Krishna School of Pharmacy and Research, Drs Kiran and Pallavi Patel Global University, Vadodara, 391240
Clinically diverse, psoriasis is a chronic skin condition that can manifest as plaque, flexural, guttate, psoriatic arthritis, nail psoriasis, pustular, or erythrodermic. Psoriasis is thought to impact 60 million individuals globally, and in the UK, it affects 1.52% of the general population. Psoriasis is an inflammatory disease that is mediated by the immune system and has a significant hereditary component. A comprehensive and multidisciplinary approach to therapy is necessary due to its correlation with psoriatic arthritis and elevated incidence of cardiometabolic, hepatic, and psychiatric comorbidities. Topical treatments for psoriasis include corticosteroids and vitamin D analogs; phototherapy (such as psoralen and ultraviolet A radiation (PUVA) and narrowband ultraviolet B radiation (NB-UVB); standard systemic treatments (such as methotrexate, ciclosporin, and acitretin); biologic treatments (such as tumor necrosis factor (TNF), interleukin (IL)-17, and IL-23 inhibitors); and small molecule inhibitors (such as dimethyl fumarate and apremilast).Advance in the understanding of its pathophysiology have led to development of highly effective and targeted treatment.
Psoriasis is an inflammatory, immune-mediated, autoimmune disease that affects the joints and skin. The name “psoriasis” comes from the Greek words "psora," which means “itch,” and “iasis,” which means “condition.” Between 2% and 3% of people worldwide have psoriasis, with lower prevalences found in some parts of Asia and Africa and greater prevalences seen in Scandinavian communities [1–3]. Psoriasis affects both males and females, with earlier onset in females and those with a family history. Its age of onset shows a bimodal distribution with peaks at 30–39 years and 60–69 years in men, and 10 years earlier in women [4]. An estimated 60 million people have psoriasis worldwide and with country specific prevalence varying between 0.44% to 2.8% of the adult population in India. Generally inherited, psoriasis is characterized by a development of erythematous, well-defined, scaly plaques that are usually symmetrical. The scalp, fingers, toes, palms, soles, umbilicus, gluteal region, under the breasts, genital area, elbows, knees and sacrum are among the often-impacted locations. Plaque psoriasis is the most common subtype of psoriasis, affecting the scalp, trunk, and extremities. It is also believed that there is also a link between Psoriasis and the HIV virus and Psoriasis is linked to dandruff and unfortunately to some forms of arthritis. Symptoms which can appear like rashes occurring in patches and look different as we see them in individual. Some may appear as major eruptions all over the body or dandruff-like scaling. It could also be rashes with variation in the colours like shades of brown or pink or black skin or grey with purple or even with red along with silver scaling on the white skin, or cracked skin due to dryness that might bleed, or scaling small spots usually occurring in children, burning sensation, soreness, the appearance of episodic rashes that would aggravate for some weeks or months and then eventually subside[5]. Family doctors are best suited to identify and start addressing psoriasis at the primary care level, where many patients initially seek evaluation and treatment. By incorporating the most recent research, this review seeks to present a thorough and up-to-date summary of psoriasis diagnostic and treatment approaches.
PATHOPHYSIOLOGY
This chronic inflammatory disease's precise pathogenesis is still mostly unknown. Nevertheless, it has been noted that when dendritic cells, also known as Antigen Presenting Cells (APCs), come into contact with an antigen, they are able to recognize the stress signals that keratinocytes emit. Naïve T cells become activated as a result of this contact, and they then release a variety of cytokines that encourage their development into effector T cell subsets like Th1, Th2, and Th17. Specific cytokines, including as interleukin (IL-2), tumour necrosis factor (TNF-α), and interferon (IFN-α), are then produced by each of these effector cells [6]. Different cytokine signals control the differentiation of naïve T cells into Th1 and Th17 subsets; IL-12 promotes Th1 lineage commitment, whereas IL-23 aids in the formation of Th17 cells. TNF-α, IFN-γ, and IL-2 are the main substances secreted by Th1 cells. These substances then improve antigen-presenting cell (APC) activation, which triggers the release of more stimulatory signals and increases T-cell recruitment [7,8,9].
On the other hand, Th17 cells generate IL-17, a crucial cytokine in the immunopathogenesis of psoriasis, and IL-23 helps Th17 cells continue to release IL-17A, IL-17F, and IL-22. [10,11]. In addition to inducing the synthesis of several cytokines and adhesion molecules, TNF-α activates its receptor on keratinocytes, causing hyperproliferation that aids in the creation of lesions and sustaining the inflammatory cascade.[12] By encouraging development into Th17 T cells, which subsequently release IL-17 and IL-22, IL-23 plays a critical role in the pathophysiology of psoriasis, according to recent results from inflammatory skin models. In psoriasis, aberrant maturation and altered epidermal differentiation are caused by these cytokines, which are known that appear after scale is to be key inducers of epidermal hyperplasia. [13] Increased vascular endothelial growth factor (VEGF) levels in psoriatic plaques promote angiogenesis and cause Auspitz's sign, or bleeding spots that appear after scale is removed. Furthermore, it has been determined that IL-8 plays a significant role in the recruitment and build-up of neutrophils in psoriasis skin [14].
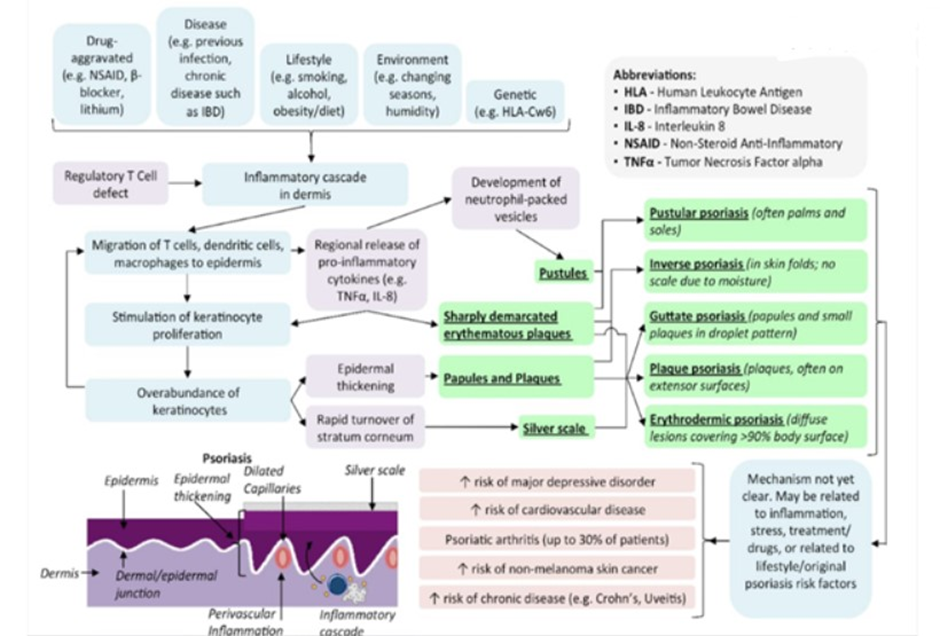
Figure 1- PATHOPHYSIOLOGY OF PSORIASIS
CLINICAL FEATURE AND DIAGNOSIS
Psoriasis is of different types in which Plaque is one of the types of psoriasis. It is the most prevalent type of psoriasis and results in elevated skin patches, covering scales, itching, and dryness. The other type is nail psoriasis, which results in irregularly shaped fingernails and toenails that are discoloured and pitted. This condition, also known as onycholysis, may cause the nails to loosen up and split from the nail bed; if it worsens, the nails may potential disintegrate. Pustular psoriasis is an uncommon kind that is characterised by blisters filled with pus. It may show up in the tiny space. The sole and palm or in widespread patches. Fever and malaise generally are accompanied by a systemic type of inflammatory, chronic disease, which is the Generalised pustular type of psoriasis. Table 1 gives types of psoriasis.
Table 1: Types of psoriasis and their characteristics
|
TYPES OF PSORIASIS |
CHARACTERISTICS |
|
Plaque psoriasis |
Itchy, dry, covered with scales |
|
Nail psoriasis |
Abnormally grown nails and discolouration |
|
Guttate psoriasis |
Scaling spot all over the trunk, arm |
|
Inverse psoriasis |
Inflamed skin in smooth patchwork |
|
Erythrodermic psoriasis |
Peeling form of rash |
|
Pustular psoriasis |
Blisters with pus |
|
Psoriatic arthritis |
Arthritis associated |

Figure 2 - PSORIASIS ON THE DIFFERENT PARTS OF BODY
Diagnosis
A skin biopsy is rarely necessary because the diagnosis is mainly clinical. Appropriate treatment can be started based on how severe the illness is. Topical treatments such as corticosteroids, vitamin D3 analogues, and combination products are the first line of treatment for mild to moderate illness. Primary care doctors can safely commence and prescribe these topical therapies because they are effective. Patients may need systemic medication and additional dermatologist assessment if their symptoms are more severe and refractory.
CURRENT TREATMENT OPTIONS
The treatment of the psoriasis contains the topical treatment, systemic therapy, biological therapy and phototherapy. Table 2 shows the current treatment options:
Table 2 : THERAPIES AND THE DRUGS
|
Treatment |
|
|
Topical Therapy |
|
|
First Line Therapy |
-Apremilast -Cyclosporine -Methotrexate
-Etanrecept -Infliximab -Secukinumab -Ustekinumab |
|
First Line Therapy |
|
|
Second Line Therapy |
|
TOPICAL TREATMENT
For patients whose disease affects less than 10% of their body surface area (BSA), topical or local therapy is considered the preferred treatment for restricted cutaneous psoriasis. [15] It is also recommended for individuals with immunocompromised conditions, psoriasis in youngsters, psoriasis in the scalp, palmoplantar psoriasis, nail psoriasis, and situations involving sensitive areas like the face, flexures, and genitalia. Additionally, individuals taking systemic therapy who have moderate to severe psoriasis (>10% BSA involvement) may benefit from topical medicines as adjuvants. Emollients The mainstay of psoriasis treatment, emollients mostly serve as adjuvants to other topical or systemic drugs. Action mechanism: Emollients facilitate the penetration of other medications and encourage the loosening of adhering hyperkeratotic scales. They work by keeping the stratum corneum hydrated and stopping water loss via the epidermis. Additionally, they soothe pruritus, lessen scaling, hydrate dry skin, and speed up crack healing. [16] Efficacy: Emollients have not proven to be more effective than a placebo when used alone. [17] However, they are useful throughout the continuation phase, act as steroid-sparing agents, and enhance the effectiveness of topical corticosteroids (TCS) when administered as adjuvants with topical or systemic therapy. [18] However, there isn't enough data to say whether they can stop localized plaque psoriasis from reoccurring frequently.
SYSTEMIC THERAPY
Phototherapy For moderate to severe psoriasis, phototherapy is the main treatment option, especially when topical medications are ineffective. Broadband UVB, narrowband UVB (NB UVB), and psoralen with UVA are among the available modalities. NB-UVB is commonly used as first-line therapy because of its proven effectiveness and good safety profile in numerous randomized controlled trials. With no indication of an elevated risk of skin cancer, it can be given to almost any patient, including youngsters and expectant mothers [19].
Acitretin:
A synthetic retinoid called Acitretin is prescribed to treat moderate to severe psoriasis. Because it increases efficacy, permits dose reduction, and reduces the likelihood of side effects, its function as an adjuvant therapy in conjunction with other systemic medicines is well established. 26–28 Large-scale, reliable clinical trials evaluating its safety and effectiveness as a monotherapy are still scarce, nevertheless. Photosensitivity, gastrointestinal issues, arthralgia, and mucocutaneous dryness are typical side effects. Acitretin may also result in increased triglyceride levels and transaminitis. Due to the drug's strong teratogenic properties, pregnant women of reproductive age and potential should not take it for up to three years after stopping it[20].
Methotrexate:
Methotrexate a common treatment for moderately to severely severe psoriasis and psoriatic arthritis is methotrexate, an inhibitor of folate production with cytostatic and anti-inflammatory properties. Robust large-scale trials are still rare despite a wealth of clinical experience. Nearly 40% of patients on methotrexate experienced a 75% decrease in Psoriasis Area and Severity Index at 16 weeks, compared to 18.9% of placebo recipients in a randomized, double-blind, placebo-controlled study[21].
While nausea, vomiting, diarrhoea, and exhaustion are among the most frequent side effects, hepatotoxicity is the most well-known adverse effect [22]
Cyclosporine:
Cyclosporine a calcineurin inhibitor called cyclosporine is prescribed for moderate to severe psoriasis and is also effective in treating psoriatic arthritis. [23,24] Within 12 to 16 weeks, 80% to 90% of the 400 patients in a multicentre randomized study showed significant improvement or total remission. [25] Compared to other systemic medicines, it has a quicker onset of action and raises fewer concerns about myelosuppression or hepatotoxicity. However, there are a number of side effects linked to cyclosporine, including nephrotoxicity, hypertension, hypertriglyceridemia, gingival hyperplasia, tremors, hypomagnesemia, hyperkalaemia, several drug interactions, and an elevated risk of cancers like lymphoma and skin cancers[26].
BIOLOGICAL THERAPY
Definition: Biologic therapy refers to protein-based drugs derived from living organisms that act on specific points within the inflammation cascade, including monoclonal al antibodies against cell surface markers, cytokines, and adhesion molecules. [27]
Biologic Treatment For patients who do not respond well to traditional systemic medicines, cannot endure side effects, or are inappropriate because of concomitant diseases, biologic drugs have become extremely effective alternatives. Although a meta-analysis of pivotal phase III trials shows that infliximab is the most effective, followed by Ustekinumab, adalimumab, and etanercept, there is no clear sequence of initiation or switching. [28] Clinical features, safety profile, patient preference, and cost-effectiveness (about $20,000 to $25,000 per year) are taken into consideration while choosing a therapy. Retrospective research and randomized trials have demonstrated that biologics are not linked to a higher risk of serious infections or cancer. [29,30]
PHOTOTHERAPY
Since ancient times, phototherapy has been used to treat skin conditions. Currently, phototherapy is still one of the most popular ways to treat psoriasis, with the most popular methods being psoralen-ultraviolet A (PUVA) and narrowband UVB. [31] Clinical evidence repeatedly demonstrates that phototherapy is among the most effective therapeutic alternatives, particularly for patients with moderate to severe illness affecting broad body surface areas.
The therapeutic effects of phototherapy for psoriasis have been explained in the literature by four categories of action: (a) cytokine profile adjustment, (b) apoptosis induction, (c) immunosuppression enhancement, and (d) other additional mechanisms.
MANAGEMENT AND LIFESTYLE MODIFICATION
Everyone can benefit from healthy habits like exercising and not smoking. If you have psoriasis, healthy habits have some extra benefits. One can manage psoriasis by Quitting smoking: Researchers have found that smokers who have psoriasis and quit smoking can: Reduce their risk of developing diseases of the heart, blood vessels, liver, and gums. Lessen their chance of developing an autoimmune disease like Crohn’s disease. Have fewer psoriasis flares. Have less palmoplantar psoriasis. Increase remissions (periods with little or no psoriasis)
Limit alcohol: Researchers have also found several benefits to limiting alcohol if you have psoriasis. These include: Less psoriasis because treatment becomes more effective. Increased remissions, Reduced risk of developing psoriatic arthritis (for women) and fatty liver disease and Decreased risk of liver damage from psoriasis medications[32].
Maintain a healthy weight: If you are overweight, losing weight can: Reduce your psoriasis flares, Decrease the need for psoriasis medications, Improve how well your psoriasis treatment works, Decrease your risk of developing diseases associated with psoriasis, including heart disease, high blood pressure, unhealthy cholesterol levels, fatty liver disease, and diabetes.
Losing weight helps: After losing weight, many patients discover that their psoriasis medicine, which previously failed, begins to work and after losing weight, many patients discover that their psoriasis medicine, which previously failed, begins to work.
Eat a healthy, balanced diet: Eating a healthy and balanced diet has benefits for everyone. If you have psoriasis, the benefits include: Improve your health and help you feel better, Reduce your risk of developing diseases linked to psoriasis, including diabetes, heart disease, and high blood pressure.
Exercise: While exercise may seem impractical if you have psoriasis, working out can reduce some of psoriasis’s negative effects by helping you: Lose weight or maintain a healthy weight, Reduce your risk of developing diseases linked to psoriasis, including fatty liver disease and heart disease, Reduce stress, depression, and anxiety, Reduce exercise pain. If you have pain while exercising, tell your dermatologist. You may be able to make some changes that can help prevent the pain while working out[33].
Get screened for related diseases: Getting screened can help you: Find a disease early, when it can often be cured or managed successfully than Take steps to reduce the effects that the related disease has on your life and then Allow you to use a psoriasis treatment that may help reduce the effects of a related disease (for example, some biologics that treat psoriasis may also reduce the risk for a heart attack).
Check your eyes: If you have severe psoriasis, your dermatologist may recommend that you see an eye doctor once or twice a year. This can find eye problems early.
See a dermatologist and keep your appointments: Psoriasis tends to be a lifelong condition. Dermatologists understand this disease and know how to treat it appropriately. A dermatologist can help you: Find psoriasis treatment that’s right for you. Control psoriasis, which can prevent psoriasis from worsening and improve your quality of life. Assess your risk of developing related diseases and tell you when to get screenings for these diseases, Find early symptoms of psoriatic arthritis so that you can begin treatment. The impact that psoriasis has on your life can be significant. Making healthy lifestyle choices may reduce this impact.
Diseases more common in people who have psoriasis: If you have psoriasis, research shows that you may have a higher risk of developing the following: Addiction to alcohol or tobacco ,Crohn’s disease, Diabetes. High blood pressure, Eye problems, Gum disease, Heart and blood vessel diseases (heart attack, stroke), Kidney disease, Liver disease, Mood disorder (anxiety, depression, thoughts of suicide), Obesity, Psoriatic arthritis and Unhealthy cholesterol levels. The longer you have psoriasis, the greater your risk of developing related diseases. A healthy lifestyle, however, can reduce your risk.
EMERGING THERAPIES AND FUTURE DIRECTIONS
SNORA 73 AND PSORIASIS
A promising new approach for psoriasis treatment involves more precise, targeted disruption of snoRNA. This regulatory molecule plays a critical role in the disease progression of psoriasis. The snoRNAs are a class of non-coding RNAs that are most notably involved in the modification and maturation of ribosomal RNA. They guide chemical modifications of rRNA, such as methylation and pseudoridylation, both of which are essential in the proper formation and function of ribosomes [34]. However, more recent research has revealed broader functional implications of small nuclear RNAs (snRNAs) in gene regulation involving alternative splicing, mRNA stability, and chromatin remodelling, impacting cellular processes far beyond ribosomal biogenesis [35]. The snoRNAs' ability to modify gene regulation reflects their functional diversity and impact on cellular homeostasis and function. Disruption of snoRNA expression and function has been linked to various neurodevelopmental, cancerous, and autoimmune diseases, further highlighting their importance in maintaining cellular integrity and function [36]. Particularly in the context of psoriasis, modifications within snoRNA activity have the potential to amplify keratinocyte hyperproliferation and inflammatory responses, both of which are notable features of the disease [37].
IL21, an alternative inhibition target
Interleukin-21 has recently gained attention as a potential therapeutic target in psoriasis due to its role in promoting inflammatory immune responses, mainly through modulation of T helper cell subtypes, such as Th17 and Tregs. Current therapeutic approaches for psoriasis often target cytokines like IL-17 and IL-23 to alleviate inflammation. However, IL-21 presents an alternative route with specific promise due to its distinct effects on immune cell differentiation and cytokine expression [38]. Studies have identified IL-21 as a key factor in psoriasis pathology, with elevated levels associated with the severity of psoriasis, promoting an inflammatory environment by encouraging Th17 differentiation while inhibiting Treg cells, which typically act to moderate immune responses [39]. This Th17/Treg imbalance leads to exacerbated inflammatory responses, further driving the progression of psoriasis [40]. For instance, Shi et al. investigated IL-21 expression in moderate-to-severe plaque psoriasis patients. They found increased IL-21 and IL-21 receptor (IL-21R) expression in lesional skin and peripheral blood samples of psoriasis patients [41]. The study illustrated that IL-21 induced Th17 differentiation, enhanced expression of pro-inflammatory cytokines IL-17A and IL-22, and suppressed Treg cell differentiation by downregulating transcription factor Foxp3 expression.
The advent of IL-21 inhibitors provides a promising therapeutic approach. However, IL-21’s multifaceted role in immune regulation poses challenges for therapeutic targeting [42]. Interleukin-21 is involved in autoimmune inflammation and contributes to antiviral and antitumor immune responses. Thus, complete inhibition of IL-21 could carry risks of weakening the immune system’s ability to combat infections or tumours.
The therapeutic challenge is to achieve a balance in which IL-21 activity is sufficiently reduced to alleviate autoimmune pathology without significantly impairing immune defences [43]. One approach to achieving this balance might involve selective inhibition of IL-21 signalling pathways specific to Th17 cells while sparing pathways that support antiviral immunity .
CONCLUSION
Psoriasis is a chronic, immune-mediated inflammatory skin disease characterized by hyperproliferation of keratinocytes and systemic inflammation. It affects approximately 2–3% of the global population and is associated with significant physical, psychological, and socioeconomic burden. The pathogenesis involves a complex interplay between genetic predisposition, environmental triggers, and immune dysregulation—particularly involving the IL-23/Th17 axis.
Recent advances in biologic therapies, particularly IL-17 and IL-23 inhibitors, have revolutionized treatment and improved the quality of life for many patients. However, long-term safety, cost, and accessibility remain ongoing concerns. In addition, psoriasis is increasingly recognized as a systemic disease, often associated with comorbidities such as psoriatic arthritis, cardiovascular disease, metabolic syndrome, and depression.
FUTURE RESEARCH DIRECTIONS
Future research should focus on:
REFERENCES
https://www.doc2us.com/topic-1-understanding-psoriasis
https://medizzy.com/feed/40596461
https://share.google/images/a0wDUP2DWEjI0DIqA
https://upload.wikimedia.org/wikipedia/commons/b/b3/Psoriasis_on_back.jpg
https://www.healthcentral.com/condition/psoriatic-arthritis/psoriatic-arthritis-of-hands
https://www.doc2us.com/topic-1-understanding-psoriasis
https://medizzy.com/feed/40596461
https://share.google/images/a0wDUP2DWEjI0DIqA
https://upload.wikimedia.org/wikipedia/commons/b/b3/Psoriasis_on_back.jpg
https://www.healthcentral.com/condition/psoriatic-arthritis/psoriatic-arthritis-of-hands






Hiral Patel, Kesha Patel, Avni Patel, Dhruvi Patel, Devanshi Matroja, Priyal Patel, Psoriasis: Evolution of Treatment Modalities – Past, Present, and Future Perspectives, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 3731-3742. https://doi.org/10.5281/zenodo.18063424
 10.5281/zenodo.18063424
10.5281/zenodo.18063424
