
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Sharda School of Pharmacy, Pethapur, Gandhinagar, Gujarat – 382610
Buoyancy-Driven Drug Delivery Systems (BDDDS), commonly known as floating systems, represent a crucial strategy for optimizing the therapeutic performance of orally administered drugs that exhibit a narrow absorption window. This comprehensive review focuses specifically on the systematic methodology required to design and optimize these complex floating formulations to ensure reliable gastric retention. The review establishes the clinical necessity for prolonged gastric residence time (GRT) in managing chronic conditions, exemplified by the absorption challenges of Dihydropyridine Calcium Channel Blockers. The core of the article details the application of a quality-focused development paradigm for system optimization. This involves the rigorous identification, control, and functional correlation of Critical Material Attributes (CMAs) (e.g., polymer viscosity, concentration) and Critical Process Parameters (CPPs) (e.g., compression force) with the desired Critical Quality Attributes (CQAs). Key CQAs discussed include rapid Floating Lag Time (FLT), extended Total Floating Duration (TFT), optimal swelling kinetics, and stable sustained drug release[5]. By detailing this scientific approach, this review demonstrates how to reliably manufacture BDDDS to deliver predictable and superior performance.
1.1. Gastroretentive Drug Delivery Systems (GRDDS)
Gastroretentive Drug Delivery Systems (GRDDS) are engineered to counter the limitations of rapid GI transit by physically prolonging the Gastric Residence Time (GRT) [1]. By retaining the dosage form in the stomach, GRDDS maximize drug release at the optimal site of absorption [2]. This strategy is vital for drugs that exhibit site-specific absorption in the upper GI tract, have limited stability at the higher pH of the lower intestinal milieu, or possess short biological half-lives, requiring sustained release at the site of absorption [3].
Objectives [4],
1.2. Floating System
This review focuses specifically on the Buoyancy-Driven Drug Delivery System (BDDDS), or floating systems, which are a highly favored GRDDS approach due to their reliability in achieving GRT extension. Flotation is achieved by ensuring the dosage form maintains a net density less than that of gastric fluid (< 1.0 g/mL) by controlled gas generation or effective air entrapment within a hydration barrier [5].
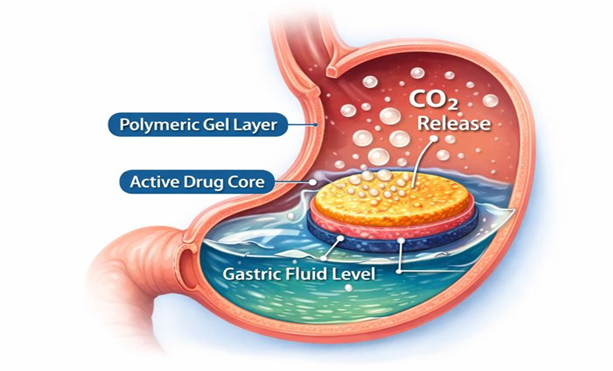
FIGURE: 1 Floating System
The two primary approaches are Effervescent Systems (using gas-generating components like sodium bicarbonate) and Non-Effervescent Systems (using highly porous matrices or swelling hydrocolloids to trap air [6].
Classification of floating system:
Table: 1 Good Candidates for Gastroretentive Drug Delivery System [7]
|
Sr. No. |
Drug |
Drug Category |
Bioavailability (%) |
Reason for Suitability in GRDDS |
|
1 |
Verapamil |
Calcium channel blocker |
20–35 |
Narrow absorption window in upper GIT and extensive first-pass metabolism |
|
2 |
Nifedipine |
Calcium channel blocker |
45–65 |
Short half-life and better absorption in stomach/upper intestine |
|
3 |
Omeprazole |
Proton pump inhibitor |
35–60 |
Acid-labile drug, acts locally in stomach, benefits from prolonged gastric retention |
|
4 |
Atenolol |
Antihypertensive |
40–50 |
Absorbed mainly in upper GIT; limited colonic absorption |
|
5 |
Propranolol |
Antihypertensive |
4–26 |
High first-pass metabolism and narrow absorption window |
|
6 |
Verapamil |
Antihypertensive |
18–35 |
Requires controlled release and prolonged gastric residence for improved absorption |
|
7 |
Diltiazem |
Calcium channel blocker |
40 |
Short biological half-life and absorption mainly in upper GIT |
|
8 |
Lidocaine |
Local anaesthetic |
35 |
Poor oral bioavailability due to first-pass metabolism; benefits from controlled release |
|
9 |
Clarithromycin |
Antibiotic |
50 |
Used for H. pylori infection; requires prolonged gastric contact |
|
10 |
Ramipril |
ACE inhibitor |
28 |
Absorbed in upper GIT and undergoes first-pass metabolism |
Table 2 Gastroretentive Products Available in Market[8]
|
Brand Name |
Drug |
Type of Gastroretentive System |
Company / Region |
|
Valrelease® |
Diazepam (15 mg) |
Floating capsule |
Hoffmann-La Roche, USA |
|
Madopar® HBS (Prolopa® HBS) |
Benserazide + L-dopa |
Floating, CR capsule |
Roche Products, USA |
|
Liquid Gaviscon® |
Al(OH)? + Mg carbonate |
Effervescent floating liquid (antacid) |
GlaxoSmithKline |
|
Topalkan® |
Al–Mg antacid |
Floating liquid alginate |
Pierre Fabre, France |
|
Conviron® |
Ferrous sulphate |
Colloidal gel forming floating system |
Ranbaxy, India |
|
Cytotech® |
Misoprostol (100 µg/200 µg) |
Bilayer floating capsule |
Pharmacia, USA |
|
Cifran OD® |
Ciprofloxacin (0.5–1 g) |
Gas-generating floating system |
Sun Pharma, India |
|
Rantac OD® |
Ranitidine (300 mg) |
Floating system |
J.B. Chemicals, India |
|
Dompan SR® |
Pantoprazole + Domperidone |
Floating tablet |
Medley, India |
|
Creon 10000® |
Pancreatin |
Microcapsules |
Abbott, India |
MATERIALS AND METHODS [9-12].
3.1. Formulation Materials Selection
The optimization process begins with the critical selection of excipients that directly impact both buoyancy and release kinetics.
Table 3: Formulation Materials
|
Component |
Examples |
Classification |
Critical Material Attribute (CMA) |
Role / Impact on FDDS Performance |
|
Active Ingredient (API) |
Drug with narrow absorption window |
Drug Substance |
Solubility, dose, absorption window |
Suitable for sustained release and gastric retention; benefits from prolonged gastric residence time |
|
Polymeric Matrix Agents |
HPMC, PEO |
CMAs |
Molecular weight, viscosity grade, concentration |
Forms a strong gel layer controlling drug release; enables air entrapment necessary for tablet flotation |
|
Gas-Generating Agents (Effervescent systems) |
Sodium bicarbonate |
CMAs |
Type, particle size, concentration |
Generates CO? on contact with gastric fluid; directly influences Floating Lag Time (FLT) |
|
Lubricants & Glidants |
Magnesium stearate, talc |
CMAs |
Concentration |
Excess levels can hinder tablet hydration, delay gel formation, and increase FLT; therefore must be minimized |
3.2. Manufacturing Process (Generalized Tablet Formulation) [14].
The tablet manufacturing method, typically direct compression or wet granulation, must be precisely controlled to ensure system functionality.
3.3. Pre- and Post-Compression Characterization [15].
Systematic evaluation is performed to link input variables to initial quality outputs:
Evaluation of Powder Blend[16]
a) Angle of Repose
Angle of repose is defined as the maximum angle possible between the surface of a powder heap and the horizontal plane. It is an indirect measure of powder flow property.
Formula:
tan?θ=hr

Where:
|
Angle of Repose (°) |
Flow Property |
|
< 30 |
Excellent |
|
30–40 |
Good |
|
> 40 |
Poor |
b) Bulk Density
Bulk density represents the total density of powder, including interparticle void spaces.
Formula:
Bulk Density=Weight of powderBulk volume

c) Percentage Porosity
Porosity indicates the void space within a powder bed and influences hardness, disintegration, and drug release.
Formula:
%Porosity=Void volumeBulk volume×100

or
%Porosity=Bulk volume – True volumeBulk volume×100

2. Evaluation of Floating Tablets [17]
a) Measurement of Buoyancy Capability
Floating behavior is evaluated by measuring resultant weight in:
Observation:
b) In-Vitro Floating and Dissolution Behaviour
Key Findings:
c) Weight Variation Test
Performed to ensure dose uniformity.
USP Method:
Acceptance Criteria:
d) Hardness and Friability
Hardness
Defined as force required to break a tablet under diametric compression.
Instruments used:
Friability
Measured using Roche Friabilator.
Formula:
%Friability=Initial weight – Final weightInitial weight×100

e) Particle Size Analysis & Surface Characterization
(For Floating Microspheres and Beads)
|
Parameter |
Method |
|
Particle size |
Optical microscopy |
|
Size distribution |
Dry state measurement |
|
Surface morphology |
Scanning Electron Microscopy (SEM) |
f) X-Ray / Gamma Scintigraphy
Used to track the position of dosage form in GIT.
g) Pharmacokinetic Studies
Essential in-vivo evaluation parameter.
Key Parameters:


Observation:
RESULT & DISCUSSION [18-20].
4.1. The Systematic Development Paradigm for Optimization
The core of BDDDS development is the implementation of a systematic, science-driven approach to define the Design Space. This approach uses structured experimental designs to efficiently map the complex relationships between the input CMAs/CPPs and the final CQAs, allowing the formulator to select optimal manufacturing parameters.
The linkage between input and output is crucial for optimization:
4.2. In Vitro Performance Evaluation
The optimized formulation must demonstrate functionality and consistency through rigorous in vitro testing:
4.2.1. Buoyancy Test
This test directly confirms the success of the optimization regarding gastric retention. The FLT must be rapid (ideally < 1-5 minutes) to prevent premature emptying, and the Total Floating Duration (TFT) must meet the sustained retention target (typically > 8-12 hours).
4.2.2. Swelling Index and Water Uptake
The Swelling Index must be optimized to ensure it provides sufficient volume increase for air entrapment while forming a controlled-release gel barrier. The rate and extent of swelling are measured over time to ensure consistency across batches[21].
4.2.3. Drug Release Studies
Dissolution testing confirms that the release profile adheres to the target requirements. The data are rigorously analyzed using kinetic models (Korsmeyer-Peppas and Higuchi) to ensure the mechanism of release is understood, predictable, and optimized for sustained action [22].
CONCLUSION
The development of Buoyancy-Driven Drug Delivery Systems for drugs with narrow absorption windows is fundamentally an optimization challenge. The adoption of a systematic, quality-focused approach is mandatory to navigate the complex interdependencies between formulation inputs and performance outputs. By defining a robust Design Space and precisely controlling CMAs and CPPs, formulators can consistently produce dosage forms that achieve reliable flotation, optimal swelling, and highly predictable sustained release. This strategic approach ensures the maximum therapeutic benefit for the patient in the long-term management of chronic diseases.
ACKNOWLEDGEMENT
The authors wish to express their profound gratitude to the Head of the Department of Pharmaceutics, Sharda School of Pharmacy, for providing the necessary laboratory facilities and administrative support to conduct the research that forms the foundation of this review. We also thank the Gujarat Technological University (GTU) for the continued opportunity and resources provided to pursue this area of specialization.
REFERENCES


Patel Nrup, Amar Raval, Gastro Retentive Drug Delivery System: A Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 734-742. https://doi.org/10.5281/zenodo.18186802
 10.5281/zenodo.18186802
10.5281/zenodo.18186802