
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
NRI College Of Pharmacy, Pothavarappadu, Eluru District, Andhra Pradesh, India
Daunorubicin, an anthracycline-class chemotherapeutic agent, plays a pivotal role in managing haematological cancers, particularly acute myeloid leukemia (AML) and acute lymphoblastic leukemia (ALL). This review presents a comprehensive statistical evaluation of daunorubicin’s effectiveness and safety, focusing on its pharmacokinetic and pharmacodynamic attributes. The most prevalent side effects included myelosuppression (85%), cardiotoxicity (10-15%), and gastrointestinal complications (60%). Statistical modelling highlighted a marked increase in cardiotoxicity risk with cumulative doses surpassing 550mg/m2 subgroup analysis identified age and comorbidities as significant predictors of treatment outcomes, with older patients and those with older patients and those with underlying cardiac conditions experiencing greater toxicity and reduced response rates. Innovative formulations, such as liposomal daunorubicin, were found to mitigate toxicity while maintaining efficacy. This study emphasizes the necessity of tailoring treatment plans to optimize dosing and patient selection, thereby improving therapeutic success and minimizing adverse events. The findings support further investigation into cardioprotective measures and personalized treatment strategies to enhance the clinical utility of daunorubicin.
Daunorubicin structural and molecular descriptors and their activity on DNA suppression:
Daunorubicin belongs to the class of anthracycline antibiotics and is utilized predominantly in chemotherapy for treating varieties of cancers such as leukaemia and solid tumours. Anthracycline, including daunorubicin, exact their therapeutic effect by binding between DNA base pairs, inhibiting the action of topoisomerase II, and including the production of free radicals that provoke DNA damage in cancer cells, ultimately resulting their demise.
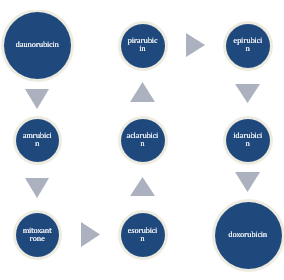
Fig:1Daunorubicin Classification is classified from Anthracycline [1]
Daunorubicin, a member of the anthracycline class, is renowned for its intricate molecular architecture robust anti-cancer properties:
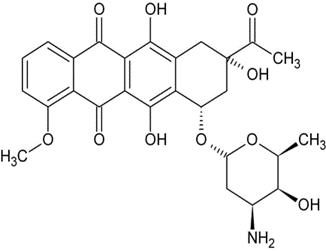
Molecular Compostion: It features a tetracyclic aromatic ring system with identified rings A, B, C, and D. attached is a daunosamine sugar moiety, enhancing solubility and influencing its pharmacokinetics. Multiple hydroxyl (- OH) groups augment its reactivity, pivotal for cellular interactions. The quinone structure within rings C and D instigates redox, generating reactive oxygen species (ROS) that impaired DNA integrity. Daunorubicin exhibits chirality, with the L- enantiomer holding therapeutic efficacy.
Mechanistic operations: - DNA intercalation disrupts replication and transcription, impeding cancer cells progression topoisomerase II inhibition hampers DNA unwinding, prompting apoptosis. ROS creation through quinone redox cycling intensifies DNA impairment and cytotoxicity. cellular entry via diffusion and active transport focuses accumulation within nuclei, intensifying DNA harm. Board-spectrum efficacy encompasses leukaemia’s, lymphomas and solid tumours, tempered by potential cardio toxicity and side effects. In conclusion, daunorubicin standards as a potent chemotherapeutic by means apoptosis induction and suppression of cancer cells proliferation via DNA impairment and essential cellular process interference. [3] Significance of Daunorubicin’s among anthracycline
Pioneering role: Daunorubicin was one of the first anthracycline introduced into clinical practice, setting the stage for other drugs like doxorubicin and epirubicin.
Leukaemia treatment: It is highly effective in treating acute myeloid leukaemia (AML) and acute lymphoblastic leukaemia (ALL), making it a key drug in induction therapy.
Mechanism of action: Daunorubicin intercalates into DNA, disrupts DNA and RNA synthesis, and generates free radicals causing DNA damage, making it highly effective at killing cancer cells.
Combination use: often used with other chemotherapy agents, daunorubicin enhances the efficacy of treatment regimens for various cancers.
Versatility: while crucial for leukaemia, daunorubicin is also used to treat various solid tumours, expanding its utility.
Research contributions: the development and use of daunorubicin have deepened understand ding of anthracycline chemistry and pharmacology, aiding in the design of new derivatives.
Clinical Importance: its role in clinical protocols for leukaemia and other cancers highlights its importance. Daunorubicin is a standard component in many chemotherapy regimens. Overall, daunorubicin pioneering role, efficacy, and versatility make it a cornerstone among anthracyclines, gently impacting oncology.[4]
????Statistics of daunorubicin: -
Paediatric patient [5]
|
Remission Rates |
Survival Rates |
|
About 80-90% of paediatric patients with AML achieve complete remission using daunorubicin based regimens.
|
5- year Survival Rate: - the 5-year survival rate for children treated with daunorubicin-based therapies is approximately 60-70% |
Younger Adults (male and female, under 60 years) [6]
|
Remission Rates |
Survival Rate |
|
Around 60-80% of younger adults attain complete remission with daunorubicin- based treatments. |
5-year survival rate: - the 5-year survival rate for younger adults treated with daunorubicin based regimens is roughly 40-50% |
Geriatric Patient (65 years and other)
|
Remission Rates:
|
Survival Rates:
|
|
Approximately 40-60% of elderly patients achieve complete remission with daunorubicin- based treatments, though the rate may be lower due to comorbidities and overall health status. |
5-year Survival rate: -the 5-year survival rate for elderly patients is typically lower, often around 10-20%, influenced by factors such as comorbidities and decreased tolerance to intensive chemotherapy. |
These statistics offer a general overview based on available clinical data and medical literature. For more precise and current statistics, especially regarding specific subgroups or newer treatment protocols, it is recommended to consult detailed clinical trial data and oncology treatment guidelines.[7]
Daunorubicin Remediable Cancers:
Types Of Cancers: - There are various types of cancers but few cancers are treated by daunorubicin they are
1.Leukemia
2. Breast Cancer
3.Sarcoma
4. Lymhoma
Leukemia: - leukemia is a cancer that targets the blood and bone marrow. It arises when the body generates excessive abnormal white blood cells, symptoms may include fatigue, frequent infection, easy brushing or bleeding, and anaemia. Leukaemia is categorized into several types, primarily acute or chronic, and further classified based on the affected blood cells (lymphoid or myeloid). Treatment can involve chemotherapy, radiation therapy, targeted therapy, and stem cell transplantation.[8]
Site Of Action: - Daunorubicin acts on major sites for treating leukemia are bone marrow, blood, CNS, lymph nodes, liver, spleen, kidney, lungs, heart.
Types Of Leukemia: -

Fig:2 Acute and chronic Breast cancers flow chart in females [9]
????Acute Lymphoblastic Leukaemia(All): -
|
Description |
Symptoms |
Treatment |
|
progressing leukaemia impacting lymphoid cells, a type of white blood cells. Common in altogether children, but also seen in grown-ups.
|
fatigue, fever, frequent infections, easy brushing or bleeding, bone and joint pain, tumescent lymph lumps.
|
chemotherapy, targeted antidote, radiation antidote, stem cell transplantation. |
????Acute Myeloid Leukaemia (AML) [10]
|
Description |
Symptoms |
Treatment |
|
A fast-advancing leukaemia affecting myeloid cells, precursors to chromatic blood cells including red blood cells, white blood cells, and platelets. Common in largely grown-ups, but can also come down in children.
|
Fatigue, fever, frequent infections, easy brushing or bleeding, weight loss, bone and joint pain.
|
chemotherapy, targeted antidote, stem cell transplant |
????Chronic Lymphocytic Leukaemia (CLL): -
|
Description |
Symptoms |
Treatment |
|
a laggardly progressing leukaemia that impacts lymphoid cells. It commonly starts in the bone keynote and can spread to blood and other body belt. Common in elderly grown-ups, rare in children. |
hourly asymptomatic in early stages, but may include fatigue, blown lymph lumps, weight loss, fever, night efforts. frequent infections.
|
observation for early stages, chemotherapy, targeted antidote, immunotherapy, stem cell transplant. |
????Chronic Myeloid Lukaemia (CML): -
|
Description |
Symptoms: |
Treatment |
|
sluggishly progressing leukaemia affecting myeloid cells, characterized by the Philadelphia chromosome, a inheritable abnormality. Common in substantially grown-ups.
|
Frequently asymptotic in early stages, but may include fatigue, weight loss, night sweats, fever, splenomegaly (enlarged spleen). treatment targeted remedy with tyrosine kinase impediments, chemotherapy, stem cell transplant. Hairy cell leukemia a rare, slow – growing leukemia where the cells appear ‘hairy’ under a microscope. It generally affects middle-aged grown-ups. T-cell prolymphocytic Leukemia (T-PLL) A rare and aggressive leukemia affecting T-cells, more common in elderly grown-ups. Adult T-cell leukemia/polyp (ATLL) linked to infection by the earthborn T-lymphotropic fungicide (HTLV-1), affecting T-cells |
observation for early stages, chemotherapy, targeted antidote, immunotherapy, stem cell transplant. |
Statistics Of Leukemia: -
Leukemia incidence and mortality rates vary significantly across different regions and countries. Here are some findings based on recent data: -
Global Incidence: -In 2020, there were approximately 474,519 new cases of leukemia worldwide. The global age standardized incidence rate was 5.4 per 100,000 people. Regions with the highest incidence rates include North America (ASR 10.9), Australia/ New Zealand (ASR 10.4), and Western Europe (ASR 8.5). conversely, the lowest incidence rates were observed in Middle Africa (ASR2.2), western Africa (ASR 2.3), and Eastern Africa (ASR 3.3).
Gender Difference: - Men generally have a higher incidence rate (ASR 6.3) compared to women (ASR 4.5), with greater disparities in regions with higher overall incidence rates.
Income Disparities: - Higher- Income countries tend to have higher incidence rates of leukemia. High-income countries have an ASR of 8.4, compared to 3.4 in low- income countries.
Mortality Rates: - In 2020, there were around 311,594 deaths due to leukemia globally. Mortality rates show less regional variation, typically ranging from 2.5 to 4.0 per 100,000 people. Western Asia had the highest mortality rate at 4.6 per 100,000, which is 40% higher than the global average of 3.3 per 100,000.[12][13]
TRENDS OVER TIME: - Between 1990 and 2017, the number of newly diagnosed leukemia cases increased globally, but the age-standardized incidence rate (ASIR) slightly decreased by 0.43% per year. Notably, the highest incidence rates shifted from high SDI (Socio-Demographic Index) regions in 1990 to high-middle SDI regions by 2017.[13]
Country-Specific-Data: - In 2017, Syria had the highest national ASIR of leukemia at 14.83 per 100,000 followed by the UK, Denmark, and Lebanon. Conversely, countries like Bahrain experienced the most significant decreases in ASIR during the same period.
Table:1 Statistical survey on new cases, Death and Survival rates
|
Country |
New cases (per 100,000) |
Deaths (per 100,000) |
5-year Survival Rate (%) 2019-2024 |
|
United states |
14.1 |
6.6 |
62.4 |
|
United Kingdom |
9.7 |
5.1 |
59.0 |
|
Canada |
12.2 |
5.8 |
63.0 |
|
Germany |
10.8 |
5.4 |
60.5 |
|
France |
10.3 |
4.9 |
61.2 |
|
Japan |
11.5 |
5.2 |
58.7 |
|
Australia |
10.5 |
5.1 |
64.1 |
|
China |
4.5 |
3.1 |
35.0 |
|
India |
3.2 |
2.7 |
20.0 |
|
Brazil |
3.2 |
4.1 |
40.0 |
|
Russia |
6.7 |
5.0 |
35.0 |
|
South Korea |
8.9 |
4.2 |
54.0 |
|
Mexico |
8.4 |
3.5 |
25.0 |
|
Italy |
9.9 |
5.0 |
59.5 |
|
Spain |
10.1 |
5.1 |
60.0 |
|
South Africa |
4.8 |
3.3 |
30.0 |
|
Egypt |
3.5 |
2.8 |
25.0 |
|
Turkey |
6.5 |
4.0 |
38.0 |
|
Argentina |
7.2 |
4.5 |
45.0 |
|
Indonesia |
3.0 |
2.5 |
18.0 |
These statistics are based on data collected from various sources and reflect the incidence, mortality, and survival trends for leukemia globally.[14]
Breast Cancer: - Breast cancer originates in the breast tissue and primarily affect women, though men can also be diagnosed. It arises when breast cells begin to grow uncontrollably, leading to the formation of a tumour, which may be felt as a lump. While the precise cause remains unclear, several risk factors, such as genetics, age, hormonal influences, and lifestyle choices, contribute to its development. The are different types of breast cancer, with invasive ductal carcinoma being the most prevalent. Common symptoms include a noticeable lump, alterations in breast shape or size and unusual nipple discharge. Detecting breast cancer early through mammograms and self- examinations can greatly enhance treatment success. Standard treatment approaches include surgery, radiation, chemotherapy, and hormone therapy, tailored to the cancers stage and type. Ongoing research is focused on improving understanding and treatment options, ultimately striving for better patient outcomes and quality of life.[15]
Site Of Action: - Daunorubicin acts on major sites for treating breast cancer are bone marrow, blood, CNS, lymph nodes, liver, spleen, kidney, lungs, heart.[16]
Types Of Breast Cancer: - Breast cancer are observed in both females and males as following types: -
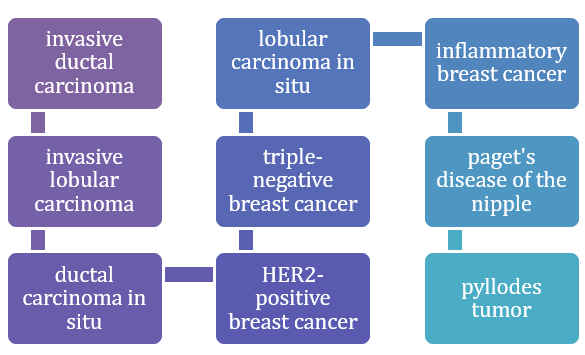
Fig:3 Types of Breast cancer in females
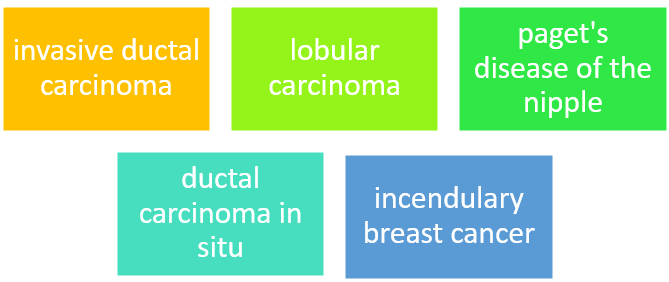
Fig:4 Types of Breast cancer in Males
Types Of Female Breast Carcinoma: -
Invasive Ductal Carcinoma (IDC): -
|
Description |
Symptoms |
Treatment |
|
Most common type, starts in the milk channels and invades enclosing tissue. |
lump in the breast, changes in breast shape or size, skin changes |
surgery, chemotherapy, radiation, hormone antidote |
Invasive Lobular Carcinoma (ILC): -
|
Description |
Symptoms |
Treatment |
|
begins in lobules (milk producing glands) and can spread |
thickening of breast tissue, now no distinct lump.
|
alike to IDC surgery, chemotherapy, radiation |
Ductal Carcinoma in Situ (DCIS): -
|
Description |
Symptoms |
Treatment |
|
Non-invasive, confined to tubes without spreading |
hourly no symptoms; may determine through mammograms |
surgery (lumpectomy or mastectomy), radiation |
Triple – Negative Breast Cancer:
|
Description |
Symptoms |
Treatment |
|
Lacks oestrogen, progesterone receptors and HER2 protein |
alike to IDC, more aggressive |
chemotherapy, surgery, radiation; no hormone therapy |
Her2 – Positive Breast Cancer: -
|
Description |
Symptoms |
Treatment |
|
Overexpression of HER2 protein, can be aggressive |
Alike to IDC, more aggressive |
Targeted antidotes (like trastuzumab), chemotherapy |
Inflammatory Breas Cancer (IBC): -
|
Description |
Symptoms |
Treatment |
|
Rare and aggressive, causes breast to go red and blown |
Warmth, skin changes, and fast growth |
chemotherapy, surgery, radiation |
Paget’s Disease of The Nipple: -
|
Description |
Symptoms |
Treatment |
|
Affects the nipple and areola, constantly associated with DCIS or invasive cancer. |
Itching, reddishness, flaking or discharge from the nipple |
Surgery (lumpectomy or mastectomy), may include radiation |
Phyllodes Tumor: -
|
Description |
Symptoms |
Treatment |
|
Rare, can be benign or malicious; grows in connective tissue |
mobile lump in the breast
|
Surgical disposal, monitoring |
Metaplastic Breast Cancer: -
|
Description |
Symptoms |
Treatment |
|
Rare, contains different types of cells; can be aggressive |
Hard lump, skin changes |
Surgery, chemotherapy, but hourly less responsive to standard treatments |
Types Of Breast Cancer in Males: -
Invasive Ductal Carcinoma (IDC): -
|
Description |
Symptoms |
Treatment |
|
Correspondent to IDC in females, starts in the channels |
Lump in the breast, changes in skin or nipple |
Surgery, chemotherapy, radiation, hormone antidote |
Ductal Carcinoma in Situ (DCIS): -
|
Descrption |
Symptoms |
Treatment |
|
non-invasive condition confined to channels
|
Again, and again asymptomatic; detected through imaging |
Surgery, may involve radiation |
Lobular Carcinoma: -
|
Description |
Symptoms |
Treatment |
|
Rare in males; arises in lobular tissue |
again, and again no distinct lump, implicit breast changes |
Surgery, perhaps radiation
|
Incendiary Breast Cancer (IBS): -
|
Description |
Symptoms |
Treatment: |
|
Genuinely rare in men, aggressive type. |
Swelling, brightness, warmth
|
Chemotherapy followed by surgery |
Paget’s Disease of The Nipple: -
|
Description |
Symptom |
Treatment |
|
Rare form affecting the nipple area |
Itching, discharge, changes in nipple skin
|
Surgery, may include radiation General symptoms of breast cancer in both genders: - Lump or mass in the breast Change in breast shape or size Skin dimpling or aggro Nipple discharge |
Statistics Of Breast Cancer: -
Global occurrence breast cancer is the most common cancer among women completely, with over 2 million new cases each cycle.
Table:2 statistics data based on gender
|
Demographic |
Incidence rate (per 100,000) |
Death rate (per 100,000) |
5- year survival rate 2019-2024 |
|
Females |
129.1 |
20.3 |
90% |
|
Males |
1.3 |
0.2 |
84% |
|
Children |
Rare |
Rare |
- |
|
Adults (18-64) |
Majority of cases |
Varies by age group |
85% |
|
Geriatric (65+) |
Higher incidence |
Higher death rate |
85% |
|
Total |
Varies by region |
19.9 |
90% |
By gender: -
Females: -Occurrence breast cancer primarily affects women, representing about 99 of cases, date hazard. around 1 in 8 women (12.5) will be diagnosed with breast cancer during their duration. Survival rates early findings and treatment advancements have led to a 5 – cycle relative survival rate of about 90 in high-income countries.
Males: - Occurrences although, men can develop breast cancer, constituting about 1 of all cases.
Hazard factors contributing factors include inborn mutations (e.g. BRCA2) family history, radiation exposure, and hormonal imbalances.
Survival rates due to lower knowledge, breast cancer in men is hourly diagnosed at subsequent stages, which can negatively impact survival rates.[21]
By age: -
Geriatric Population (65 Cycles and Old): - occurrence the hazard of developing breast cancer increases with age, with the top rates seen in women grew 65 and aloft.
Challenges again grown -ups may feel added complications, alike as comorbidities, which can affect treatment and outgrowths.
Survival rates although slightly lower than in younger population, effective treatment is still vital for again grown-ups.
Adults (18 -64 ages): - constancy last breast cancer cases are diagnosed in women aged 40-64.web regular mammograms and complexion- quizzes are vital for early finding in this age group.
Survival rates adolescent women (under 40) may encounter more aggressive forms of breast cancer, but overall survival rates are high with proper treatment.
Children and adolescents: - chronicity breast cancer is exceeding rare in children and adolescents. Cases when it occurs, it’s over and over associated with hereditary conditions or radiation exposure. Treatment paediatric breast cancer requires technical treatment and long- term follow-up due to possible movables on growth and development.[22]
Country – Specific- Data: -
Table:3 Statistics data based on country specificity
|
Country |
Incidence rate (per 100,000) |
Death rate (per 100,000) |
5-year survival rate 2019-2024 |
|
United states |
129.1 |
20.3 |
90% |
|
Canada |
98.3 |
18.7 |
88% |
|
United Kingdom |
95.0 |
17.1 |
85% |
|
Australia |
94.2 |
16.5 |
87% |
|
India |
25.8 |
12.7 |
66% |
|
China |
36.1 |
8.8 |
75% |
|
Brazil |
62.9 |
15.2 |
78% |
|
Germany |
62.5 |
15.6 |
87% |
|
Japan |
63.1 |
9.3 |
85% |
|
South Africa |
45.3 |
22.6 |
65% |
These statistics are based on data collected from various sources and reflect the incidence, mortality, and survival trends for leukemia globally.[23]
Sarcoma: - Sarcoma is a cancer that develops in connective tissues, including bones, muscles, fat, and blood vessels. It differs from carcinomas, which come from epithelial cells, and is relatively rare. Sarcoma can be categorized into several types, such as osteosarcoma (affecting bones), liposarcoma (affecting fat), and leiomyosarcoma (affecting smooth muscle). Symptoms vary based on the tumour’s location and may involve swelling, pain or the presence of a lump. Treatment usually includes surgery, radiation and chemotherapy, tailored to the specific type and stage of the cancer.[24]
Site Of Action: -Daunorubicin acts on major sites for treating sarcoma are bone marrow, blood, CNS, lymph nodes, liver, spleen, kidney, lungs, heart.[25]

Statistics Data: -
Country- Specific- Data: -
|
Country |
Incidence rate (per 100,000 people annually) |
5-year survival rate (%) 2019-2024 |
|
United states |
4.0 |
65 |
|
United Kingdom |
3.0 |
55-60 |
|
Germany |
3.5 |
60-65 |
|
France |
2.5 |
60 |
|
Japan |
2.2 |
70 |
|
Australia |
3.5 |
60-65 |
|
Canada |
4.0 |
65 |
|
Italy |
3.0 |
60-65 |
|
Spain |
2.8 |
60 |
|
Sweden |
3.5 |
65 |
|
Brazil |
2.5 |
50-55 |
|
India |
1.5-2.0 |
50 |
|
South Korea |
2.0 |
65-70 |
|
China |
1.5 |
55-60 (urban areas) |
|
Mexico |
2.2 |
50-55 |
Table: - 4 These statistics are based on data collected from various sources and reflect the incidence, mortality, and survival trends for leukemia globally.
By Gender: - Sarcoma are generally more common in males than in females, with the male-to-female rate varying by specific sarcoma subtype. Overall, about 60 of sarcoma cases occur in males and 40 in females.
By Age: -
|
Children And Adolescents: |
Young Adults |
Adults |
Geriatric Population |
|
Sarcoma is the most common type of solid growths in children. Rhabdomyosarcoma is the most going type among this age group, with an occurrence of about 4-5 cases per million in children matured 0-14 years.
|
Adolescents and young adults (ages 15-39) also feel significantly frequency, particularly for osteosarcoma and Ewing sarcoma, with rates ranging from 1-2 cases per million.
|
Sarcoma are less common in aged grown-ups, but specific subtypes like leiomyosarcoma and liposarcoma can befall more often in middle-aged and elderly populations, with an overall occurrence of about 3-4 cases per 100,000 beings. |
Occurrence rates can increase in geriatric grown-ups, especially for soft tissue sarcomas. Those aged 65 and old tend to present with more aggressive forms of sarcoma.
|
Lymphoma: - Lymphoma is a cancer that develops in the lymphatic system, part of the immune system. It mainly targets lymphocytes, a type of white blood cells crucial for fighting infections. There are two primary forms: - Hodgkin lymphoma, marked by Reed-Sternberg cells, and non – Hodgkin lymphoma, a more common and varied group lacking these cells. Symptoms often include swollen lymph nodes, fever, night sweats, weight loss, fatigue and itching. Treatment depends on the lymphoma’s type and stage and may involve chemotherapy, radiation therapy, targeted therapy, targeted therapy, and sometimes stem cell transplant.[29]
Site Of Action: - Daunorubicin acts on major sites for treating lymphoma are bone marrow, blood, CNS, lymph nodes, liver, spleen, kidney, lungs, heart.
Types of lymphoma: - The are several types of lymphoma, broadly categorized into two main groups: -
HODGKIN LYMPHOMA (HL) and NON-HODGKIN LYMPHOMA(NHL): -

Fig: - 6 Hodgkin Lymphoma (HL)
NON -HODGKIN LYMPHOMA (NHL): -NHL includes a diverse group of lymphomas, classified based on the type of lymphocyte (B-CELL or T-CELL) they originate from and their growth rate.

Fig: - 7 B-Cell Lymphomas: -
Fig: - 8 T-Cell and NK-Cell Lymphomas: -
Hodgkin Lymphoma (HL): -
Classical Hodgkin Lymphoma (CHL): -
Nodular Sclerosis Hodgkin Lymphoma (NSHL): - The most common subtype, characterized by large cancerous Reed-Sternberg cells and bands of connective tissue (sclerosis) dividing the lymph lump.
Mixed Cellularity Hodgkin Lymphoma (MCHL): - Features a combination of different types of cells, including Reed -Sternberg cells. Common in elderly grown-ups and people with HIV.
Lymphocyte-Rich Hodgkin Lymphoma (LRHL): - A rare subtype with multiple lymphocytes and countless Reed-Sternberg cells. Hourly institute in upper body lymph lumps.
Lymphocyte-Depleted Hodgkin Lymphoma (LDHL): - The rarest subtype, with multiple lymphocytes and abundant Reed-Sternberg cells. More common in old grown-ups and those with HIV.
Nodular Lymphocyte- Predominant Hodgkin Lymphoma (NLPHL): - A rare subtype characterized by large, popcorn-shaped cells. It generally has a slower progression and better prognosis than classical Hodgkin lymphoma.[30]
Non- Hodgkin Lymphoma (NHL): -
B-Cell Lymphomas: -
Diffuse Large B-Cell Lymphoma (DLBCL): - The most common NHL subtype, characterized by large, fast growing B cells. It’s aggressive but major responds well to treatment.
Follicular Lymphoma (FL): -A slow- growing lymphoma that forms in the lymph lumps in a circuitous (follicular) pattern. It can make over into a more aggressive form over time.
Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma (CLL/SLL): - CLL primarily affects the blood and bone core, while SLL affects lymph lumps. They are slow-growing and have a comparable cellular appearance.
Mantle Cell Lymphoma (MCL): - A rare, aggressive subtype that starts in the mantle zone of lymph lumps. It’s again and again diagnosed at an advanced stage.
Burkitt Lymphoma: - A broadly aggressive lymphoma that big involves the jaw or abdomen. It’s linked to the Epstein-Barr venom and is common in children in Africa.
Marginal Zone Lymphoma (MZL): - It includes subtypes like mucosa- associated lymphoid tissue (MALT) cancer, which hourly begins in the stomach and is associated with certified inflammation;
Primary Mediastinal B-Cell Lymphoma (PMBCL): - A subtype of DLBCL that ordinarily affects adolescent grown-ups and births in the thymus gland in the mediastinum (chest area).[31]
T-Cell Lymphomas: -
Peripheral T-Cell Lymphomas (PTCL):- A group of aggressive cancers that develop from mature T-cells. The are hourly diagnosed at an advanced stage and have chromatic subtypes.
Cutaneous T-Cell Lymphoma (CTCL): - Include mycosis fungoides and Sezary development, which primarily affect the skin but can spread to other organs.
Anaplastic Large Cell Lymphoma (ALCL): - An aggressive lymphoma that can be systemic or cutaneous. It’s characterized by large, anaplastic cells and can be ALK-positive or ALK-negative, moving prognosis.
Other Less Common NHL Subtypes: -
Primary Central Nervous System (CNS) Lymphoma: - A rare lymphoma that starts in the brain, spinal cord, or eyes. It can be either B-cell or T-cell in origin.
Lymphoblastic Lymphoma: - A double- quick-growing lymphoma that resembles acute lymphoblastic that resembles ACUTE Lymphoblastic Leukemia (ALL) and primarily affects children and immature grown-ups.[32]
Statistical Data of Lymphoma: -
Country-Specific-Data: -
Table: - 5 These statistics are based on data collected from various sources and reflect the incidence, survival rates and deaths for leukemia globally.[33]
|
Country |
New cases |
Survival rate (5-year) in percentage (%) |
Deaths 2019-2024 |
|
United states |
83,087 |
72 |
20,140 |
|
China |
88,200 |
50 |
39,500 |
|
India |
40,000 |
60 |
24,000 |
|
Brazil |
12,500 |
65 |
6,000 |
|
Russia |
14,600 |
55 |
7,300 |
|
Japan |
14,500 |
68 |
6,800 |
|
Germany |
14,000 |
70 |
6,000 |
|
United Kingdom |
11,600 |
65 |
5,200 |
|
France |
10,200 |
68 |
4,600 |
|
Italy |
12,800 |
67 |
5,500 |
|
Canada |
9,500 |
74 |
2,200 |
|
Australia |
6,400 |
76 |
1,500 |
|
South Korea |
5,000 |
65 |
2,200 |
|
Mexico |
6,000 |
55 |
3,000 |
|
Spain |
8,000 |
68 |
3,500 |
|
South Africa |
5,800 |
52 |
2,900 |
|
Argentina |
5,200 |
60 |
2,400 |
|
Turkey |
5,400 |
60 |
2,800 |
|
Indonesia |
4,000 |
55 |
2,200 |
|
Saudi Arabia |
2,500 |
62 |
1,100 |
General Statistics: -
Non-Hodgkin Lymphoma (NHL): -Represent about 4-5 all cancers in the United States. Additional conventional than Hodgkin lymphoma. Estimated 80,470 new cases in the U. S in 2023.life hazard is like 1 in 42 for men and 1 in 52 for women.
Hodgkin Lymphoma (HL): - comprises about 0.5 of all cancers in the U.S. estimated 8,830 new cases in the U.S in 2023. Life hazard is about 1 in 432 for men and 1 in 454 for women.
Distribution By Age: -
|
Children And Adolescents |
Adults |
Geriatric |
|
NHL Accounts for about 5 of childhood cancers and HL most common in days 15-39, with a peak in the 20s.
|
NHL the hazard increase with ages, with about half of cases diagnosed in beings 65 or older and HL shows a bimodal distribution with peaks in young maturity (ages 20-30) and after adulthood (ages 55 and other) |
NHL appearance rises with age, peaking in those grew 80 and older.
|
Gender Distribution: -
|
Non-Hodgkin Lymphoma |
Hodgkin Lymphoma |
|
Men evolved continuousness compared to women. Women slightly lower frequency than men. |
Men slightly developed chronicity compared to women. Women slightly lower chronicity than men. |
Percentage Breakdown: -
|
Children Adolescents (0-19 Years): |
Adults (20-64 Years) |
Geriatrics (65 Years) |
|
NHL about 5 of cases and HL about 15-20 cases. |
NHL around 50 of cases and HL about 60 of cases. |
NHL about 45-50 of cases and HL around 20-25 of cases |
Fig: - 9 Effects of daunorubicin on particular organ for treating leukemia as follows: -
Bone Marrow: -
|
Mechanism Of Action |
Site Of Action |
Uses |
Adverse Effects |
Pharmcodynamics |
Pharmacokinetics |
|
Daunorubicin primarily intercalates into DNA, breaking the enzyme topoisomerase II. This prevents DNA from unwinding and duplicating, thereby inhibiting DNA and RNA amalgamation. This leading to apoptosis (programmed cell death) of hastily dividing cells, comparable as cancer cells.
|
Daunorubicin targets the bone marrow centring on fast dividing leukemic cells.
|
daunorubicin is by and large used to treat AML AND ALL it can also be combined with other chemotherapeutic agents to enhance its effectiveness.
|
Common adverse effects of daunorubicin include Myelosuppression (depleted blood cell output) Cardiotoxicity (which can lead to congestive heart failure with elongated use) Nausea and gagging Mucositis (inflammation of the mucous membranes) Alopecia (hair loss) Hepatoxicity (liver damage) Born tissue necrosis if extravasation occurs during intravenous administration |
Onset of action daunorubicin acts enough full tilt due to its intravenous administration. Duration of action its effects on the bone marrow and leukemic cells can last for several days to weeks. Half-life the plasma half-life of daunorubicin is around 18.5 hours, though this can vary among objects. Overall, daunorubicin is an effective chemotherapeutic agent for leukemia treatment, but it’s use is associated with significant dangers and side effects that challenge careful monitoring and management |
Administration: - Attention daunorubicin is administered intravenously, guaranteeing full bioavailability. DISTRIBUTION: - It’s generally distributed throughout the body, including the heart, classes, liver and lungs. METABOLISM: - Daunorubicin is primarily metabolized in the liver to daunorubicinol, an active metabolite. EXCERTION: - It’s excreted through the biliary system into the faeces and also in the urine.
|
Liver: -
Daunorubicin, an anthracycline antibiotic, is broadly applied in treating leukemia, particularly AML and ALL. This overview highlights its employment in leukemia treatment with a focus on its liver movables.
|
Mechanism Of Action |
Uses |
Adverse Effects |
Effects On Liver |
Pharmcodymanics |
Pharmcokinectics |
|
Daunorubicin functions by working in into DNA strands, hindering the synthesis of DNA and RNA. it stabilizes the topoisomerase II complex after it breaks the DNA chain for replication, staving off the DNA double helix from being resealed and leading to cell death. This makes it particularly effective against briskly dividing cancer cells.
|
Acute Myeloid leukemia (AML) daunorubicin is continually combined with other chemotherapy agents, alike as cytarabine, for the induction treatment protocois for ALL, particularly in induction antidote. Other cancers while primarily used for leukemia, daunorubicin can be applied in treating other cancers as part of chromatic chemotherapy governances.
|
Cardiotoxicity a major concern with daunorubicin and other anthracyclines, manifesting as cardiomyopathy or congestive heart failure. Myelosuppression leads to lower blood cell output, acting in anaemia, increased infection hazard and bleeding. Gastrointestinal venom normally causes nausea, hurling, mucositis and diarrhoea. Alopecia hair loss is continually observed. Hepatoxicity elevated liver enzymes indicating liver damage or dysfunction can go down. Secondary spleen long term use may increase the danger of developing secondary cancers.
|
Hepatotoxicity can bring a but liver damage, bore out by elevated liver enzymes due to direct hepatocyte venom and reactive oxygen species generation, monitoring liver function tests are vital before and during treatment to turn up hepatoxicity prematurely, medication adaptations or expiration may be necessary if significant liver damage occurs. Daunorubicin is a potent chemotherapeutic agent but its use requires careful governance of adverse effects, particularly hepatoxicity and cardiotoxicity, to optimize healing aftereffects in leukemia treatment |
Cytotoxic conditioning induces cytotoxicity through DNA intercalation, topoisomerase II inhibition and free radical generation, contributing to apoptosis of cancer cells. Therapeutic window has a narrow curative window, needing careful dosing and monitoring to balance efficiency and venom |
Absorption: -Daunorubicin is administered intravenously and has poor oral bioavailability DISTRIBUTION: - generally distributed throughout the body, with high concentrations in the liver, spleen, classes, and heart. METABLOSIM: - primarily metabolized in the liver to daunorubicinol, an active metabolite. EXCRETION: - Excreted via acidity and urine. The elimination half-life is about 18.5 hours.
|
Spleen: - Daunorubicin is an anthracycline antibiotic extensively utilized in treating various leukamia, including those involving the spleen.
|
Mechanism Of Action |
Site Of Action |
Uses |
Adverse Effects |
Pharmcodynamics |
Pharmcokinetics |
|
Daunorubicin intercalates into DNA, disrupting the synthesis of DNA and RNA crucial for cancer cell growth. it also inhibits topoisomerase II , causing DNA strand breaks, leading to the inhibition of nucleic acid synthesis and the induction of apoptosis in cancer cells.
|
The primary site of action for daunorubicin is the DNA within the cell nucleus. In leukemia involving the spleen, daunorubicin targets malignant white blood cells found in the bone marrow, peripheral blood and spleen |
Daunorubicin is mainly used to treat AML and ALL and other leukaemia’s as a part of combination chemotherapy regimens.
|
Myelosuppression (bone marrow suppression) Nausea and vomiting Mucositis (inflammation of the mucous membrane) Alopecia (hair loss) Cardiotoxicity (damage to the heart muscle)
|
Onset of action: Effects on cell cycle arrest and apoptosis initiation occur shortly after administration. Duration of action: - Antitumor effects last for the cell cycle duration of malignant cells. Peak plasma concentration: - Achieved rapidly after intravenous administration. Therapeutic window: - Dosage is carefully calibrated to optimize efficacy while minimizing toxicity, especially cardiotoxicity. Daunorubicin’s effectiveness in treating spleen leukemia lies in its capacity to target rapidly dividing cells, effectively eradicating cancerous cells in the spleen and other affected areas. However, it’s use requires careful monitoring and management due to potential serious side effects |
ABSORPTION: - Administered intravenously with immediate absorption. DISTRIBUTION: - Widely distributed throughout the body, particularly in the spleen, liver, kidneys, and bone marrow. METABOLISM: - Mainly metabolized by the liver into active and inactive metabolites. EXERCTION: -Primarily excreted through bile and faces, with a minor amount excreted in urine. Half- life: - Approximately 18.5 hours for the terminal elimination phase.
|
Lymph Nodes: -
|
Mechanism Of Action |
Effects On Lymph Nodes |
Uses: |
Adverse Effect |
Pharmacodynamics |
Pharmcokinetics |
|
Daunorubicin works by intercalating into DNA, thereby disrupting DNA replication and transcription. It also inhibits the enzyme topoisomerase II, causing DNA strand breaks and cell death. Additionally, daunorubicin generates free radicals that further damage cellular components.
|
In leukemia treatment, daunorubicin targets rapidly dividing leukemic cells, including those in the lymph nodes. It’s cytotoxic effects lead to the destruction of these malignant cells, reducing the tumour burden in the lymph nodes. |
AML often used in combination with ither chemotherapeutic agents to induce remission. ALL part of combination chemotherapy regimens. Other hematologic malignancies sometimes utilized for other leukemia and lymphomas depending on the specific treatment protocol.
|
Hematologic: - Myelosuppression, causing neutropenia, thrombocytopenia and anaemia. Cardiotoxicity, alopecia Gastrointestinal: - Nausea, vomiting, mucositis
|
Onset of action: - Rapid, affecting dividing cells soon after administration. DURATION OF ACTION: - Cytotoxic effects can last several days due to the drug’s long half-life and ongoing presence of metabolites. THERAPEUTIC EFFECTS: -Decreases leukemic cell counts and improves clinical symptoms of leukemia overall, daunorubicin is a powerful chemotherapeutic drug used to treat leukemia, including those affecting lymph nodes |
Absorption: - Given intravenously DISTRIBUTION: - Quickly distributed to tissues, particularly in highly vascular organ. Poor penetration of the blood – brain barrier. METABOLISM: - Mainly metabolized in the liver to active and inactive metabolites. ELIMINATION: - Excreted primarily through bile and urine. The half- life typically ranges from 18 to 55 hours.
|
Central Nervous System: -
|
Mechanism Of Action |
Site Of Action |
Uses |
Adverse Effects |
Pharmacokinetics: -
|
Pharmcodynamics: |
|
DNA intercalation daunorubicin inserts itself between DNA base couples, fragmenting the admixture of DNA and RNA. Topoisomerase II inhibition it inhibits topoisomerase II, an enzyme required for DNA unwinding, thereby blocking DNA replication and transcript. Free radical arrangement daunorubicin produces free extremists, which bring about DNA strands breaks and damage cell membranes. |
CNS daunorubicin doesn’t significantly cross the blood- brain barrier, making it less effective for CNS leukemia.
|
AML a vital element in induction therapy. ALL hourly used in combination with other chemotherapy agents.
|
Cardiotoxicity hazard of heart failure, especially with additive medications, myelosuppression significant bone core inhibition leading to neutropenia, thrombocytopenia and anaemia. Gastrointestinal venom causes nausea, hurling mucositis, and diarrhoea. alopecia normally results in hair loss. extravasation can catalyse severe indigenous tissue damage if it leaks from the vein during administration.
|
ADMINISTRATION: - Given intravenously DISTRIBUTION: - Generally distributed in body tissues but doesn’t cross the blood-brain barrier well. METABOLISM: - Basically, metabolised in the liver to both active and inactive metabolites. EXCRETION: -primarily excreted via acidity and faeces, with some renal excretion.
|
Action on cancer cells daunorubicin’s cytotoxic effects are due to DNA intercalation and topoisomerase II inhibition, leading to programmed cell death in cancer cells. Timing of effects maximum effective against fast dividing cells, particularly during the S phase of the cell cycle, but it can affect cells in other phases too
|
Kidneys: -
|
Mechanism Of Action |
Uses |
Adverse Effects |
Pharmacodnamics |
Pharmcokinetics: -
|
|
Daunorubicin in the kidneys DNA intercalation and inhibition of topoisomerase II daunorubicin intercalates into DNA and inhibits the enzyme, topoisomerase II, leading to the inhibition of DNA replication and transcription. While this action is systemic, it can impact rapidly dividing cells in the kidneys, contributing to nephrotoxicity. Generation of free radicals: daunorubicin generates free radicals that can cause oxidative damage to kidney cells, leading to cellular injury and apoptosis. |
use of nephroprotective agents or antioxidants to reduce oxidative stress and protect renal cells
|
Daunorubicin can cause direct nephrotoxicity, leading to damage of the renal tubules and glomeruli. Acute kidney injury- patients receiving daunorubicin may develop AKI, characterized by a sudden decline in kidney function. Chronic kidney disease- long term use or high doses of daunorubicin can contribute to the development of CKD. Proteinuria: - the presence of protein in the urine is a sign of kidney damage caused by daunorubicin.
|
Cellular damage: the drug’s ability to induce DNA damage and generate free radicals can lead to renal cell injury. Induction of apoptosis: - the oxidative stress and DNA damage caused by daunorubicin can trigger apoptosis renal cells.
|
ABSORPTION: - Daunorubicin is administered intravenously and is rapidly distributed throughout the body. DISTRIBUTION: - The drug is distributed to various organ, including the kidney, where it can exert its effect. METABOLISM: -Daunorubicin is metabolised in the liver to both active and inactive metabolites, which can also be nephrotoxic. EXCRETION: - Daunorubicin and its metabolites are excreted via the bile and urine, with significant renal excretion contributing to potential nephrotoxicity.
|
Lungs: -
|
Mechanism Of Action |
Site Of Action |
Adverse Effects |
Pharmcokinetics |
Pharmcodynamics |
|
Daunorubicin works primarily through intercalation into DNA, which disrupts the function of topoisomerase II enzyme. This disruption prevents the displacement of DNA strands and thereby inhibits DNA replication and RNA synthesis, leading to cell death. Daunorubicin also generates free revolutionists that damage cellular components, including DNA, proteins and lipids. |
While daunorubicin is used to treat leukemia, which primarily affects the bone marrow and blood, its effects can be systemic, impacting varied organs, including the lungs. The lungs aren’t the primary site if action but can be affected by the medicament’s systemic distribution.
|
Pulmonary poison daunorubicin can create pulmonary poison, though it’s less common compared to cardiotoxicity. Symptoms may include coughing, conciseness of breath and in severe cases, interstitial pneumonitis or pulmonary fibrosis. Infection due to myelosuppression (diminished bone marrow conditioning) cases are at evolved danger for infections, including respiratory infections.
|
ADMINISTRATION: - Daunorubicin is naturally administered intravenously, assuring fast clearness in the bloodstream. DISTRIBUTION: - It has a wide distribution in the body, including penetration into the lungs. It binds largely to plasma proteins. METABOLISM: - primarily metabolized in the liver to daunorubicinol, an active metabolite. EXCRETION: - Banned through acidity and urine the elimination half-life is about 18.5 hours for daunorubicin and 26.7 hours for daunorubicinol.
|
Effect on cancer cells daunorubicin’s capacity to work into DNA and inhibit topoisomerase II leads to apoptosis in fast dividing cells, including leukemic cells. Systemic effects: - the systemic administration of daunorubicin means it affects multiple organ systems, with the lungs potentially knowing adverse effects due to its distribution and capability for causing oxidative stress and tissue damage.
|
Skin: -
|
Mechanism Of Action |
Site Of Action |
Adverse Effects |
Pharmacokinetics |
Pharmacodynamics |
|
Daunorubicin is an anthracycline antibiotic that works primarily by intercalating DNA strands, thereby inhibiting DNA strands, thereby inhibiting DNA emulsion and function, it also inhibits the enzyme topoisomerase II, helping the relaxation of supercoiled DNA, which is essential for DNA replication and transcription. These bearing lead to cell death, particularly in fast dividing cancer cells.
|
for leukemia, the primary site of action for daunorubicin is the bone spirit, where it targets leukemic cells. Truly so, when considering cutaneous externalization of leukemia (leukemia cutis), daunorubicin can affect the skin dead by reducing the leukemic cell burden in the bloodstream and bone marrow, potentially leading to a decline in leukemic skin infiltration.
|
Myelosuppression a significant reduction in bone marrow exertion, leading to decreased of blood cells. Cardiotoxicity can bring damage to the heart muscles, leading to cardiomyopathy and congestive heart failure, especially with accumulative medicaments. Gastrointestinal venom includes nausea, barfing, mucositis and diarrhoea Alopecia hair loss is a common side effect Extravasation can bring severe tissue damage if the medicament leaks out of the mode during administration Skin takes although rare, daunorubicin can bring domestic answers so as erythema, rash and hyperpigmentation. |
ADMINISTRATION: - Given intravenously, assuring complete bioavailability’ DISTRIBUTION: -Largely distributed throughout the body, with high uptake in the liver, spleen, and heart. METABOLISM: - primarily metabolized in the liver to an active metabolite, daunorubicinol EXCRETION: - Excreted through the acidity and urine. The half- life of daunorubicin is about 18.5 hours.
|
Onset of action: -the cytotoxic effects on leukemic cells are immediate, but clinical reactions may take days to weeks. Duration of action: - effects persist as long as the medication remains in the system and for a period after due to the medicament’s intercourse with cellular DNA. medicament response relationship edge and venom are pharmaceutical – dependent, with helped medication effects and the hazard of adverse effects
|
Gastrointestinal (GI): -
|
Mechanism Of Action |
Site Of Action |
Adverse Effects |
Uses |
Pharmacokinetics |
Pharmacodyanmics |
|
Daunorubicin works primarily by intercalating DNA strands and inhibiting the enzyme topoisomerase II this action prevents DNA replication and transcription, leading to apoptosis of quickly dividing cells, like as cancer cells. |
The site of action for daunorubicin is within the cell nucleus, where it intercalates into DNA and inhibits topoisomerase II, yet breaking the DNA structure and function in gastrointestinal.
|
Nausea and spewing diarrhoea mucositis (inflammation of the mucous membrane) Anorexia (loss of appetite)
|
AML and ALL it’s now used in combination with other chemotherapeutic agents, particularly in cases of relapse or refractory disorder
|
ADMINISTRATION: - Daunorubicin is commonly administered intravenously DISTRIBUTION: - it has a large volume of distribution, indicating deep tissue belt. It penetrates well into varied tissues, including the kidney, liver and spleen. METABOLISM: - daunorubicin is metabolized primarily in the liver by reduction and oxidative to active and inactive metabolites. EXCRETION: - the medicament and its metabolites are excreted through both the biliary system (faces) and the kidneys (urine) |
the pharmacodynamics of daunorubicin involve its band to DNA and inhibition of topoisomerase II, which are critical for DNA replication and condition. The medicament’s effectiveness is largely medication dependent, with improved medications building up the probability of both healing effects and venom.
|
Reproductive System: -
In Females: -
|
Mechanism Of Action |
Site Of Action |
Uses |
Adverse Effects |
Pharmcokinetics |
Pharmacodynamics |
|
daunorubicin is an anthracycline antibiotic commonly used in chemotherapy for treating various types of cancer, including leukemia. It’s primary mode of action, involves intercalation into DNA, which inhibits the synthesis of nucleic acids and prevents cell division.
|
female reproductive system daunorubicin’s primary target is the rapidly dividing cancer cells. However, it can also affect healthy rapidly dividing cells, including those in the female reproductive system.
|
targeting leukemia infiltration: - in cases where leukemia has infiltrated the reproductive organs daunorubicin, through its systemic action, can help eliminate leukemic cells within these tissues. Since leukaemia is a systemic disease drugs like daunorubicin are effective in targeting cancer cells throughout the body including the reproductive organs
|
Ovarian dysfunction: - Daunorubicin can cause damage to the ovaries, leading to menstrual irregularities, amenorrhea (absence of menstruation) and premature ovarian failure. Infertility: - Due to its cytotoxic effects on ovarian tissue, daunorubicin can result in temporary or permanent infertility. Teratogenicity: daunorubicin is teratogenic, meaning it can cause congenital abnormalities if administered during pregnancy. Secondary malignancies: there is a risk of developing secondary cancers, including those of the reproductive organs, due to the mutagenic properties of daunorubicin. |
ABSORPTION: - Daunorubicin is typically administered intravenously DISTRIBUTION: - it has a wide distribution in body tissues, including the bone marrow, liver and spleen. It can also cross the placenta. METABOLISM: - Daunorubicin is metabolized primarily in the liver to active and inactive metabolites. EXCRETION: - the drug and it’s metabolites are excreted mainly via bile and faeces , with a smaller proportion eliminated through the urine.
|
MECHANISM OF ACTION: - DNA intercalation: Daunorubicin inserts itself between DNA base pairs, disrupting the double helix structure and inhibiting the replication and transcription processes. Topoisomerase II inhibition: Daunorubicin inhibits topoisomerase II, an enzyme crucial for DNA replication and repair, leading to double-strand breaks in the DNA. Generation of free radicals: it includes the formation of free radicals, causing oxidative damage to cellular components, including DNA, proteins and lipids.
|
In Males: -
|
Mechanism Of Action |
Site Of Action |
Uses |
Adverse Effects |
Pharmacokinetics |
Pharmacodynamics |
|
|
Daunorubicin is an anthracycline antibiotic used primarily in cancer chemotherapy. It works by intercalating DNA, thereby inhibiting the synthesis of DNA and RNA. This leads to the inhibition of topoisomerase II, an enzyme involved in DNA replication, which results in DNA strand breakage and apoptosis of cancer cells. |
Daunorubicin targets rapidly dividing cells, including cancer cells. It does not specifically target the male reproductive system but can affect rapidly dividing cells in ant tissue, including those in the male reproductive organs.
|
daunorubicin is used in treatment of AML and ALL leukemia.
|
nausea and vomiting, hair loss, mucositis (inflammation of the mucous membranes) Effects on male reproductive system: - testicular toxicity, potentially leading to reduced fertility or infertility. Reduce sperm count and motility. Gonadal toxicity , which can result in hormone imbalances |
ABSORPTION: - Daunorubicin is typically administered intravenously, ensuring complete bioavailability. DISTRIBUTION: - it is widely distributed throughout the body, with high concentration in the liver, kidneys, and heart. METABOLISM: -Daunorubicin is metabolised primarily in the liver to daunorubicinol, an active metabolite. EXCRETION: - it is excreted mainly via the bile and faeces, with a smaller amount excreted in the urine.
|
Onset of action: Daunorubicin acts rapidly on dividing cells, with effects on cell proliferation noticeable shortly after administration. DURATION OF ACTION: - the cytotoxic effects on cancer cells are prolonged due to its interference with DNA synthesis and cell division. HALF-LIFE: - the plasma half-life of daunorubicin varies, with an initial half-life of about 45 minutes and a terminal half -life of approximately 18.5 hours, reflecting its extensive tissue distribution and prolonged presence in the body
|
|
Table: - 6 Difference Between Daunorubicin and Doxorubicin: -
|
Daunorubicin |
Doxorubicin |
|
Chemical structure: - C22H29NO10 |
Chemical structure: - C27H29NO11 |
|
Structure contains a daunomycinone chromophore and an amino sugar daunosamine. |
Structure also to daunorubicin, but with an added hydroxyl group at the carbon 14 position. |
|
Mechanism of action: -intercalates into DNA, busting the DNA double helix. Inhibits topoisomerase II, precluding DNA replication and carbon. Generates free extremists, leading to cell membrane and DNA damage. |
Mechanism of action: - So to daunorubicin, intercalates into DNA and inhibits topoisomerase II. Generates free crazies, contributing to cytotoxicity. Slightly broader process due to the added hydroxyl group, which may affect its intercourse with cellular fundamentals. |
|
Clinical uses: - primarily used in the treatment of acute myeloid leukaemia (AML). Also used in some cases of acute lymphoblastic leukemia (ALL) |
Clinical uses: - Generally used in a variety of cancers, including breast cancer, lymphoma, bladder cancer and Kaposi’s sarcoma. Hourly a vital factor of combination chemotherapy governances. |
|
Administration: -Administered intravenously. capsule is naturally calculated rested on body skin area. |
Administration: -also administered intravenously. capsule can be accommodated rested on case-specific factors, including body skin area and liver function. |
|
Pharmacokinetics: - Half-life like 18.5 hours. Metabolized in the liver to daunorubicinol, which is less active, excreted altogether via acidity and faeces. |
Pharmacokinetics: -Half -life ranges from 20 to 48 hours, metabolized in the liver to daunorubicinol, which retains some exercise, excreted primarily in the acidity and to a minor extent in urine. |
|
Side effects: - Myelosuppression, cardiotoxicity, gastrointestinal disturbances Alopecia
|
Side effects: - Myelosuppression, cardiotoxicity. Added hazards include severe tissue damage if extravasation occurs. Enhanced constancy of inveterate cardiotoxicity due to incremental capsule. |
|
Cardiotoxicity: - Hazard increase with enhanced accretive medicaments. Operation involves free revolutionist arrangement leading to oxidative damage in cardiac cells. |
Cardiotoxicity: - especially forward hazard of cardiotoxicity compared to daunorubicin. cardiotoxicity may present as congestive heart failure, continually unredeemable. |
|
Effectiveness: -Effective in moving absolution in AML cases. Hourly combined with other agents like cytarabine for better children. |
Effectiveness: - greatly effective in a broad range of cancers hourly used in combination rules like CHOP for lymphoma or FAC for breast cancer. |
|
Resistance: - resistance can develop through increased medicinal efflux, altered medicinal targets, or enhanced DNA form mechanisms. |
Resistance: - resistance mechanisms so to daunorubicin cross- resistance with other anthracyclines is common. |
REFERENCES


CH. Bindusri*, P. Gayatri Devi, Dr. Y. A. Chowdary, Y. V. Veerendranadh, Statistical Study on Daunorubicin, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 1, 742-771. https://doi.org/10.5281/zenodo.14631411
 10.5281/zenodo.14631411
10.5281/zenodo.14631411