Minerva College of Pharmacy, Indora (H.P)
Lipid nanoparticles (LNPs) have gained considerable attention as advanced drug delivery carriers due to their biocompatibility, ability to encapsulate diverse therapeutic agents, and potential for controlled and targeted release. Recent developments have focused on integrating LNPs with microneedle (MN) patch delivery systems, creating a minimally invasive and highly efficient transdermal platform. Microneedles overcome the barrier function of the stratum corneum by creating microchannels that enable direct delivery of LNP-encapsulated drugs into the viable epidermis or dermis, thereby enhancing bioavailability and bypassing first-pass metabolism. This combined approach effectively addresses major limitations of conventional delivery routes, including poor drug solubility, instability of biologics, and low patient compliance. Recent studies demonstrate successful incorporation of LNPs into dissolving, hydrogel-forming, and coated microneedle systems for the delivery of vaccines, peptides, nucleic acids, anticancer agents, and other biologics. This review provides a comprehensive overview of recent advances in LNP-loaded microneedle patches, with emphasis on formulation strategies, fabrication techniques, stability considerations, in vitro and in vivo performance, and therapeutic applications. Despite promising outcomes, challenges such as maintaining microneedle mechanical strength, ensuring nanoparticle stability during fabrication, large-scale manufacturing, and regulatory standardization remain significant. Ongoing advancements in materials science, nanotechnology, and microneedle fabrication are progressively addressing these limitations. Overall, LNP-integrated microneedle patches represent a promising transdermal drug delivery system with significant potential for personalized medicine, self-administration, and next-generation vaccine and biologic delivery.
A collection of physicochemical technologies known as "drug delivery systems" (TDDS) are capable of controlling the release and distribution of pharmacologically active substances into cells, tissues, and organs in order to maximize their effectiveness [1]. With a surface area of 20 square feet and essential functions, the human skin is the largest organ in the body [2]. It serves as a barrier between the internal and external environments, keeping harmful substances out of the body, shielding it from infections and the elements, controlling body temperature, minimizing water loss, and permitting touch, heat, and cold sensations [3]. TDDS is a painless systemic drug delivery technique that applies a medication formulation to healthy, intact skin. Microneedles have been used extensively to improve the transdermal delivery of drug molecules, particularly as a pre-treatment where the drug can diffuse through remaining skin holes from a topical formulation [4].
Nanoparticles have been widely used for delivering a wide variety of drugs that are applied for multiple disease treatments, such as diabetes, wound healing, and cancers, due to their unique advantages, which include protection from enzyme degradation, a prolonged half-life of drugs, desired targetability, and the ability to achieve sustained release [5]. However, most medications cannot reach the required therapeutic levels through the skin because of the stratum corneum's thick and impermeable outer layer, which limits the use of transdermal technology. Only lipophilic, low molecular weight, potent drugs can be administered transdermally due to the barrier that the human skin presents [6]. Several businesses used nanotechnology and made previously unheard-of cost investments during the COVID-19 pandemic to quickly develop vaccines based on lipid nanoparticles. The ability to preserve the active ingredients, create customized treatments, and target them are the primary factors that make this technology possible [7].
The ability of microneedles (MNs) to deliver drug-loaded nanoparticles transdermally has garnered significant attention because it can avoid gastrointestinal tract enzymatic degradation and improve patient compliance by lowering the pain associated with hypodermic injection, even though drug-loaded nanoparticles can be administered orally, intravenously, or ocularly for therapeutic purposes (Table 1). Development of delivery systems that intend to aid penetration of such drugs through deeper layers has been increasing in the past 20 years, extending the applications of these hydrophilic and macromolecule drugs for the treatment of deep tissue and dermatologic diseases. Many physical or pharmaceutical strategies, such as sonophoresis, electroporation, iontophoresis, microneedles (MNs), chemical enhancers [8].
TABLE 1: The advantages and disadvantages of different administration routes for drug-carrying nanoparticles.
|
Administration Routes |
Microneedles |
Oral |
Intravenous |
Topical |
|
Advantages
|
No pain, self-administration, enabling localized drug delivery, high bioavailability, increase patient compliances, reduced side effects |
Easy to use, no pain |
High bioavailability |
Easy to use, no pain |
|
Disadvantages |
Limited drug dose |
Low bioavailability, poor distribution, undesirable side effects |
Pain, reduced patient compliance, systemic toxicity |
Poor bioavailability, low absorption, only for small lipophilic drugs use |
The pharmaceutical industry is currently very interested in MN arrays because of their many benefits over more conventional drug delivery techniques like parenteral and oral administration. The ability to deliver the active pharmaceutical ingredient painlessly, avoid hepatic first-pass metabolism, and expand the variety of drugs that can be administered intradermally and transdermally are a few advantages [9]. Recently, some review papers have reported on MNs; this work focused on this topic differently, including the design and summary of drug-carrying nanoparticles integrated with MNs. In this review, we first present the four different kinds of drug-carrying nanoparticles: inorganic, polymeric, lipid, and nanocrystal nanoparticles. Next, we discuss MN-based approaches that have been used to facilitate the transdermal delivery of these nanoparticles for drug delivery. Lastly, we offer our thoughts on the possible application of MNs-mediated skin nanoparticle delivery [10, 11, 12].
Transdermal drug delivery:
By applying a drug formulation to healthy skin, transdermal drug delivery is a painless way to administer medications systemically. Without accumulating in the dermal layer, the medication first penetrates the stratum corneum before moving on to the deeper epidermis and dermis. The skin was first used as an administration site for long-term drug delivery in the tenth century, and TDDS is a crucial component of innovative drug delivery systems. One of the most dependable and efficient methods is transdermal drug delivery. One of the most inventive and successful drug delivery methods nowadays is the transdermal route. Over 20 years have passed since the initial introduction of this system. Major pharmaceutical companies were extremely excited and interested in the technology [13]. An adhesive medication patch that is applied over the skin to deliver a precise dosage of medication through the skin and into the bloodstream at a predetermined rate of release is known as a transdermal patch. The most widely used transdermal system on the market today is primarily based on semi-permeable membranes known as patches. Transdermal drug delivery systems (TDDS), sometimes referred to as "transdermal patches" or "skin patches," are dosage forms intended to administer a therapeutically effective dosage of medication through the patient's skin and into their bloodstream [14].
Skin:
About one-third of the blood that circulates through the body passes through the skin, which has a surface area of two square meters on average for an adult.
The skin is a complex organ with numerous histological layers. The epidermis, dermis, and hypodermis are the three main tissue layers that are typically used to describe it (Figure 1). The stratum corneum, the outermost layer of the epidermis that is exposed to the outside world, is one of the five anatomical layers that make up the epidermis under a microscope.
It is estimated that each square centimeter of human skin has between 40 and 70 hair follicles and 200 to 250 sweat ducts.
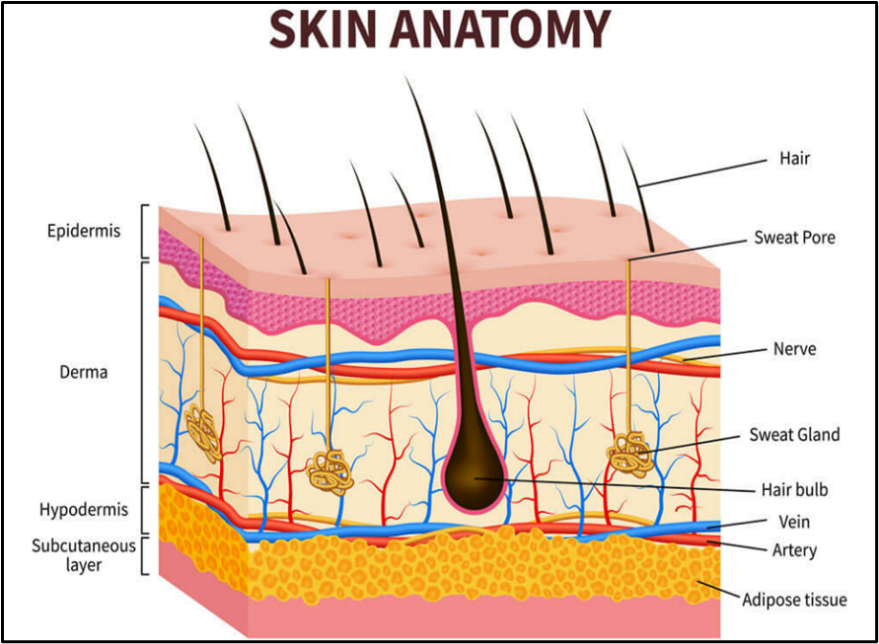
Figure 1: Structure of skin
Lipid nanoparticles:
Phospholipids are a crucial component of lipid and lipid-based drug delivery systems due to their many qualities, including their amphiphilia, biocompatibility, and multifunctionality. The SLN delivery system has arisen as a result of the numerous disadvantages of liposomes, lipospheres, and microsimulation carrier systems, including their challenging large-scale manufacturing, low percentage entrapment efficiency (% EE), and complex production process. SLNs typically have a diameter of 50–1000 nm and a spherical form. Lipids, which are solid at room temperature, emulsifiers, and occasionally a combination of the two, active pharmaceutical ingredients (APIs), and a suitable solvent system are the main components of SLN formulation [15].
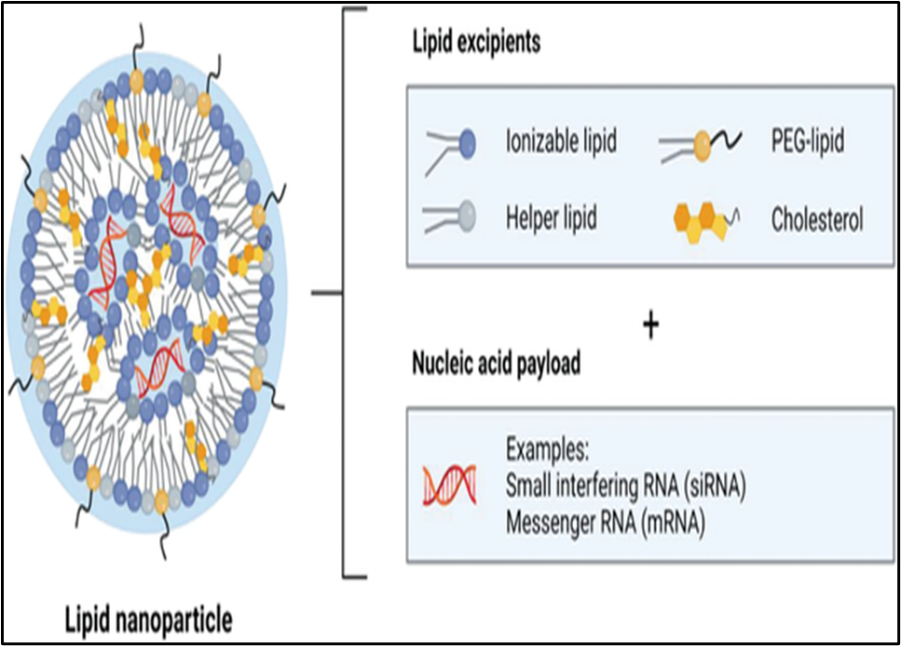
Figure 2: Structure of lipid nanoparticles
Lipids are thought to be a more physiological option and are anticipated to have a high level of biocompatibility when compared to many other materials used as drug carriers, especially polymers. Solid lipid nanoparticles, out of all the varieties, are at the forefront of the quickly evolving field of nanotechnology and have a number of potentials uses in research, clinical medicine, drug delivery, and other diverse sciences [16].
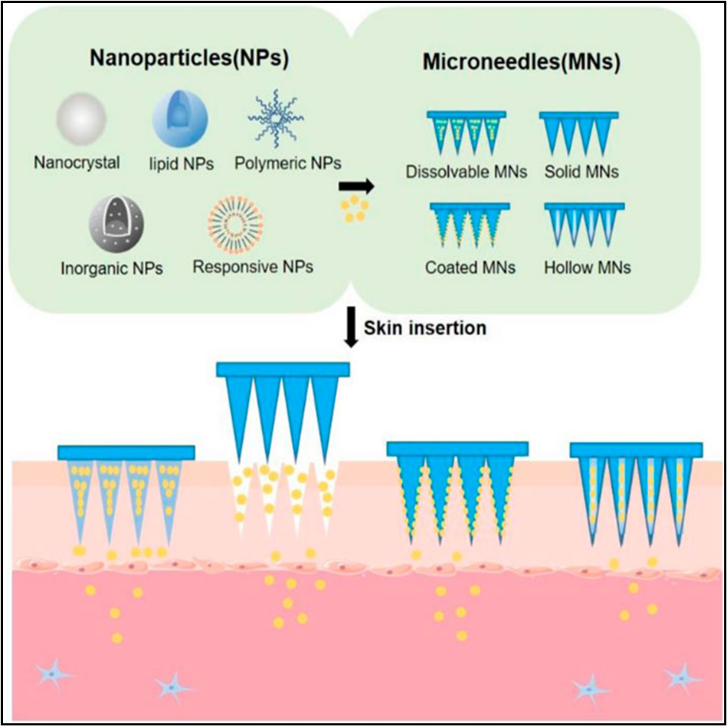
Figure 3: The schematic representation of MNs-mediated nanoparticle transdermal delivery
Microneedle
Due to its many advantages, such as avoiding the gastrointestinal tract's degradation of therapeutics, avoiding the liver's first-pass metabolism (for oral delivery), and avoiding the invasive and uncomfortable intravenous drug delivery method, this treatment method has drawn a lot of interest from researchers (figure 4). Since then, microneedles have been extensively developed for TDD along with advances in microfabrication manufacturing and pharmaceutics technologies. According to differences in drug delivery pattern, microneedles can be divided into solid, hollow, dissolved, or coated microneedles [17].
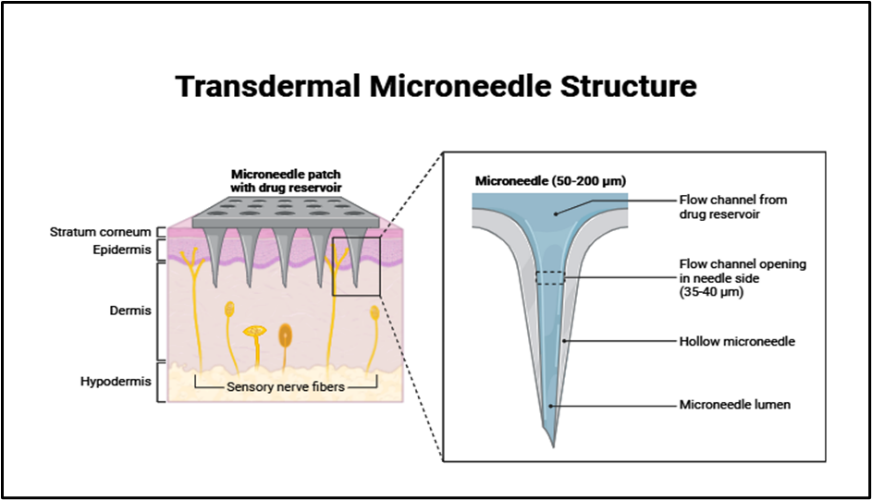
Figure 4: Structure of Transdermal Microneedle patch
Mechanism
Invasive and supporting components make up microneedles. Numerous needles with lengths ranging from 25 to 2000 microns make up the invasive portion. A base plate serves as the supporting component, giving the sharp needle tips uniform mechanical support so they can efficiently pierce the SC [18]. The pain increases with the length of the microneedle.
Furthermore, the insertion and penetration of the microneedle for drug delivery greatly depend on its geometric shape [19]. The poke and flow method uses either passive or active diffusion to release medication from hollow needles (under any kind of external pressure). Coated MNs that employ the coat-and-poke method enter the skin's epidermis and then release a moisture-based coated drug formulation. Finally, the entire MN disintegration process is followed by the release of the medication in the poke and release method of dissolving MNs [20]. It avoids the barrier layer by penetrating the stratum corneum. When the medication reaches the site of action, it immediately enters the epidermis or upper dermis layer, enters the systemic circulation, and exhibits a therapeutic response [21]. Mechanism of microneedle (figure 5).
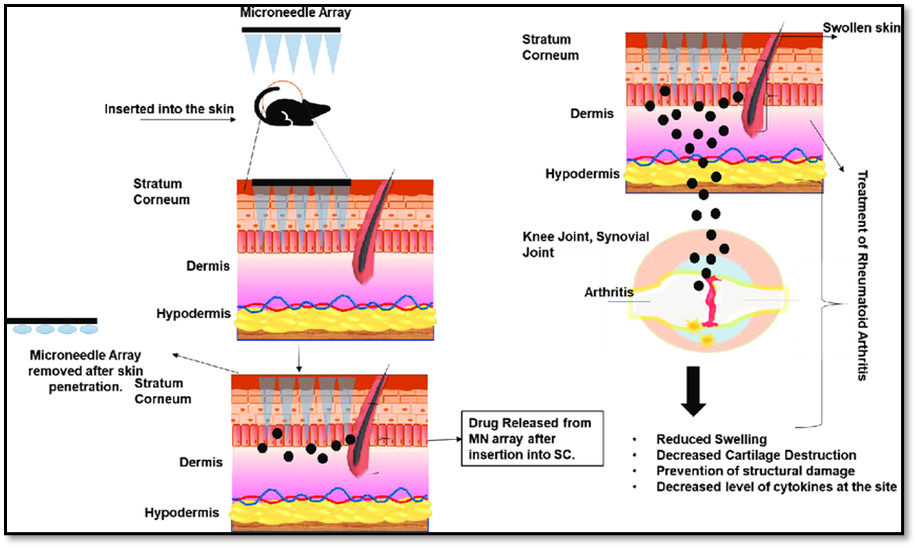
Figure 5: Mechanism of microneedle
MATERIAL AND FABRICATION
Aqueous blends comprising 7.5% w/w PEG 10,000 and 15% w/w Gantrez1 S-97 were used to create MN arrays. Carefully, the formulation (0.5 g/cm2) was syringed onto silicone micro molds (600mm needle height, 14 ~14 needles on a 0.5 cm2 area). After 15 minutes of applying positive pressure (3–4 bar) to the formulation, the needle cavities were filled. MN arrays were heated to 80°C for 24 hours to crosslink them by esterification after being allowed to dry for 48 hours at room temperature [22]. The dissolvable material HA was selected as matrices for MN because it is a skin intrinsic composition with high security [23]. While designing MNs through any suitable method, the size and shape of MNs in (Table 2) and (Figure 6) [24].
When compared to hypodermic needles, MNs have the advantage of reducing pain (26G). However, a patient's perception of pain may be influenced by the size and quantity of MNs in a patch. According to Gill et al., pain may be lessened if the length and quantity of MNs are Reduced [25]. The size and shape of MNs should be taken into account when designing them using any appropriate technique because these factors can affect how well drugs are delivered [26].
Table 2: Material for the fabrication of microneedle
|
Materials |
Advantages |
Disadvantages |
Application |
|
Silicon |
Biocompatible, hard, mature fabrication techniques |
Sharp waste Brittle |
Solid, Coated, Hollow microneedles |
|
Ceramic materials |
Natural porous |
Long fabrication time, significantly brittle |
Hollow, Dissolving microneedles |
|
Glass |
Chemically inert, transparent and cheap. |
Cumbersome fabrication, brittle |
Hollow microneedles |
|
Metals |
Biocompatibility, high conductivity, have catalytic activity for some nanometals. |
High cost for noble metals, allergic risk |
Solid, Coated, Hollow microneedles |
|
Polymers |
Biodegrable or Swellable, easy fabrication |
Low mechanical strength |
Solid, Coated, Hollow, Dissolving, Swellable microneedles |
|
Carbohydrates |
Biodegradable, biocompatible |
High processing temperature, low mechanical strength and hygroscopicity. |
Dissolving microneedles |
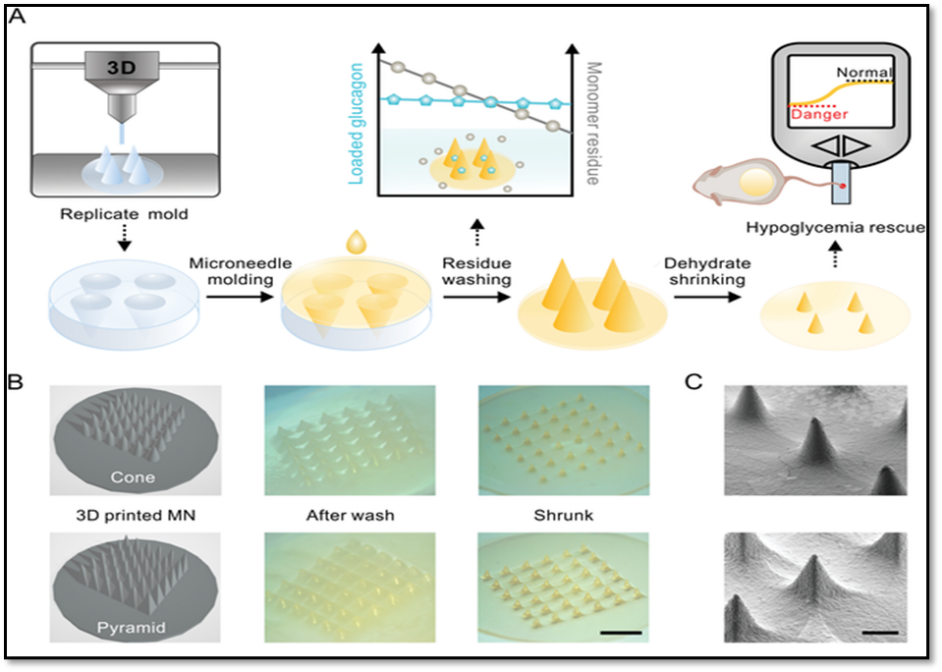
Figure 6: (A) Schematic illustration of the shrinking fabrication process. B) 3D design drawing and images of the 1.5 cone (top panel) and 1.5 pyramid?shaped (bottom panel) MN patch before (middle) and after shrinkage (right). Scale bar, 3 mm. C) SEM images of the 1.5 cone (top) and 1.5 pyramid (bottom) shaped MN patch. Scale bar, 500 µm. The D) tip base width and E) needle height change of the different MNs after full shrinkage.
Types of Microneedles
Different types of microneedles fabricated and investigated for their application in drug delivery are solid, coated, dissolving, hollow, and hydrogel microneedles. Different types of microneedles with their unique properties are displayed in (figure 5). Each type of microneedle has its own way of delivering the drug into the epidermis. Some are used just to create pores in stratum corneum, some are precoated with the drug solution on their surface, some are dissolvable and some are prefilled with the drug solution [27, 28, 29].
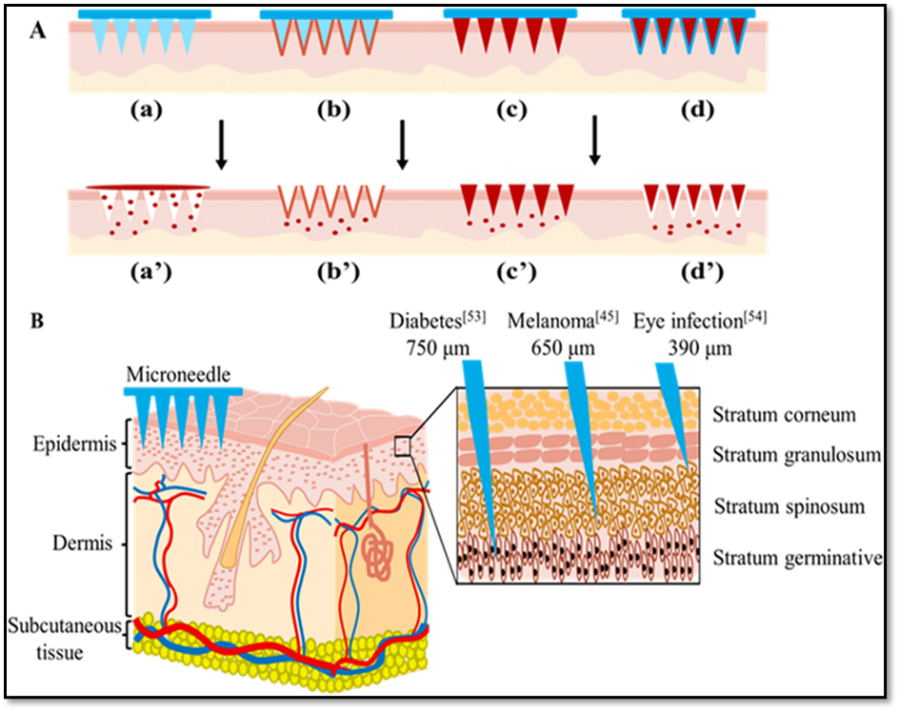
Figure 7: (A) Schematic diagram of different types of microneedles for gene-drug delivery. (a)-(d): Microneedles are inserted into the skin. (a): Solid microneedles. (b): Coated microneedles. (c): Soluble microneedles. (d): Hollow microneedles. (a’)-(d’): Sustained gene-drug release after microneedles application. (a’): Solid microneedles. (b’): Coated microneedles. (c’): Soluble microneedles. (d’): Hollow microneedles. (B) Skin structure diagram and transdermal treatment of microneedle.
Solid microneedles:
In order to create drug diffusion microchannels on the skin, sharp geometric microneedles are designed to pierce the stratum corneum. Usually, the drug is applied to a flexible surface underneath the development of the microneedle. In order for systemic treatment to occur, the microneedles in the skin patch penetrate the skin and the medications are taken up by the capillaries [30]. For TDD solid microneedles can be used with or without a drug coating. For the subsequent topical administration, non-drug coated solid microneedles can improve drug penetration efficiency and form temporary skin microchannels [31]. Solid MNs have been made from a variety of materials, including silicone, metals (such as titanium and stainless steel), polymers, and ceramics. For example, Narayanan and Raghavan used a wet etching process to create sharp silicon MNs that had a mechanical strength 52 times greater than skin for seamless insertion. The needles' average height, base width, and tip diameter were 0.4, 110.5, and 158 lm, respectively [32] [Fig.7(a)]. These MNs have the ability to transport medication or vaccine formulations via passive diffusion, which is subsequently absorbed into the capillaries to produce systemic effects [33].
Coated Microneedles:
The drug solution or drug dispersion layer envelops the microneedles. The medication is rapidly administered after it dissolves from the layer. The coating layer's thickness and the needle's size, which is typically very small, determine how much medication can be loaded [34][Figure7(b)]. Lidocaine was loaded onto poly L-lactide (PLLA) microneedle arrays by Baek et al. In phosphate buffer saline, the loaded lidocaine released quickly and remained stable for three weeks. When placed and in contact with interstitial fluids, microneedles are assisted in disengaging from the skin by the use of a hydrophobic covering material. The use of coated microneedles to deliver several medications using a single formulation is being investigated. One study found that coating microneedles with different formulations and agents enables the co-administration of several drugs with different characteristics. The hydrophobicity of the peptide, the shape of the needle, and the excipients can all impact how well coated MNs deliver the peptides. These needles were also employed for the administration of local anesthetics. Following MN insertion, this PBAE and ICMV coating quickly moved from the MNs to the skin, facilitating the effective delivery of antigens to antigen-presenting cells and triggering a strong immune response. Despite being extremely simple, this approach still has a limit on the quantity of nanoparticles that coated MNs can be delivered to the skin [35].
Soluble microneedles:
The combination of drug nanocrystals or drug-loaded nanoparticles with dissolvable MNs has been prompted by the dire situation of poorly soluble drugs in topical application. Dissolvable MNs can deliver more nanoparticles than coated MNs because, in contrast to coated MNs, they can dissolve the entire MN and then release the encapsulated nanocrystals or nanoparticles at the administration site beneath the skin. The biodegradable and biocompatible materials that make up dissolving MNs have a tendency to break down and dissolve in bodily fluids, releasing loaded cargo at the target site. They are typically made by dissolving gelatin/carboxymethyl cellulose polymeric MN patches using the micro molding technique [36] [Figure 7(c)]. Dissolving microneedles, as opposed to coated ones, completely dissolve in the skin and leave no biohazardous waste behind after use. Typically, the microneedles are composed of water-soluble, safe, and inert substances like sugars and polymers that dissolve in the skin after Drugs are usually enclosed within the microneedle for skin delivery, even though dissolving microneedles can improve skin permeability as a pretreatment [37].
Hollow Microneedles:
In contrast to the first two, hollow needles have a hole at the tip that permits the release of the drug and a hollow core. Despite the differences between the two delivery methods, because the drug release action in MNs is comparatively similar to that of hypodermic needles, pre-existing vaccine formulation can be directly added to MNs in a smaller quantity without the need for additional processing. Large doses of medication or compounds with high molecular weights can be administered using these needles [38][Figure 7(d)]. Because pressure can be applied throughout the length of the MN during administration, it has also been demonstrated that they permit an increase in drug infusion rate. have demonstrated the in-situ construction of polymeric MNs for DD that are hollow and filled with liquid. Drugs can now be administered continuously thanks to the fabrication of hollow metal MN arrays. UV lasers have been employed in micromachining techniques to create machine molds from polyethylene terephthalate. Solid MNs are thought to be more robust than hollow MNs, which are still thought to be mechanically weaker and require more intricate manufacturing procedures [39].
Evaluation Parameters of LNP-Microneedle:
1. Physicochemical Characterization of LNPs
2. Mechanical and Structural Integrity of MNs
3. Stability of the LNP?MN System
4. In Vitro and Ex Vivo Release & Permeation Studies
5. In Vivo Pharmacokinetics & Efficacy
Advantages of Combining Lipid Nanoparticles with Microneedles:
1. Enhanced Skin Penetration & Bioavailability
2. Controlled, Sustained Drug Release
3. Improved Stability and Reduced Toxicity
4. Targeted and Flexible Delivery
5. Versatile Applications
Recent Evidence and Developments in LNP-Loaded Microneedles:
1. Dissolvable Bubble Microneedle Patches (bMNP) for Room-Temperature mRNA-LNP Delivery
A 2025 study introduced a dissolvable bubble microneedle patch (bMNP) that successfully incorporated mRNA-LNPs within a PVA + trehalose matrix. This design preserved LNP stability, enabling at least one-month storage at room temperature, and effectively induced spike-specific IgG, neutralizing antibodies, and Th1-polarized T-cell responses after transdermal SARS-CoV-2 antigen delivery [49].
2. Ionic Lipid Composition Optimizes LNP Stability During Microneedle Fabrication
A 2024 AIChE conference study explored how LNP composition affects stability when processed into microneedle patches via drying and casting. Using a Moderna-like formulation (SM-102, cholesterol, DMG-PEG2000, DSPC), researchers found:
These findings point toward formulation tuning as a key strategy for maintaining LNP integrity in MN platforms [50].
3. Thermostable Printed Micro-Needle Vaccine Patches
Another landmark publication demonstrated a microneedle “vaccine printer” that printed mRNA-LNP-laden microneedles capable of maintaining thermostability (≥6 months at room temperature). The printed patches preserved LNP integrity (particle size, encapsulation, morphology) and delivered consistently effective doses per needle, validated by in vitro assays [51].
4. LNP-Loaded Microneedles in Preclinical Vaccination Studies
A broader review (2023) of microneedle-based vaccine platforms highlighted the growing use of advanced systems—including PLGA nanoparticles embedded in dissolving MNs—for enhanced immunogenicity. While not always lipid-based, these systems underscore the increasing trend toward nanoparticle-MN convergence. Notable outcomes included six-month retention of mRNA activity at room temperature and sustained immune responses after single-patch delivery [52].
Future prospects of LNP-loaded microneedles for drug delivery:
1. Thermostable, cold-chain-independent vaccines and biologics
Prospect: LNP-loaded MN patches (printed, lyophilized or powder-attached) can convert cold-chain-dependent mRNA vaccines and other biologics into thermostable patch formats suitable for low-resource settings and mass campaigns. Recent studies demonstrated printed MN patches that preserved mRNA-LNP activity for months at room temperature and powder/lyophilized formats that markedly improve storage stability. This opens realistic pathways for decentralized distribution and easier stockpiling [53].
2. Decentralized/on-demand manufacture and personalized dosing
Prospect: Automated “microneedle vaccine printers” and modular printing technologies enable local, on-demand manufacturing of LNP-MN patches — supporting rapid response to outbreaks and personalized dose manufacture (age/weight/antigen). Coupled with thermostable LNP formulations, decentralized production could reduce reliance on large centralized cold-chain facilities [54].
3.Powder-attachment and lyophilization as scalable stabilization strategies
Dry LNP formats (powder-attached coatings or lyophilized LNPs reconstituted into MN matrices) are emerging as practical ways to preserve particle integrity during MN fabrication and storage. These approaches both reduce aqueous stress during casting and simplify handling, making industrial scale-up and QC easier. Continuous freeze-drying and optimized cryo/lyoprotectants are promising process innovations [55].
4. Expansion beyond vaccines -topical gene therapy, local oncology, and chronic dermal indications.
Dermal delivery via LNP-MN enables access to APC-rich skin (vaccination/immune modulation), local delivery of gene-editing cargos (CRISPR/siRNA) for dermatological diseases, and focal administration of chemotherapeutics/ immunomodulators for cutaneous tumors. Early preclinical studies and reviews highlight strong potential across these therapeutic areas, provided formulation and dosing challenges are solved [56].
5. Improved safety, efficacy and dose-sparing through dermal targeting
MN-mediated intradermal deposition of LNPs concentrates payloads in immune-active skin compartments, often eliciting stronger immune responses per microgram and enabling dose-sparing. This could lower costs and adverse systemic events for vaccines and immunotherapies. Continued mechanistic studies will refine particle size/surface design to optimize retention vs lymphatic drainage [57].
6. Regulatory and translational pathway-combination product challenges & opportunities
LNP-MN products are combination device-biologic entities requiring integrated CMC, device biocompatibility (ISO-10993), dose-per-needle control, sterility, and stability data. Recent reviews of nanoparticle therapeutics and MN regulatory guidance stress the need for robust comparability, stability-indicating assays for nucleic acids, and early dialogue with regulators to streamline pathways. These steps will determine the speed of clinical translation [58].
7. Key technical and knowledge gaps to address (near-term research priorities)
8. Longer-term outlook (5–10 years)
If the technical gaps above are closed, we can expect: (a) first approvals in niche vaccine or dermatology indications where local delivery offers clear advantages; (b) wider adoption for outbreak response via decentralized printing + thermostable LNPs; and (c) an expanding pipeline of topical gene therapies and combination immuno-oncology patch treatments. Regulatory frameworks likely will evolve to accommodate combination LNP-MN platforms as precedents emerge [60].
CONCLUSION
Lipid nanoparticle (LNP)–integrated microneedle (MN) patch systems represent a promising advancement in transdermal drug delivery by combining the advantages of nanocarrier-based encapsulation with minimally invasive skin penetration. This synergistic approach enhances drug stability, bioavailability, and patient compliance, particularly for vaccines, biologics, and gene-based therapeutics. Recent studies demonstrate successful formulation and delivery of LNPs using dissolving, hydrogel-forming, and coated microneedle platforms, highlighting their versatility and therapeutic potential.
However, challenges related to microneedle mechanical strength, nanoparticle stability, dose uniformity, large-scale manufacturing, and regulatory standardization remain to be fully addressed. Future research should focus on optimizing materials and fabrication techniques to ensure robust performance and reproducibility. Advances in scalable manufacturing technologies and standardized evaluation protocols will be critical for clinical translation. Overall, with continued progress in formulation design and regulatory alignment, LNP-loaded microneedle patches have strong potential to emerge as a clinically viable and patient-friendly drug delivery platform.
CONFLICT OF INTEREST: The author declares no potential conflict interest concerning the contents, authorships, and/or publication of this article.
SOURCE OF SUPPORT: Nil
FUNDING: The author Declare that this study has received no financial support.
ACKNOWLEDGEMENT:
The authors would like to thank Minerva College of Pharmacy, Indora, H.P for providing academic support and access to library and online resources required for this review study.
CONSENT & ETHICAL APPROVAL: Not applicable.
REFERENCES


Aatish Attri, Ritika Gupta, Kapil Kumar Verma, Lipid Nanoparticles in Microneedle Patch Delivery System: A Recent Insight and Prospects, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 306-322. https://doi.org/10.5281/zenodo.18140054
 10.5281/zenodo.18140054
10.5281/zenodo.18140054
