as endometriosis, adenomyosis, pelvic inflammatory disease, or uterine fibroids. Understanding this classification is crucial for accurate diagnosis and targeted management.
The global burden of dysmenorrhea is substantial, with prevalence rates ranging from 45% to over 90% among menstruating women, particularly adolescents and young adults. However, due to sociocultural attitudes, embarrassment, and the normalization of menstrual pain, many women do not seek medical attention, resulting in under diagnosis and under treatment. This highlights the need for increased awareness, education, and DE stigmatization of menstrual health. The condition not only affects physical well-being but also has psychosocial and economic implications, including absenteeism from school or work, reduced academic performance, and emotional distress.
From a pathophysiological perspective, research has established that excessive synthesis of prostaglandins, mainly prostaglandin F2α and prostaglandin E2, plays a central role in the pain mechanism. These compounds induce intense uterine contractions, reduced blood flow, and heightened sensitivity of nerve endings. Hormonal fluctuations, particularly the withdrawal of progesterone before menstruation, trigger the release of these prostaglandins from endometrial cells. Moreover, other mediators such as vasopressin, leukotrienes, and endothelins may contribute to uterine hyperactivity and pain perception. In secondary dysmenorrhea, the pathogenesis depends on the underlying disease, with inflammatory or structural changes amplifying menstrual pain.
Effective management of dysmenorrhea involves a multidimensional approach that combines pharmacological, non-pharmacological, and lifestyle interventions. Pharmacologically, nonsteroidal anti-inflammatory drugs (NSAIDs) remain the first-line therapy, acting by inhibiting cyclooxygenase enzymes and reducing prostaglandin production. Hormonal contraceptives, including oral pills, intrauterine systems, and injectables, offer additional benefits by suppressing ovulation and stabilizing endometrial growth. In refractory cases or secondary causes, surgical interventions may be required. Complementary methods such as heat therapy, regular physical exercise, dietary modifications, stress reduction, and the use of alternative therapies like acupuncture or herbal medicine have also shown supportive benefits. A personalized treatment plan, tailored to symptom severity, individual preference, and the presence of comorbidities, is essential for optimal results.
Importantly, early recognition and education play a pivotal role in preventing chronic pain development and improving menstrual health literacy. Health professionals should prioritize menstrual education in schools and community settings to empower young women with knowledge about normal and abnormal menstrual symptoms. Encouraging open discussions about menstruation can also reduce stigma and promote timely medical consultation. Furthermore, ongoing research into novel therapies, including selective prostaglandin receptor modulators and non-invasive diagnostic tools, holds promise for improving outcomes in the near future.
In summary, dysmenorrhea, though often perceived as a minor or inevitable aspect of menstruation, represents a significant public health concern with wide-ranging physical, emotional, and social consequences. Its effective management requires not only medical treatment but also societal change in how menstrual pain is perceived and addressed. Through comprehensive education, timely diagnosis, and evidence-based therapeutic strategies, the burden of dysmenorrhea can be greatly reduced, enhancing the well-being and quality of life of millions of women worldwide. Continued research, awareness campaigns, and holistic approaches are essential to ensure that menstrual health receives the attention it rightfully deserves in both clinical and community settings.
REFERENCES

Vaishnavi Rokade, Sabafarin Shaikh, Prachi Kadam, Pragati Nade, Shital Rathod, Snehal Rathod, Sandesh Aade, Dysmenorrhea, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 2318-2334. https://doi.org/10.5281/zenodo.17617476
 10.5281/zenodo.17617476
10.5281/zenodo.17617476
