M.J.P. Rohilkhand University, Bareilly UP, India.
Gastroprotective drug delivery systems (GRDDS) have emerged as a promising approach to enhance the bioavailability and therapeutic efficacy of drugs with narrow absorption windows, low solubility at high pH, or local activity in the stomach. Among various GRDDS technologies, the floating in-situ raft system represents a novel and innovative strategy designed to prolong gastric residence time and enable sustained drug release. This system involves a sol-to-gel transition triggered by gastric conditions, forming a buoyant raft-like structure that floats on the gastric fluid. The formulation typically comprises a gelling agent (such as sodium alginate), a gas-generating agent (like calcium carbonate or sodium bicarbonate), and a cross-linking agent that reacts under acidic pH. The formed gel entraps the drug and slowly releases it in a controlled manner, enhancing patient compliance and improving therapeutic outcomes. This review explores the design principles, formulation components, mechanisms, advantages, and recent advancements in floating in-situ raft systems, highlighting their potential in treating gastrointestinal disorders and improving the pharmacokinetic profiles of various drugs.
The evolution of oral drug delivery systems has been transformative in the pharmaceutical sector, addressing challenges related to drug solubility, stability, and targeted therapeutic effects. The major concern for oral delivery is incomplete absorption of drugs due to physiological variability and other parameters [1, 2]. One important factor of physiological variability is the gastric residence time of dosage forms. Since most conventional oral delivery techniques exhibit quick gastric emptying that result in lower bioavailability, gastric retention has acquired lots of attention in recent years. Gastro-retentive dosage forms (GRDFs) usually achieve sustained effects of medication for enhancing oral bioavailability by prolonging its stay in the stomach through gastric retention [3-6]. Incomplete release of drugs, decreased dosage efficiency, and repeated dose frequency are some drawbacks of conventional drug delivery via the gastrointestinal tract (GIT). GRDDS offers numerous advantages, including extending the gastric retention time (GRT) until desired time of duration. It also enhances drug absorption to increase the therapeutic impact of the system. Several gastro-retention technologies were reported to enhance the efficacy of the delivered therapeutic agents. Additionally, GRDDS can aid in controlling the release of the therapeutic agents for extended time at predetermined rate until complete release of API at specific absorption site. In order to eradicate Helicobacter pylori, GRDDS are extremely efficient. Gastro-retention techniques are also useful for medications exhibiting reduced gastric absorption in lower GIT, unstable drug candidates that have very little solubility in basic pH, exhibiting local effect in upper GIT, or possessing shorter half-lives [7-10]. Controlled release GRDDS have been developed using a variety of formulation techniques, including as raft-forming, magnetic, hydrogels, bio/mucoadhesive, expandable, and low and high-density systems. Gastro- retentive dosage forms can be influenced by a number of formulation-related parameters, including polymer types (anionic, cationic and non-ionic polymers), composition of polymer in form of administration, viscosity grade and molecular weight of polymer, and solubility of drug. The physicochemical characteristics of the excipients are also quite important in this formulation. For designing effervescent floating DDS, excipient density and ratio of effervescence producing agents are key components. [11-13]. Among these systems, the raft forming system has been most commonly used as it is one of the most feasible & preferred approaches for achieving a prolonged and predictable drug delivery profile in the GI tract. This system is capable of releasing a drug molecule in a sustained manner affording relatively constant plasma profiles. These hydrogels are liquid at room temperature but undergo gelation when in contact with body fluids or change in pH. The goal for designing this system is to reduce the frequency of dosing or to increase effectiveness of the drug by localization at the site of the action, decreasing the dose required or providing uniform drug delivery. The raft forming system also possesses some potential advantages like simple manufacturing processes, better patient compliance and ease of administration. [14, 15]
Basic Anatomy of Stomach and Its Physiology: [16-20]
During past 4 decades, the idea of gastro retention is known to researchers and is popularly cultured Davis, in 1968, 1st described the concept of floating drug delivery system. To understand the approaches for gastro retention it is necessary to overview gastric physiology and gastric motility.
Anatomy of the Stomach:
Human stomach has a resting volume of 25-50 ml, which can distend up to 1500 ml following a meal. The stomach is a J-shaped organ. It is located in the upper left-hand portion of the abdomen, just below the diaphragm. It occupies a portion of the epigastric and left the hypochondriac region. The main function of the stomach is to store the food temporarily, grind it and then release it slowly into the duodenum. Since the drugs are absorbed in the upper small intestine, it will be beneficial to develop the dosage forms that reside in that region. Anatomically stomach is categories into 3 parts:
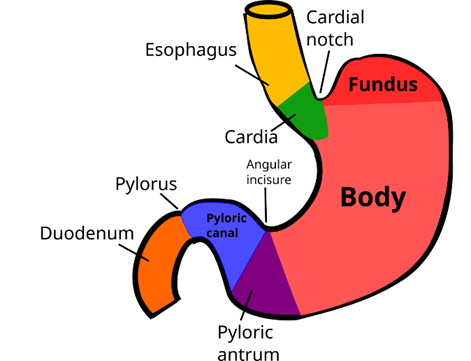
Figure No. 1: Anatomy of Stomach
Physiology of the Stomach:
The GIT is always in a state of continuous motility. There are two modes of motility pattern such as the digestive mode and interdigestive mode.
Gastric emptying occurs during fasting as well as fed states. In case of fasted state an interdigestive series of electrical events occurs in cyclic manner both through the stomach and the small intestine every 2–3 h. This electrical activity is termed as interdigestive myoelectric cycle or migrating myoelectric complex (MMC) [30, 31]. The migrating myoelectric complex (MMC) is further divided into four phases (Fig. 2):
Phase I: It is quiescent period with rare contraction & lasting from 30 to 60 min.
Phase II: It consists of intermittent action potentials & contraction that gradually increases intensity & frequency as the phase progresses. It lasts for 20–40 min.
Phase III: It is for short period of intense, large regular contraction from 10 to 20 min, and it sweeps the undigested material from the stomach to the small intestine. Phase III is termed as ‘housekeeper wave’ as it enables to sweep away all undigested materials out of the stomach & down to the small intestine. Between phase III & phase I of two consecutive cycles a brief transitional phase IV occurs.
Phase IV: Short transitional phase of about 0 to 5 min.
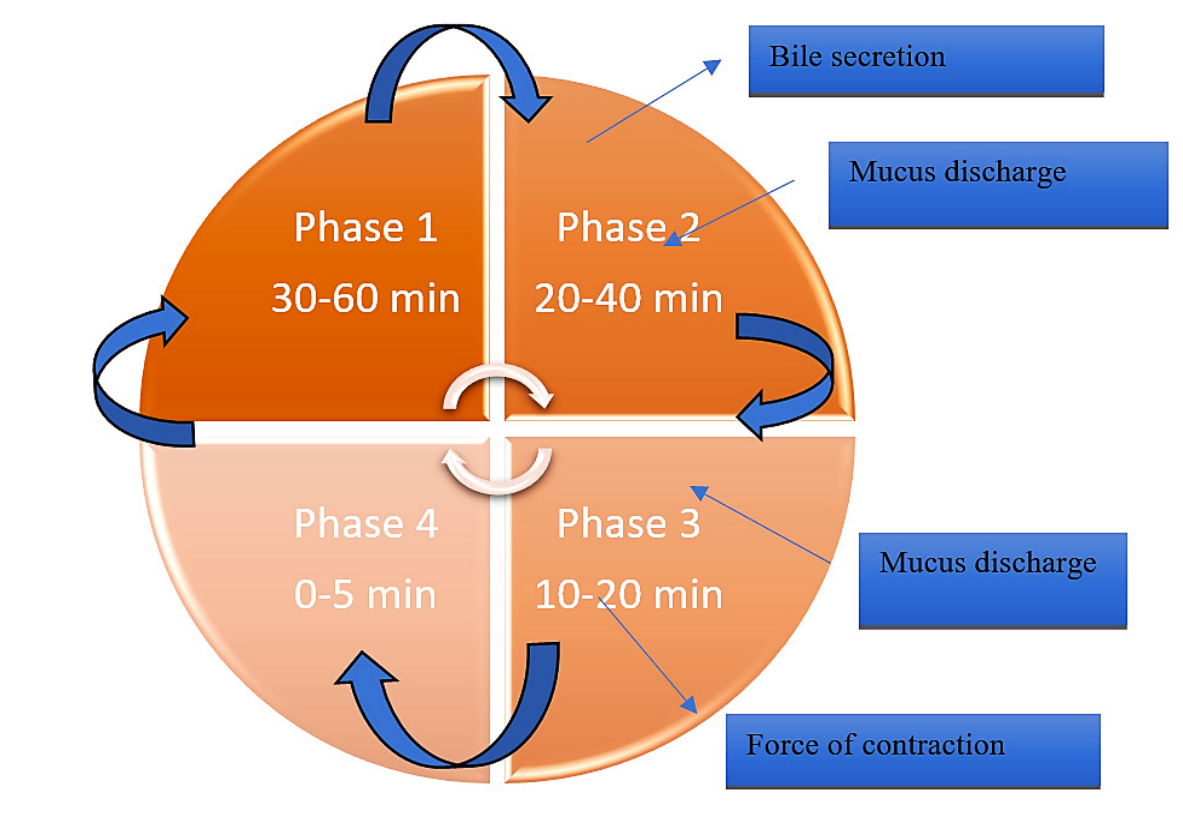
Figure No. 2: Motility phases of GIT
Factors Controlling Gastro Retention Of The Dosage Form [19, 20]
Physical and chemical aspects
Stability based on pH
Medications that are weakly acidic dissolve more quickly at higher pH levels (when more drug exists in its ionized form), whereas medications that are weakly basic often dissolve more slowly at higher pH levels (when more drug exists in its unionized form).
Physiological factors
The kinetics of drug absorption and the total amount absorbed can be significantly altered by physiological factors such as the mechanism of absorption, gender, age, ethnic origin, the human genome, or the health condition of the treated patient. This can change the pharmacokinetics of a drug and potentially its effect when compared to observed behaviour in healthy adults. When comparing patients to healthy populations, the main physiological parameters that are frequently changed are the intestinal surface area, epithelial permeability, gastric emptying rate and pH, transit times across the various intestinal segments, gastrointestinal enzyme and transporter expression and intestinal surface area.
Classification of GRDDS
Many technological approaches have been made to develop a dosage form that can be retained in the stomach. The approaches that have been proposed to increase the retention of an oral dosage form in the upper part of the gastrointestinal tract are described in Fig. 3
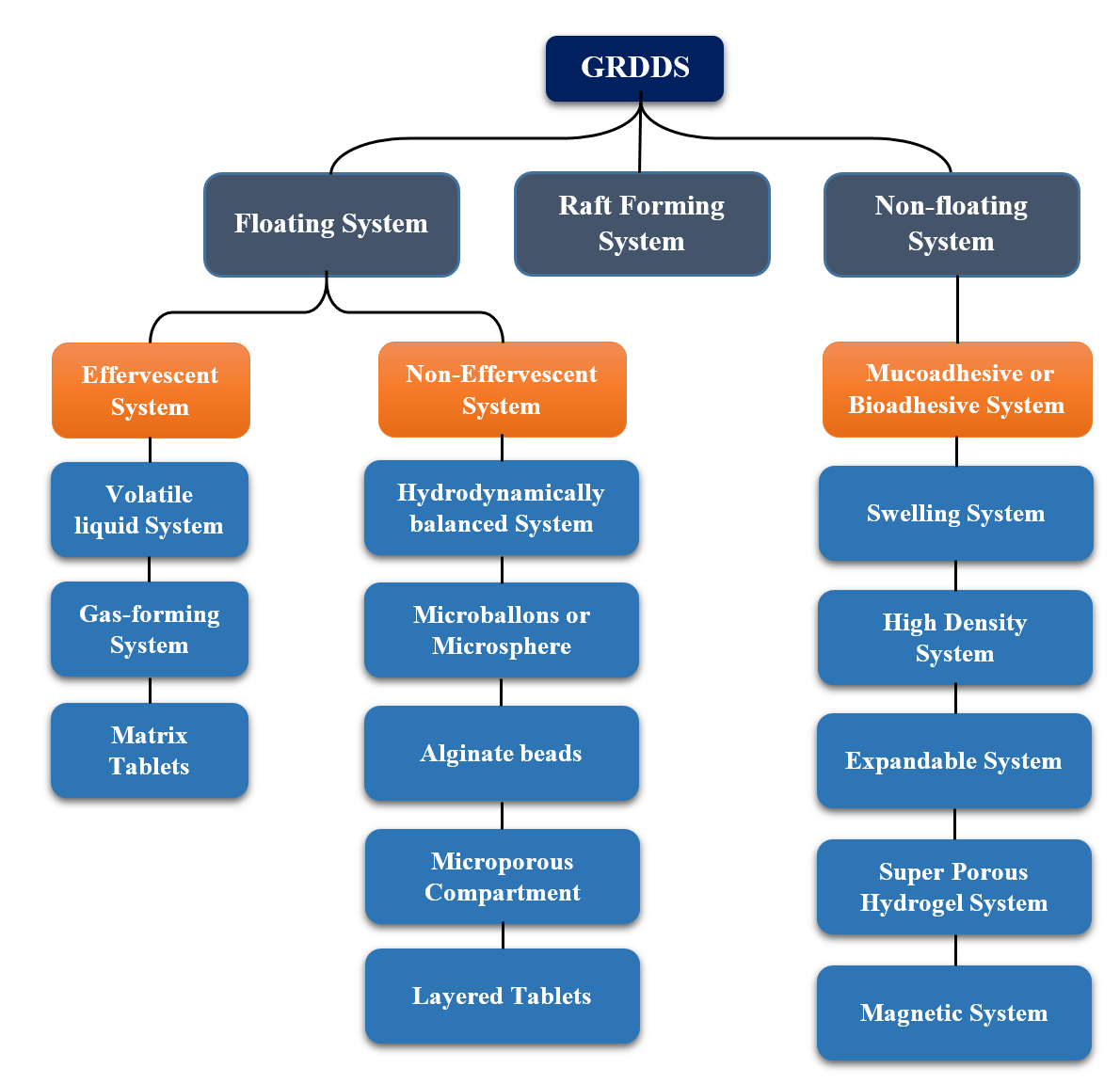
Figure No. 3: Classification of GRDDS
Floating GRDDs (low density)
In 1968 Davis initially reported floating systems, which have a lower bulk density than the stomach content. Low density systems are the most commonly used gastroretentive dosage forms which is also known as floating drug delivery systems [21, 22]. Low-density systems exhibit lower density or higher buoyancy than the gastric content (1.004 g/cm3) which facilitates floating of the drug delivery systems. An increased gastric retention time helps to release the drug in a sustained or controlled manner at a desired rate for a long period of time depending on its buoyancy property. According to this buoyancy mechanism this low-density system can be divided into effervescent and non-effervescent systems [23, 24].
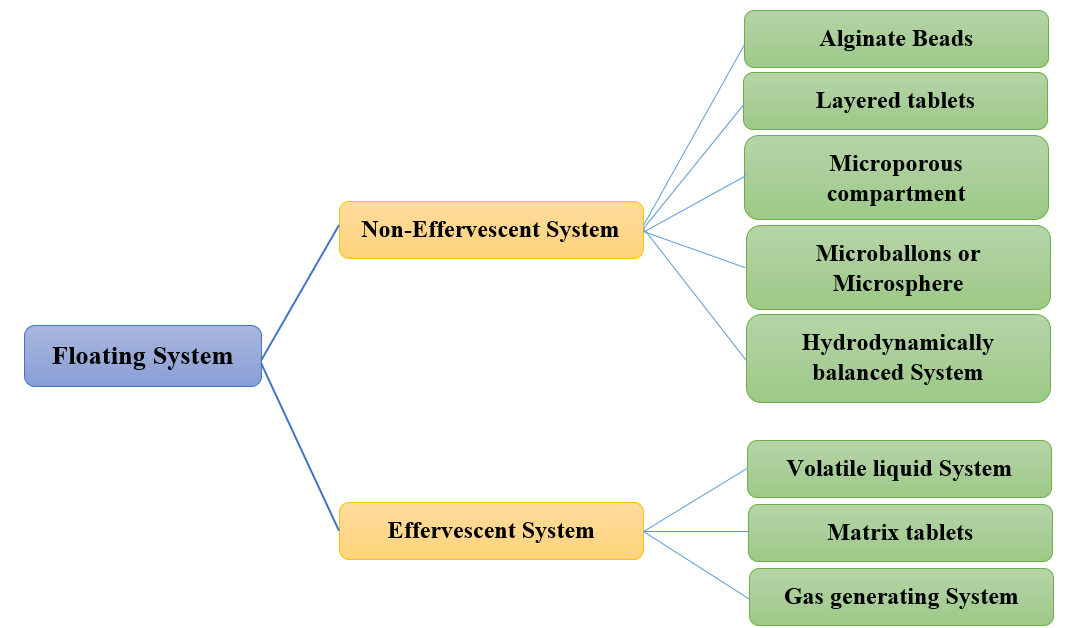
Figure No. 4: Classification of FDDS
Effervescent System:
Effervescent systems use gas generating agents, carbonates (like sodium bicarbonate) and other organic acids (like citric and tartaric acid) in the formulation to create Carbon Dioxide (CO2) gas, which lowers the system's density and causes it to float on the stomach fluid. Alternatively, a matrix with a liquid component can be included to create gas that evaporates at body temperature as shown in Figure 5 like pentoxyfilline. It falls into one of three classes: Volatile liquid system, Gas forming system and Matrix tablet [19].
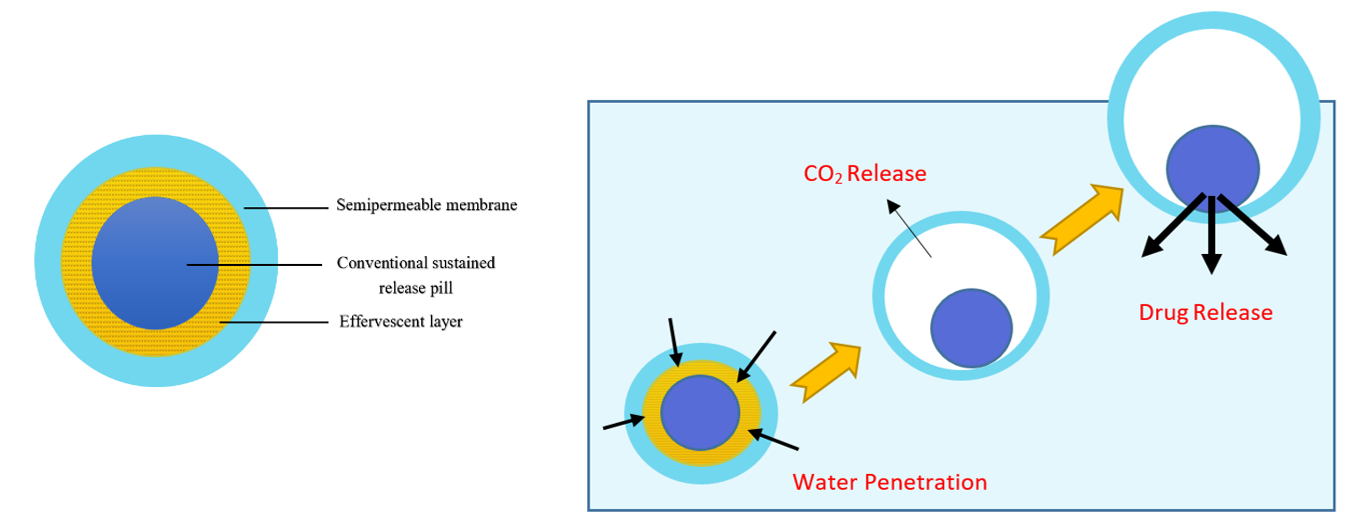
Figure No. 5: Mechanism of effervescent system
Matrix tablets:
The release of drugs via the polymer matrix of the matrix tablet is regulated by the collapsible spring. Resin beads filled with bicarbonate and coated with a substance called ethyl cellulose are commonly used in the preparation of these systems. Water can permeate the covering since it is permeable but not soluble. As a result, the stomach produces CO2, which makes the beads float. A combination of sodium alginate and sodium bicarbonate, extremely swollen hydrocolloids, light mineral oils and floating mini-capsules with a polyvinyl pyrrolidone, lactose and sodium bicarbonate core are some other described methods and materials [19, 25].
These formulations include agents like sodium bicarbonate, citric acid, or tartaric acid, which react with gastric acid to produce carbon dioxide. The released gas gets trapped in a gel matrix, reducing the density of the dosage form, allowing it to float on the stomach contents. Example: Floating tablets, granules, or capsules containing gas-forming agents [26, 27].
These systems include volatile liquids like ether or hydrocarbons encapsulated in a structure. When exposed to body temperature, the liquid vaporizes, producing gas that helps the system float. Note: These are less commonly used due to safety concerns [28].
The non-effervescent floating drug delivery system is based on the mechanism of swelling of polymer or bio-adhesion to mucosal layer in the GI tract. Non-effervescent floating dosage forms use a gel forming or swellable cellulose type of hydrocolloids, polysaccharides, and matrix forming polymers like polycarbonate, polyacrylate, polymethacrylates, and polystyrene. The formulation methods of such dosage forms involve the mixing of the drug with a polymer, which swells in contact with the gastric fluid after oral administration and maintains a relative integrity of shape and a bulk density is less than one within the outer gelatinous barrier [29].
These are spherical particles with a hollow core, prepared using techniques like solvent diffusion or evaporation. Their low density allows them to float and release the drug gradually. Example: Ethyl cellulose-based micro-balloons for prolonged drug release [30].
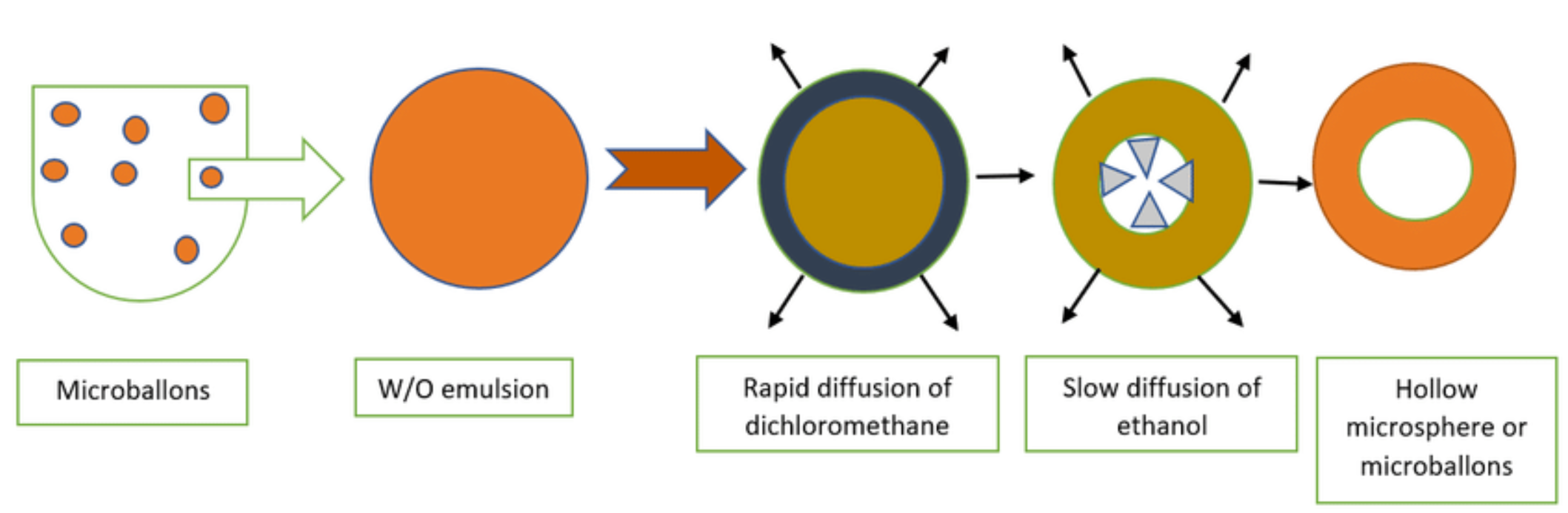
Figure No. 6: Hollow microspheres system
Hydrodynamically Balanced Systems (HBS)
These are formulations composed of gel-forming polymers such as hydroxyl propyl methylcellulose (HPMC). On contact with gastric fluid, the polymer hydrates and swells, forming a gelatinous barrier that keeps the dosage form buoyant. Example: HBS tablets containing drug dispersed in a gel-forming matrix [30].
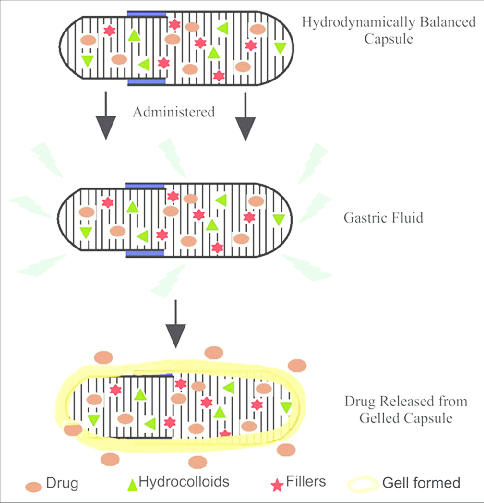
Figure No. 7: Hydrodynamically Balanced Systems
Microporous Compartment Systems
These systems contain a drug reservoir enclosed in a floating chamber. The outer layer contains pores that allow gastric fluid to enter and dissolve the drug, but the internal air compartment ensures buoyancy [22, 30].
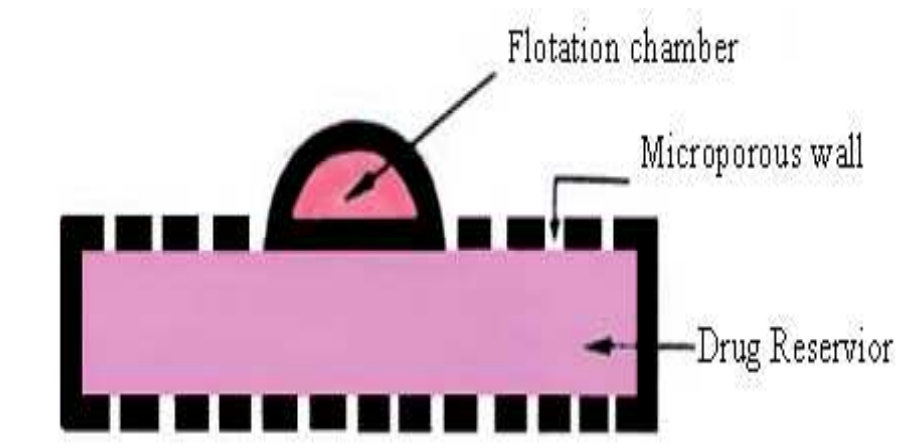
Figure No. 8: Microporous Compartment system of GRDDS
Alginate Beads
Prepared using sodium alginate and cross-linked with calcium ions, these beads can trap air within their matrix. The air pockets allow them to float on gastric fluid. Example: Alginate beads formed via ionotropic gelation technique. [30, 31]
In a layered tablets more than one layer is present, the first layer is called the immediate release layer and it releases the first dose from the system. The second layer is called the sustained release layer and it absorbs the gastric fluid, forming an impermeable barrier on its surface made of colloidal gel and keeping its bulk density below 1 as a result the Gastro retentive time of these tablets is increased and they release the drug for extended period of time [19].
The gastro-retentive drug delivery system's dosage form which does not float in the stomach but rather remains there by a distinct mechanism in the non-floating drug delivery system. This drug delivery system is pH dependant and dissolves at a certain pH. The medication may settle in the stomach, exhibiting bioadhesive and mucoadhesive qualities. The dosage form delivers the drug in a sustained way and at the intended place. The non-floating is further divided into 6 categories bioadhesive or mucoadhesive system, swelling system, high density system, expandable system, super porous hydrogel systems and magnetic system.
This delivery system can enhance the absorption of drugs in a specific site of action by adhering to the mucosal layers present in the region. In this drug, delivery system mucoadhesive polymers are employed which can stick to the epithelial lining present in the stomach wall as shown in Fig. 9. Thus, localization of dosage form occurs which enhances the gastric residence time [32, 33]. There are different mechanisms by which this dosage form can adhere to the mucosal surface i.e., wettability, diffusion, adsorption, electronic and fracture theories. There are various bioadhesive polymers for preparing bioadhesive drug delivery such as chitosan, tragacanth, dextrin, alginates, Hydroxypropyl methylcellulose, cholestyramine, polylactic acid, polyethylene glycol etc. Mucoadhesive polymers may interact with mucin by electrostatic interaction, hydrogen bonding, hydrophobic bonding and disulphide bond formation.
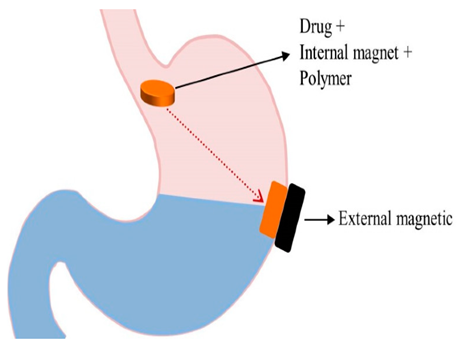
Figure No. 9: Bio adhesive/ Mucoadhesion mechanism
Ideally it should be inert, non-irritating, and non-toxic, which adheres to the mucosal surface exhibiting site specificity The molecular weight of the polymer, shape and flexibility of polymer backbone, density of cross-linking, ability to form H-bond, concentration, polymeric charge, hydration behavior, all together affect the polymer's mucoadhesive characteristics, and contact strength [34-36].
These systems are characterized by the presence of the drug, excipients, and a minute amount of an intramural magnet, with the availability of an extramural magnet placed on the stomach. This extramural magnet is capable of directing the location of the formula containing the internal magnet. Both the magnetic field strength of the extramural magnet and its position may influence the GRT [37]. If the position of the extramural magnet wasn’t accurately specified, the desired outcomes won’t be satisfied. Thus, the appropriate use of these systems will be doubtful.
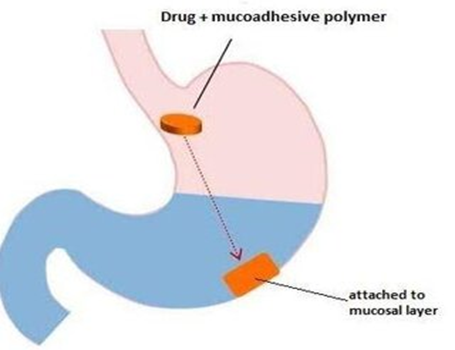
Figure No. 10: Magnetic GRDDS
Super-porous hydrogel systems are described as one category of water-absorbent polymer systems. These systems consist of countless unlocked interconnected pores with an average pore size greater than 100μm. Consequently, they swell rapidly due to water uptake by capillary wetting and reaching an equilibrium size. Thus, such systems acquire enough mechanical strength to withstand the pressure of gastric contraction and increase GRT. This approach has gained wide approval in the controlled?release formulation due to its high mechanical strength and elastic properties. However, the swelling capability of these systems may be affected by the change in pH and may have low mechanical strength of the structure. Examples of highly swellable polymers are croscarmellose sodium and sodium alginate [38-40].
Expandable drug delivery systems have been introduced to extend the gastric retention time by enhancing in their volume or shape. There are three general criteria for proper functioning of the system i.e., for easy oral administration small configuration of dosage form is required, expanded gastroretentive form to obstruct the passage through pyloric sphincter, and reduction in size after release of drug which facilitates evacuation. Due to the capability of interrupting the pyloric sphincter, this system is known as a “plug type system”. This drug delivery system can be expanded by swelling and unfolding of the dosage forms that can vary the volume and shape of it. For swelling and release of drugs from the system, diffusion is the main mechanism. Several highly swellable polymers are used which can swell after absorbing water from gastric content.
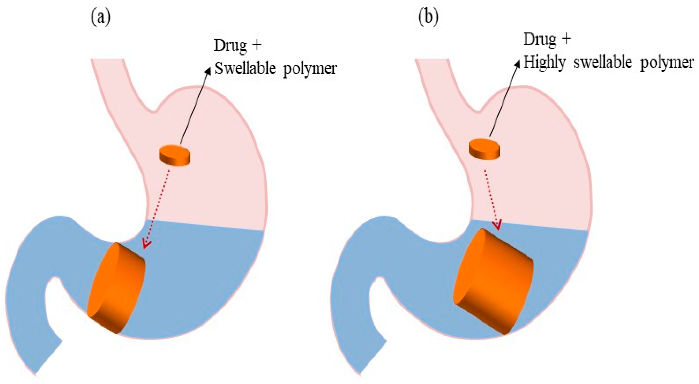
Figure No. 11: Represent Swellable GRDDS
In the unfolding system, the drug and polymer are either compressed or kept in a folded state within a gelatin made capsule shell which dissolves in gastric content and the content is exposed to gastrointestinal medium to absorb water and swell as shown in Fig. 11. [41-43].
Typically, expandable Gastro Retentive Dosage Forms (GRDFs) are design to allow for easy oral intake, an expanded form that is produced in the stomach and blocks passage through the pyloric sphincter and a final small form that is produced in the stomach when retention is no longer necessary, that is, once the GRDF has liberated its active ingredient, allowing evacuation. Either swelling or unwinding in the stomach might cause the enlargement. One of the greatest ways to delay stomach emptying may be through unfolding mechanisms. For the patient's convenience, the unfolding mechanism is often administered as a hard gelatin capsule. Gastric acid causes the carrier to disintegrate in the stomach, releasing the GRDF system, which then unfolds or stretches out to take on its expanded structure. Long periods of time should be maintained by the carrier's unfolded qualities [44].
Raft forming systems are mostly taken into consideration for the administration of antacids and other drugs for gastro-infection and gastro-intestinal illnesses. When the gel-forming solution comes into touch with gastric fluid, it expands and forms a viscous, compact gel with trapped CO2 bubbles that forms an inflatable layer on top of the fluid and releases the medicine gradually into the stomach. As a result, these rafts forming system have a longer Gastro retentive time and release the medication over a longer duration of time as shown Figure 12. This technique can provide comparatively stable plasma profiles by continuously releasing a pharmacological molecule. At room temperature, these hydrogels are liquid, but when they come into touch with bodily fluids or experience a pH shift, they gel. The purpose of this system's design is to either decrease the frequency of dosing or enhance the effectiveness of the medication by localizing it at the site of action, lowering the dosage needed, or delivering the medication consistently. Additionally, the raft forming technology has several potential benefits, such as easier administration, improved patient compliance and straightforward production procedures [45-46].
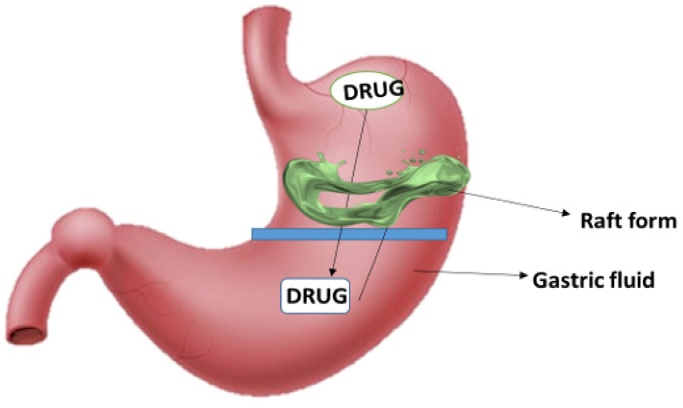
Figure No. 12: Raft system approach
Raft Formation Based on Physical Mechanism [20]
Bloating: In situ gel formation is the process by which materials expand to cover a desired space after absorbing water that comes from the surrounding environment.
Diffusion: It involves the precipitation or solidification of the polymer matrix due to the solvent from a polymer solution diffusing into the surrounding tissue. N-Methyl Pyrolidone is a mixture of polymers that may be used in this situation.
The Raft Forming System's Design
The raft forming system's formulation is influenced by the drug's physicochemical characteristics, the patient population, the ailment that has to be treated and marketing preferences. Anatomical and physiological aspects include membrane transport and tissue fluid pH; formulation factors include pH, gelation temperature, viscosity, osmolarity and spreadability; physicochemical factors include molecular weight, lipophilicity and molecular charge. In order to ensure that the dose form is stomach retained the following requirements must be met by the dosage form [47].
They are listed in the following order: [20, 47]
Formulation Strategies of Raft Forming System
Ingredients used in the Formulation of the Raft Forming System:
An appropriate candidate should be selected for the formulation of controlled release gastro-retentive formulation. Various ingredients used in the formulation of such system are gel forming agent and alkaline bicarbonates or carbonates, which are responsible for the formation of a less dense system, which floats on the gastric fluids. [48, 49].
Drugs Selection Criteria for the Raft Forming System:
Raft forming systems have received much attention for the delivery of antacids and drug delivery for gastrointestinal infections and disorders. The raft forming system is the potential approach for heartburn and esophagitis. This system is suitable for acid soluble drugs that are poorly soluble or unstable in intestinal fluids [50].
Thus, the criteria of the drug to be considered for the selection of the drug for gastro retention are as follows: [20, 51, 52]
Polymer used for formulation
Polymer used for formulation Various polymers are employed in floating drug delivery systems so as to target the delivery of the drug to a specific region in the gastrointestinal tract i.e. stomach. Various natural and synthetic polymers are used in the formulation of the raft forming drug delivery system. Natural polymer such as alginic acid, guar gum, gellan gum, xyloglucan, pectin, chitosan etc. and synthetic polymer such as poly(DL lactic acid), poly(DL-lactide-co-glycolide) and poly-caprolactone, HPMC etc. are used for formulation development of the raft forming drug delivery system [53].
A polymer used for in situ gels should have the following characteristics [12, 54]
Approaches used for the formulation of the raft forming drug delivery system
Raft forming drug delivery systems are a revolution in oral drug delivery. These systems are liquids at room temperature but undergo gelation when comes in contact with body fluids or change in pH. These have a unique property of temperature dependent and cation-induced gelation. Gelation involves formation of the double helical junction zones followed by aggregation of the double helical segments which form three dimensional networks by complexation with cations and hydrogen bonding [54].
Different approaches based on their mechanisms used for triggering the raft formation in the GIT are as follows
Swelling: Formation of a gel occurs when the liquid effervescent system comes in contact with gastric fluid. In situ formation of gel occurs when materials absorb water from the surrounding environment and expand to occur at the desired space. Swelling of the polymer occurs by absorption of water which further causes formation of the gel. Certain biodegradable lipid substance such as myverol 18–99 (glycerol mono-oleate), is a polar lipid that swells in water to form lyotropic liquid crystalline phase structures. It has some bioadhesive properties and can be degraded in-vivo by enzymatic action [55].
Diffusion: Diffusion is the method which involves diffusion of a solvent from polymer solution into surrounding tissue, which further results in precipitation or solidification of polymer matrix. Solution of polymer that can be used for such mechanism is N-methyl pyrrolidone (NMP) [56]
Ionic crosslinking: There are various polysaccharides that undergo phase transition in the presence of various ions. Polysaccharides falling into the class of ion-sensitive ones are most widely used [20]. Ion sensitive polysaccharides such as carrageenan, gellan gum (Gelrite®), pectin, and sodium alginate undergo phase transition in the presence of various ions such as k+, Ca+, Mg+, and Na+. Various polysaccharides undergo gelation in the presence of various monovalent, divalent cations. Alginic acid undergoes gelation in the presence of divalent/polyvalent cations like Ca2+ due to the interaction with guluronic acid block in alginate chains. K-carrageenan forms rigid, brittle gels in response to small amount of K+, i-carrageenan forms elastic gels mainly in the presence of Ca2+. Gellan gum commercially available as Gelrite® is an anionic polysaccharide that undergoes in situ gelling in the presence of mono- and divalent cations, including Ca2+, Mg2+, K+ and Na+. Gelation of the low-methoxy pectin can be caused by divalent cations, especially Ca2+ [57].
pH dependent gelling: Formation of gel in the system also occurs due to change in the pH of the medium. Various pH dependent polymers are used which cause the formation of in situ gel in the system. Various polymers such as PAA (Carbopol®, carbomer) or its derivatives, polyvinylacetal diethylaminoacetate (AEA), mixtures of poly (methacrylic acid) (PMA) and poly (ethylene glycol) (PEG) show change from sol to gel with change of pH. Swelling of hydrogel increases as the external pH increases in the case of weakly acidic (anionic) groups, but decreases if polymer contains weakly basic (cationic) groups. Mixtures of poly(methacrylic acid) (PMA) and poly(ethylene glycol) (PEG) also have been used as a pH sensitive system to achieve gelation. pH sensitive polymer can be neutral or ionic in nature. The anionic networks contain negatively charged moieties, cationic networks contain positively charged moieties, and neutral networks contain both positive and negatively charged moieties. In the case of anionic polymeric network containing carboxylic or sulphonic acid groups, ionization takes place, as the pH of the external swelling medium rises above the pKa of that ionizable moiety [50, 58].
Temperature dependent gelling: These hydrogels are liquid at room temperature (20 °C–25 °C) and undergo gelation when in contact with body fluids (35 °C–37 °C), due to an increase in temperature. This approach exploits temperature-induced phase transition. Some polymers undergo abrupt changes in solubility in response to increase in environmental temperature (lower critical solution temperature, LCST) [59]. At the LCST, hydrogen bonding between the polymer and water becomes unfavorable, compared to polymer–polymer and water–water interactions, and an abrupt transition occurs as the solvated macromolecule quickly dehydrates and changes to a more hydrophobic structure. Alternatively, some amphiphilic polymers that self-assemble in solution, show micelle packing and gel formation because of polymer–polymer interactions when temperature is increased [60]. Temperature-sensitive hydrogels are probably the most commonly studied class of environment-sensitive polymer systems in drug delivery research. Polymers such as pluronics (poly(ethylene oxide)– poly(propylene oxide)–poly(ethylene oxide) (PEO–PPOPEO Triblock), polymer networks of poly(acrylic acid) (PAA) and polyacrylamide (PAAm) or poly(acrylamide-co-butyl methacrylate) are commonly used for temperature sensitive hydrogels formation [120]. A positive temperature-sensitive hydrogel has an upper critical solution temperature (UCST), and such hydrogel contracts upon cooling below the UCST. Polymer networks of poly(acrylic acid) (PAA) and polyacrylamide (PAAm) or poly(acryl amide-co-butyl methacrylate) have positive temperature dependence of swelling [61, 62].
Preparations of Raft forming system
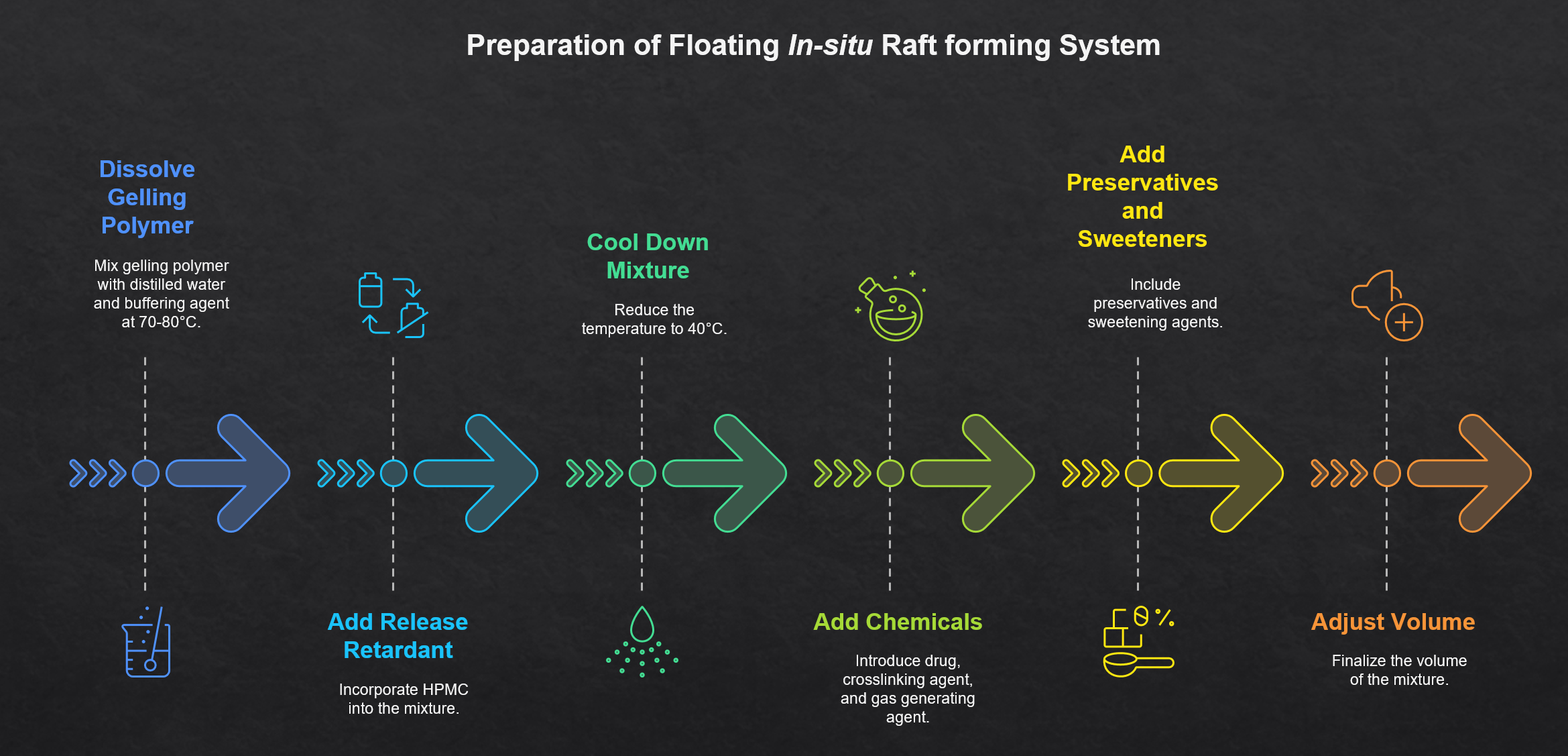
Figure No. 13: Perpetration of Raft system
Advantages of Raft forming GRDDS [19, 20, 48, 63]
Limitation of Raft forming GRDDS [19, 20, 34, 63]
Evaluation parameters of the Raft forming system
The clarity of formulated solution is determined by visual inspection under black and white background [64, 65].
This is an important parameter to be evaluated for the raft forming system. The viscosity and rheological properties of the polymeric formulations, either in solution or in gel made with artificial tissue fluid (depending upon the route of administrations) were determined with a different viscometer. The viscosity can be determined with Brookfield rheometer or some other type of viscometers such as Ostwald's viscometer [20, 64].
This is used to determine gelling property of prepared formulation. This parameter can be evaluated using a rheometer. In this test a specified amount of gel is prepared in a beaker, from the sol form. Gel containing beaker is raised at a certain rate, then pushing a probe of rheometer slowly through the gel. The changes in the load on the probe can be measured as a function of depth of immersion of the probe below the gel surface [19, 20].
Raft forming system is an effervescent liquid which involves the formation of viscous cohesive gel in contact with gastric fluids. The sol-gel transition temperature is the temperature at which the phase transition of sol meniscus is first noted when kept in a tube at a particular temperature and then heated at a certain rate. While gel formation is denoted by an absence of movement of the meniscus on tipping the tube and gelling time is the time for the first appearance of gelation [66].
This test is performed to study the compatibility of ingredients by using Fourier transform infrared spectroscopy. During the gelation process, the nature of interacting forces can be evaluated using this technique. As well, Differential scanning calorimetry can also be used to observe if there are any changes in thermograms as compared with the pure ingredients used thus indicating the interactions [64, 67].
It is tested to measure the time taken by the dosage form to float on the top of the dissolution medium, following it is placed in the medium. Both the time between the introduction of the dosage form and its buoyancy on the simulated gastric fluid (Floating lag Time) and the time during which the dosage form remains buoyant were measured (known as floating time) [38, 68].
The in vitro drug release of the raft forming system is carried in 0.1 N HCl from 0 to 8 h by USP type-II apparatus at 50 rpm. The dissolution medium used is 900 ml of simulated gastric fluid (0.1N HCl, pH 1.2) and the temperature is maintained at 37±0.2 °C. At each time interval, a precisely measured sample of the dissolution medium is pipette out and replenished with a fresh medium. Drug concentration in the aliquot can be determined by spectrophotometrically [20, 69].
Marketed Formulation of the Raft Forming System
There are many formulation of the Raft forming system are tabulated in Table No. 1 [11, 15, 19, 20]
Table No. 1: Marketed formulation of Raft system
|
Brand Name |
Active Ingredient |
Company |
Delivery system |
|
Liquid Gaviscon® |
Al hydroxide (95mg) and Mg carbonate (358mg) |
Glaxos Mith Kline India |
Effervescent floating liquid alginate preparation |
|
Topalkan® |
Al-Mg antacid |
Pierre fabre drug, France |
Effervescent floating liquid alginate preparation. |
|
Valrelease® |
Diazepam (15mg) |
Hoffmann laroche, USA |
Floating Capsule |
|
Conviron |
Ferrous sulphate |
Ranbaxy, India |
Colloidal gel forming FDDS |
|
Cifran od® |
Ciprofloxacin (1mg) |
Ranbaxy, India |
Gas-generating floating tablet |
|
Cytotec® |
Misoprostal (100Mcg/200mcg) |
Pharmacia, USA |
Bilayer floating capsule |
|
Oflin od® |
Ofloxacin (400mg) |
Ranbaxy, India |
Gas-generating floating tablet |
|
Glumetza |
Metformin hydrochloride |
Depomed |
Gas-generating floating tablet |
|
Ulge-Raft |
Sod Alginate, Sod Bicarbonate, Calcium Carbonate |
Alembic |
Oral suspension |
CONCLUSION
In the recent time various drugs are formulated as Gastro retentive drug delivery system with a motive of sustained and control release of the drug for the local and systemic effects. GRDDs contain immense promise for the future of the drug delivery. In traditional oral dosage forms, drugs that have a narrow absorption window in the gastrointestinal tract often exhibit limited bioavailability. This is mainly due to incomplete drug release and a brief residence time at the absorption site. To address this limitation, advanced drug delivery systems have been designed to enhance the oral uptake of such drugs. Gastroprotective drug delivery is an emerging area focused on improving drug retention in the stomach to enhance bioavailability. Various systems like floating, high-density, mucoadhesive, expandable, swelling, and ion-exchange have been explored. Among them, raft-forming systems are particularly effective, as they float on gastric fluids and enable prolonged drug release at the absorption site. This enhances therapeutic efficacy, reduces dosing frequency, and is patient-friendly, especially for children and the elderly. Despite challenges due to the variable nature of the human GI tract, raft systems offer a promising solution for sustained gastric drug delivery.
ACKNOWLEDGMENTS
We are very grateful to Mr. Lakshya Veer Singh and Aditya Kumar for their appropriate and constructive suggestions to improve this review article.
REFERENCES



Dr. KVV Satyanarayana*, Dr. Vidhya Kuppili, CH. Tejaswi, Dr. K. Ravi Naini, Satya Varaprasad, Dr. VVL Narasimha Rao, A Clinical Study on Iris Thickness in Asians and Africans, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 8, 1947-1966 https://doi.org/10.5281/zenodo.16901002
 10.5281/zenodo.16901002
10.5281/zenodo.16901002
