Department of Pharmaceutics, MVP Samaj’s college of pharmacy Nashik.
Clotrimazole is a widely used azole antifungal for vulvovaginal candidiasis; however, its poor aqueous solubility can limit dissolution and delay local availability. This study explores mechanochemical co-crystallisation as a solid-state strategy to enhance solubility and dissolution performance and translate the optimised co-crystal into a vaginal tablet dosage form. GRAS-listed co-formers (tartaric acid, cinnamic acid, ascorbic acid, maleic acid, m-toluic acid, and thiourea) were screened via liquid-assisted grinding (LAG). Prepared co-crystals were evaluated for melting point and saturated solubility. The best-performing system (clotrimazole–ascorbic acid) was optimised for stoichiometric ratio and characterised by FTIR, DSC, and PXRD to confirm a distinct solid phase. The optimised 1:2 co-crystal demonstrated a marked increase in saturated solubility over pure clotrimazole and improved dissolution in simulated vaginal fluid (SVF) of pH 4.5 compared with pure drug and marketed preparation. Vaginal tablets prepared by direct compression showed acceptable physical quality (thickness, hardness, friability) and enhanced drug release
Vulvovaginal candidiasis (VVC) is a common infection associated with discomfort and reduced quality of life. Local therapy via vaginal dosage forms is preferred because drug is delivered directly to the site of infection, systemic exposure is reduced, and effective local concentrations can be achieved. Among available dosage forms, vaginal tablets are convenient, stable, easy to handle, and can be manufactured by scalable processes such as direct compression—making them suitable for routine therapy as well as large-scale supply. [2,3]
Clotrimazole is a widely used azole antifungal, but its performance is limited by poor aqueous solubility. According to the Biopharmaceutic Classification System, clotrimazole is commonly discussed as a class II drug (high permeability, low solubility), making dissolution a key step for local availability. [9] When solubility is low, dissolution can be slow, which may delay therapeutic levels at the vaginal mucosa. Conventional solubility enhancement methods exist, but they can add formulation complexity or introduce stability challenges. A solid-state approach that improves solubility without changing the drug’s chemical identity is therefore valuable for developing robust vaginal tablets.
Pharmaceutical co-crystallisation is one such approach. Regulatory guidance describes co-crystals as crystalline materials composed of two or more different molecules (typically an API and a co-former) in the same crystal lattice. [4] Co-crystals can modify melting behaviour, solubility, dissolution rate, and processing attributes while keeping the API chemically intact. [5–7] In this work, multiple GRAS co-formers were screened to prepare co-crystals of Clotrimazole; the optimised system was characterised using solid-state techniques (FTIR/DSC/PXRD); and the selected co-crystal was formulated into vaginal tablets and evaluated for tablet quality and dissolution performance in simulated vaginal fluid (pH 4.5).
MATERIALS AND METHODS
Materials
Clotrimazole was used as the active pharmaceutical ingredient (API). The following co-formers were screened for co-crystal formation: tartaric acid, cinnamic acid, ascorbic acid, maleic acid, m?toluic acid, and thiourea. Simulated vaginal fluid (SVF) of pH 4.5 was used as dissolution medium for in?vitro release testing; the SVF concept is based on established vaginal fluid simulant literature. [8]
Co-crystal preparation by liquid-assisted grinding (LAG)
Drug and co-former were weighed in the desired molar ratio and triturated using mortar and pestle. A minimal quantity of volatile solvent (few drops) was added to promote co-crystallisation under mechanochemical conditions. Initial screening was carried out at 1:1 molar ratio. Promising systems were further evaluated at 1:2 and 1:3 ratios. [6,7]
Evaluation of co-crystals
Prepared co-crystals were evaluated for melting point, saturated solubility (UV quantification), and morphology (microscopy). The optimised co-crystal was further characterised by FTIR, DSC, and PXRD to support formation of a distinct solid phase. [6]
Vaginal tablet formulation (direct compression)
The selected co-crystal was formulated into vaginal tablets by direct compression. Powder blend was mixed, lubricated, and compressed using rotary tablet compression with B?tooling.
Table 1. Composition of vaginal tablet (per tablet)
|
Ingredient |
Quantity (mg) |
|
Clotrimazole |
200 |
|
Lactose monohydrate |
379.5 |
|
Maize starch |
379.5 |
|
Methyl paraben |
0.8 |
|
Propyl paraben |
0.2 |
|
Sodium starch glycolate |
10 |
|
Talc |
10 |
|
Magnesium stearate |
10 |
|
Colloidal silicon dioxide |
10 |
Dissolution study
Dissolution testing was performed in SVF (pH 4.5) using USP type II (paddle) apparatus. Medium volume: 100 mL; paddle speed: 50 rpm; temperature: 39 ± 0.5 °C (bath) and 37 ± 0.5 °C (bowl). Samples were withdrawn at 5, 10, 15, 20, 30, 45, 60, and 75 minutes and analysed at 263 nm.
RESULTS AND DISCUSSION
Co-crystal screening: melting point shift
Co-crystals prepared at 1:1 ratio exhibited melting points distinct from the pure drug and co-formers (Table 2), suggesting alteration of the solid-state arrangement and potential new phase generation.
Table 2. Melting points of screened co-crystals (1:1, LAG)
|
System |
Pure component MP (°C) |
Co-crystal MP (°C) |
|
Clotrimazole (API) |
147–149 |
— |
|
CLT–Tartaric acid |
TA: 170–175 |
60–70 |
|
CLT–Cinnamic acid |
CA: 127–130 |
48–58 |
|
CLT–Ascorbic acid |
AA: 187–190 |
95–100 |
|
CLT–Maleic acid |
MA: 135–140 |
105–115 |
|
CLT–m?Toluic acid |
m?TA: 105–107 |
62–68 |
|
CLT–Thiourea |
TU: 175–180 |
110–120 |
Saturated solubility screening and co-former selection
Saturated solubility screening at 1:1 ratio (Table 3) identified clotrimazole–ascorbic acid (CLT–AA) as the best-performing system, followed by CLT–cinnamic acid. Figure 1 visualises the comparative solubility across screened co-formers.
Table 3. Saturated solubility screening (1:1, LAG)
|
System |
Solubility (mg/mL) |
Fold enhancement |
|
Pure clotrimazole |
0.0009 |
— |
|
CLT–Tartaric acid |
0.0071 |
7.88 |
|
CLT–Cinnamic acid |
0.0106 |
11.77 |
|
CLT–Ascorbic acid |
0.0166 |
18.44 |
|
CLT–Maleic acid |
0.0076 |
8.44 |
|
CLT–m?Toluic acid |
0.0099 |
11.00 |
|
CLT–Thiourea |
0.0075 |
8.33 |
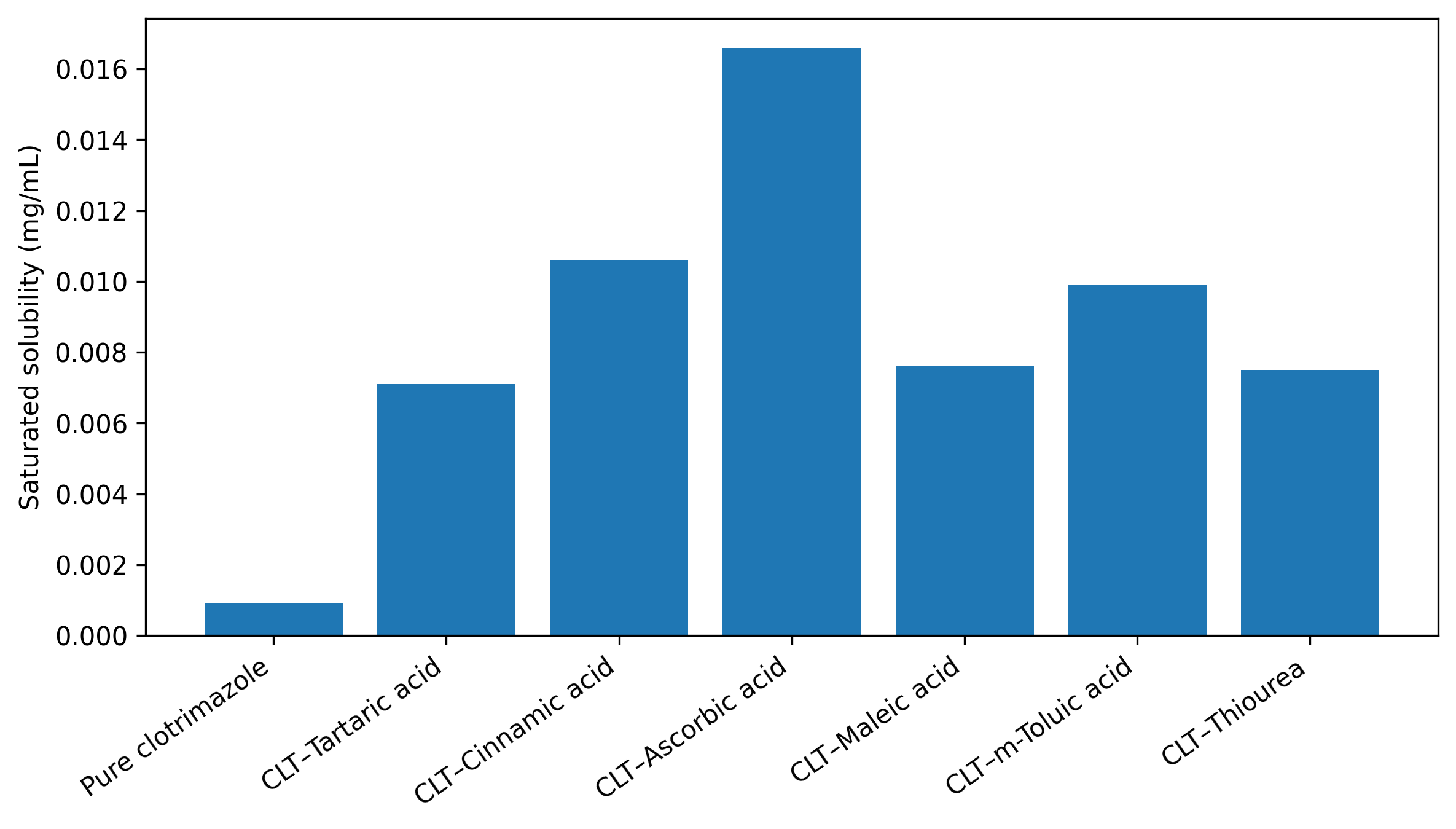
Figure 1. Saturated solubility screening of clotrimazole co-crystals (1:1, LAG).
Stoichiometric optimisation
Promising co-crystals (CLT–AA and CLT–cinnamic acid) were evaluated across multiple drug:co-former ratios. The CLT–AA 1:2 system provided the highest solubility among tested ratios (Table 4), supporting selection of 1:2 as the optimised ratio. Figure 2 summarises the effect of stoichiometry on saturated solubility.
Table 4. Effect of stoichiometric ratio on saturated solubility
|
Co-crystal |
1:1 (mg/mL) |
1:2 (mg/mL) |
1:3 (mg/mL) |
|
CLT–Ascorbic acid |
0.0166 |
0.0266 |
0.0201 |
|
CLT–Cinnamic acid |
0.0106 |
0.0187 |
0.0152 |
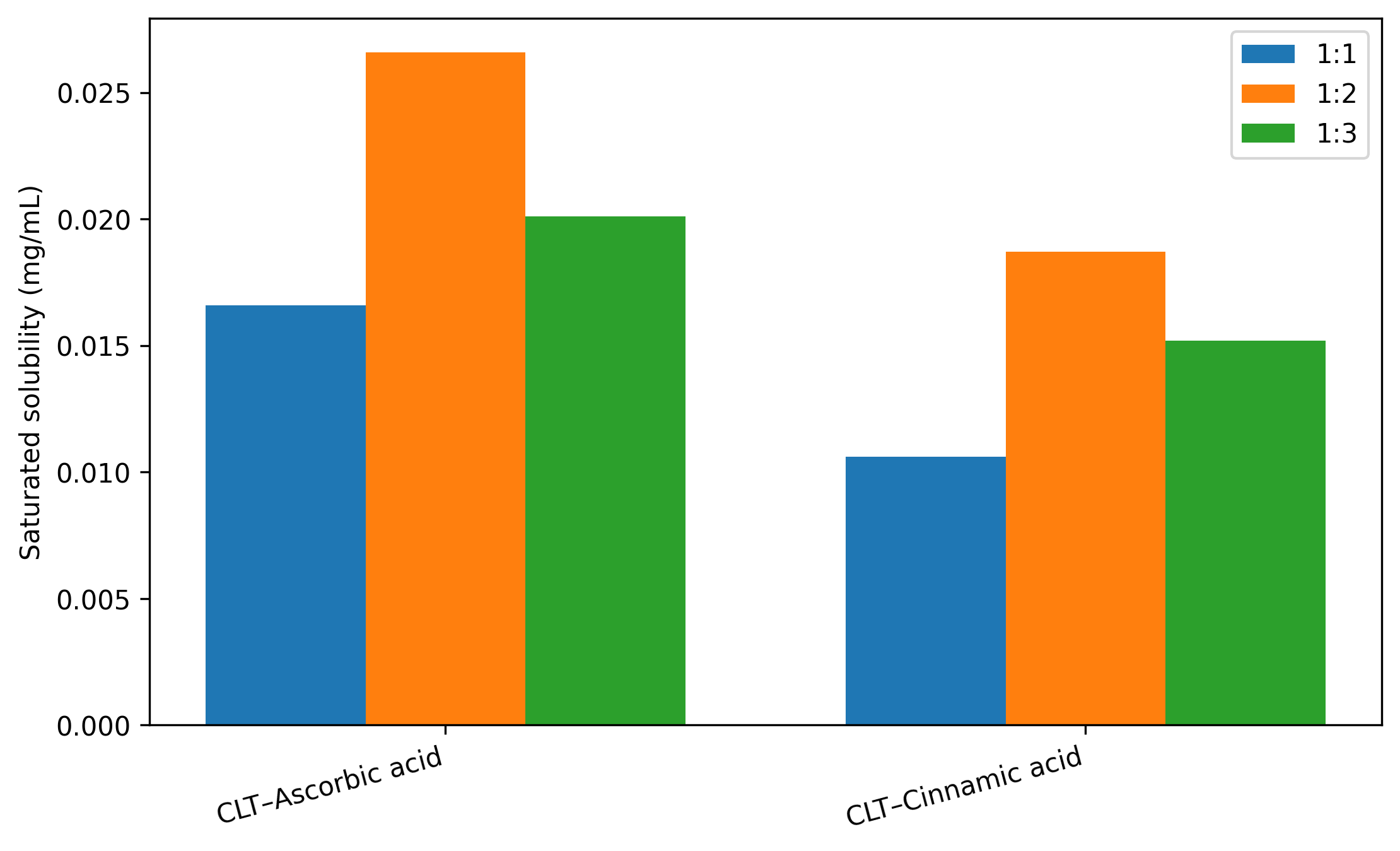
Figure 2. Effect of drug:co-former ratio on co-crystal solubility.
Solid-state characterisation of the optimised co-crystal
The optimised CLT–AA (1:2) co-crystal was characterised using FTIR, DSC, and PXRD. Shifts/changes in characteristic FTIR bands, distinct thermal transition(s) in DSC, and emergence of new PXRD peaks along with disappearance/attenuation of parent peaks support formation of a distinct crystalline phase. [6]
Micromeritics and assay
Micromeritic parameters (Table 5) and drug content (Table 6) were evaluated to support processability and confirm drug loading.
Table 5. Micromeritics properties
|
Property |
Clotrimazole |
Co-crystal (CLT–AA) |
|
Bulk density |
0.629 ± 0.0193 |
0.502 ± 0.0161 |
|
Tapped density |
0.728 ± 0.0190 |
0.823 ± 0.0193 |
|
Angle of repose (°) |
40.13 ± 0.816 |
52.18 ± 0.736 |
|
Carr’s Index |
23.60 ± 1.360 |
30.98 ± 1.204 |
|
Hausner’s Ratio |
1.44 ± 0.0254 |
1.30 ± 0.0233
|
Table 6. Drug content (assay)
|
Sample |
Equivalent amount analysed |
% Drug content |
|
Pure clotrimazole |
10 mg |
100 |
|
CLT–AA (1:2) co-crystal |
4.8 mg |
98 |
Tablet evaluation
Vaginal tablets containing the optimised co-crystal were evaluated for key physical parameters (Table 7). All measurements were within acceptable limits for a directly compressed vaginal tablet.
Table 7. Physical evaluation of vaginal tablets
|
Parameter |
Result |
|
Average weight |
1000 ± 3 mg |
|
Thickness |
5.78 ± 0.04 mm |
|
Hardness |
5.1 ± 0.1 kg/cm² |
|
Friability |
0.02% |
In?vitro dissolution in SVF (pH 4.5)
Dissolution testing in simulated vaginal fluid (SVF, pH 4.5) demonstrated that the CLT–AA (1:2) co-crystal achieved substantially higher cumulative release than pure clotrimazole and also exceeded marketed preparation at most time points (Table 8, Figure 3). [8]
Table 8. % cumulative drug release (%CDR) in SVF (pH 4.5)
|
Time (min) |
Pure CLT |
CLT–AA co-crystal (1:2) |
Marketed preparation |
|
5 |
21.66 ± 1.4 |
37.33 ± 1.69 |
30.38 ± 1.55 |
|
10 |
31.06 ± 0.82 |
49.66 ± 1.24 |
38.62 ± 1.22 |
|
15 |
38.16 ± 0.62 |
63.66 ± 1.35 |
51.32 ± 1.34 |
|
20 |
44.53 ± 0.41 |
68.12 ± 0.81 |
59.32 ± 0.77 |
|
30 |
51.16 ± 0.84 |
72.21 ± 1.63 |
65.71 ± 1.09 |
|
45 |
54.3 ± 0.81 |
81.5 ± 1.08 |
74.5 ± 1.59 |
|
60 |
56.33 ± 1.24 |
92.23 ± 1.11 |
80.23 ± 1.38 |
|
75 |
62.12 ± 1.64 |
96.28 ± 0.72 |
87.32 ± 0.66 |
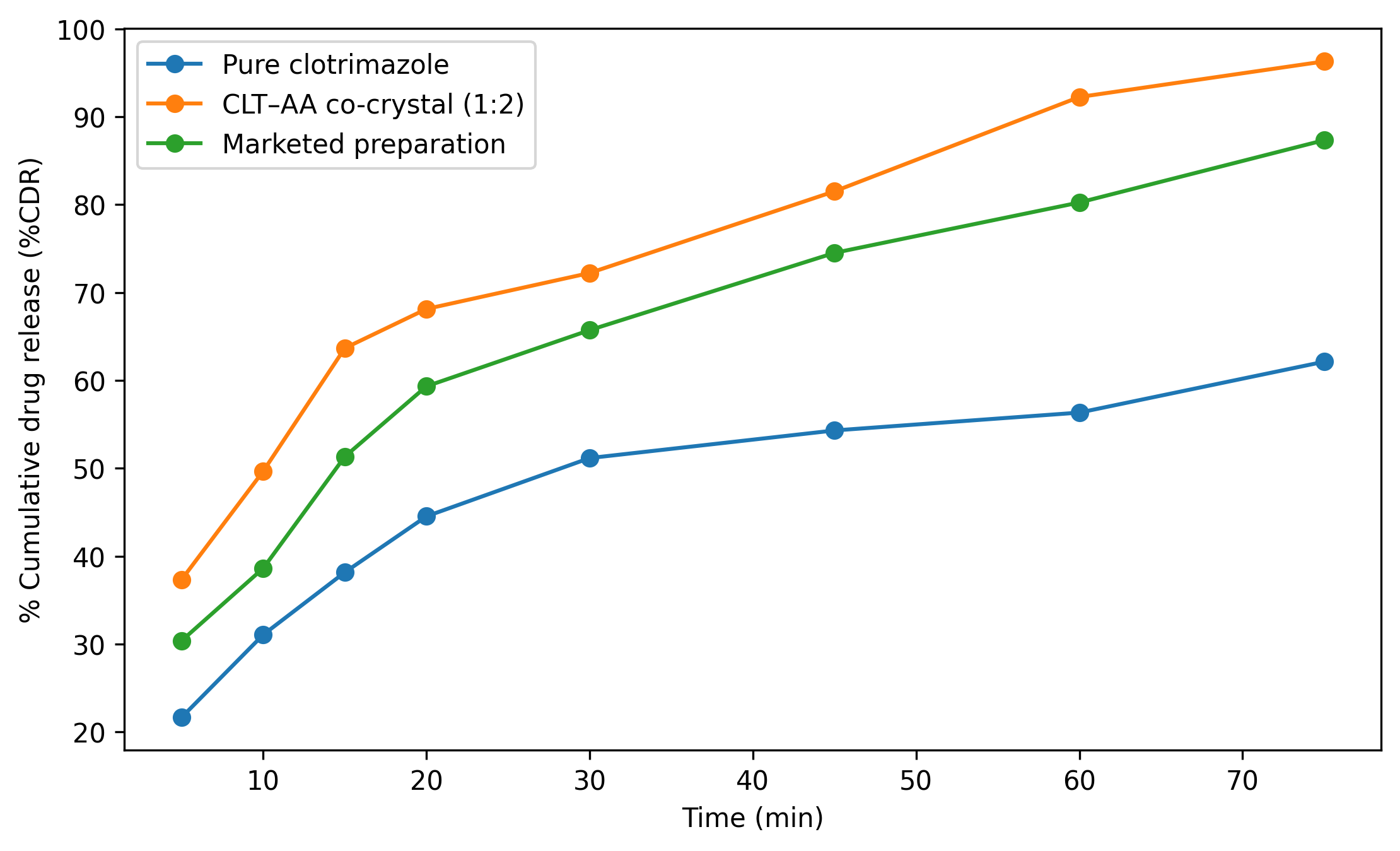
Figure 3. Dissolution profile in simulated vaginal fluid (SVF) of pH 4.
CONCLUSION
Mechanochemical co-crystallisation using GRAS co-formers successfully generated clotrimazole co-crystals with altered solid-state properties and improved aqueous performance. Among screened systems, clotrimazole–ascorbic acid (CLT–AA) showed the highest solubility enhancement at screening stage and the 1:2 ratio delivered the best solubility among tested stoichiometries. The optimised co-crystal exhibited improved dissolution in SVF (pH 4.5) compared with pure clotrimazole and marketed preparation. Vaginal tablets prepared by direct compression met physical quality requirements and preserved the dissolution advantage. Co-crystallisation is therefore a viable solid-state strategy to enhance in?vitro performance of clotrimazole vaginal tablets. [5–7]
SUMMARY
Six GRAS co-formers were screened via liquid-assisted grinding (LAG) for co-crystal formation with clotrimazole.
CLT–Ascorbic acid demonstrated the highest saturated solubility at 1:1 screening.
Stoichiometric optimisation identified CLT–AA (1:2) as the best-performing ratio in terms of solubility.
Solid-state analysis (FTIR/DSC/PXRD) supported formation of a distinct crystalline phase. [6]
Co-crystal vaginal tablets showed faster dissolution in SVF (pH 4.5) than pure drug and marketed preparation. [8]
Finished tablets met key physical quality parameters (weight variation, thickness, hardness, friability).
REFERENCES

A. Savkare, S. Karwa, M. Jadhav, A. Ushir, R. Jadhav, A. Bachhav, Mechanochemical Co-crystallization of Clotrimazole and Development of an Optimized Vaginal Tablet, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 4, 413-418 https://doi.org/10.5281/zenodo.19396623
 10.5281/zenodo.19396623
10.5281/zenodo.19396623
