
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Shree Venkateshwara College of Paramedical sciences, College of pharmacy.
Thiocolchicoside (TCC) is a semi-synthetic derivative of colchicoside, a natural glucoside obtained from Gloriosa superba. It exhibits strong muscle-relaxant, analgesic, and anti-inflammatory properties, making it effective in treating musculoskeletal, rheumatologic, and neurologic disorders. TCC acts primarily by binding to GABA-A and glycine receptors, promoting inhibitory neurotransmission without causing significant sedation. It is available in oral, injectable, and topical formulations, with a favorable safety profile when used within prescribed limits. Pharmacokinetically, TCC is rapidly absorbed and metabolized to its active form, 3-desmethylthiocolchicine, and mainly excreted through feces. Common side effects include mild gastrointestinal symptoms, dizziness, or skin reactions, with rare cases of hepatotoxicity. Analytical methods such as UV spectroscopy (including derivative and AUC techniques) and high-performance liquid chromatography (HPLC) have been validated for its estimation. Forced degradation studies show TCC is unstable in acidic, alkaline, and oxidative environments but stable under heat and light, indicating method specificity. Therapeutically, TCC is used for conditions like acute lower back pain, neuralgias, and post-traumatic muscle spasms. It is also being studied for potential use in oral submucous fibrosis and bone loss. Its clinical effectiveness and well-established analytical methods support ongoing pharmaceutical applications and further research.
Thiocolchicoside (TCC) is a partially synthetic compound developed from colchicoside, a natural glucoside found in the Gloriosa Superba. It is produced by replacing a methoxy group in colchicoside with a thiomethyl group[1]. Thiocolchicoside (TCC) is commonly used in medical treatment for its muscle-relaxing, pain-relieving, and anti-inflammatory effects[2]. Research has shown that it acts on the central nervous system of rats by interacting with GABA type A receptors (GABAARs) and glycine receptors that are sensitive to strychnine [2]. Thiocolchicoside (THC) chemically, N- [3-(β-D glucopyranoxyloxy)-5,6,7,9-tetrahydro-1,2-imethoxy-10-(methylthio)-9-oxobenzo[a] heptalen-7yl] acetamide [3]. While the compound has been in use since many years in the european countries, the first formulation containing thiocolchicoside was approved in India in the year 2008. Being less sedating than other centrally acting muscle relaxants. Oral, parenteral and topical formulations of thiocolchicoside are available in India. The maximum recommended oral dose is 8 mg every 12 hours for no more than 7 consecutive days. The maximum intramuscular dose should be 4 mg every 12 hours, for up to 5 days [4]. After being taken orally, thiocolchicoside is rapidly absorbed through the digestive system, reaching its highest concentration in the bloodstream in about one hour [5] is used topically for the treatment of muscular spasms and for rheumatologic, orthopaedic and traumatologic disorders [6].
Chemical Structure:
CHEMICAL NAME: N-[(7S)-1,2-dimethoxy-10-methylsulfanyl-9-oxo-3-[(2S,3R,4S,5S,6R)-3,4,5-trihydroxy-6-(hydroxymethyl) oxan-2-yl] oxy-6,7-dihydro-5H-benzo[a]heptalen-7-yl] acetamide
Chemical Formula: C??H??NO??S
Macroscopic Characteristics [2]:
Nature: Crystalline powder
Colour: Pale yellow to yellow
Odour: Characteristic Odour
Taste: Unpleasant taste
Shape: Like that of colchicine with extensive hydrogen bonding determining the crystal structure.
Purity: >95%
Strength: 4mg & 8mg
Foreign matter: Not more than 2%
Total ash : Not more than 4%
Acid- insoluble ash: Not more than 1%
Alcohol-soluble extractive: Not less than 2.5%
Loss on drying: Not less than 60%
Volatile oil: Not less than 0.1%

Fig. 1: Thiocolchicoside API
Fig. 2: Thiocolchicoside Tablet

Solubility [7]:
Mechanism Of Action:
Thiocolchicoside, is a synthetic sulfur derivative of colchicoside, a naturally occurring glucoside contained in the Colchicum autumnale plant. Thiocolchicoside has a selective and potent af?nity for g-aminobutyric acid A (GABA-A) receptors and acts on muscular contractures by activating the GABA inhibitory pathways thereby behaving as a potent muscle relaxant [2]. Gamma-aminobutyric acid (GABA) is the main inhibitory neurotransmitter in the human cortex [8]. GABAergic neurons are involved in myorelaxation, anxiolytic treatment, sedation, and anesthetics. GABA can also modulate heart rate and blood pressure.It also has an affinity for the inhibitory glycine receptors (i.e., have glycomimetic and GABA mimetic activity), therefore acts as a muscle relaxant. Glycine is an inhibitory neurotransmitter and acts as an allosteric regulator of NMDA (N-methyl-D-aspartate) receptors. It is involved in the processing of motor and sensory data, thereby regulating movement, vision, and audition. Inhibitory neurotransmitter in spinal cord, allosteric regulator of NMDA receptors [9]. In one study, thiocolchicoside inhibited the function of recombinant human strychnine-sensitive glycine receptors composed of the alpha1 subunit with a potency (median inhibitory concentration of 47 microM) lower than that apparent with recombinant GABA(A) receptors. The drug also inhibited the function of human nicotinic acetylcholine receptors made of the alpha4 and beta2 subunits, however, this effect was partial and moreover only apparent at high concentrations. Thiocolchicoside demonstrated no effect on the function of 5-HT(3A) serotonin receptors[8].
Pharmacokinetics [10]:
When administered orally, thiocolchicoside reaches its peak concentration in the plasma approximately 50 minutes after ingestion. In contrast, intramuscular (I.M.) administration leads to a quicker peak, occurring around 30 minutes post-injection. During the absorption phase and initial passage through the liver (first-pass metabolism), thiocolchicoside is swiftly converted into its active metabolite, 3-desmethylthiocolchicine. This transformation may also occur partially within the acidic environment of the stomach. Following intramuscular administration, the drug exhibits an apparent volume of distribution of about 42.7 liters, indicating extensive tissue distribution. Studies involving equilibrium dialysis and centrifugation have shown that thiocolchicoside and its metabolites bind to human serum proteins, with a binding affinity of 38.90 C, and to human albumin at a level of 12.80 C ± 5.3%. Thiocolchicoside primarily undergoes metabolism in the intestine facilitated by the enzyme 3-O-glucuronido methylcholine, resulting in the formation of three major metabolites. The drug has a biological half-life of roughly 7.7 hours. Its metabolites are excreted unchanged via both feces and urine, indicating minimal further metabolic transformation. When thiocolchicoside is co-administered with other agents, no chemical interaction or structural alteration occurs, and its pharmacological activity remains unaffected.
Adverse Drug Reaction:
The reported side effects included diarrhea, dizziness, nausea, and skin rashes. All of these were mild and went away on their own without any treatment. Although it is uncommon, thiocolchicoside has the potential to cause liver damage[11]. Allergic reactions like itching, hives, and swelling under the skin; severe allergic shock after a muscle injection; sleepiness; fainting due to a sudden drop in blood pressure, usually happening shortly after the injection; as well as diarrhea, stomach pain, nausea, vomiting, and skin allergies have been reported. Most of these reactions are rare or uncommon. In a large, randomized clinical trial comparing treatments, thiocolchicoside caused more side effects than tolperisone, a muscle relaxant that tends to cause less drowsiness[12]. The impact of thiocolchicoside on psychomotor skills was studied in patients with acute lower back pain and compared to tizanidine. Thiocolchicoside was shown to be at least as effective as tizanidine but without causing any sedation[13]. The main side effects of thiocolchicoside are somnolence (drowsiness), Asthenia(weakness), and fainting or feeling lightheaded due to sudden drop in blood pressure[14].
Route Of Elimination:
Thiocolchicoside is not excreted in its original form, but rather as one of three metabolites, which are primarily eliminated via feces (around 79%) and to a lesser extent in urine (about 20%). The metabolites 3-demethylcolchicine (M2) and 3-O-glucurono-demethylcolchicine (M1) are detected in both urine and feces, while the di-demethylcolchicine metabolite is only present in feces[15] .
Pharmacodynamics:
Thiocolchicoside is a muscle relaxant that works by selectively binding to GABA-A receptors. It helps prevent muscle contractions by activating the inhibitory motor pathway mediated by GABA. This drug functions as a competitive antagonist at GABA receptors and also blocks glycine receptors with similar strength as it does nicotinic acetylcholine receptors. Due to its strong convulsant effects, it should be avoided in people who have a risk of seizures. Thiocolchicoside is used alongside glafenine and meprobamate to calm patients during hysterosalpingography. It is effective in treating painful muscle spasms caused by central nervous system issues, reflex-type contractures, as well as rheumatic and traumatic conditions. Additionally, it helps reduce symptoms related to spasticity following hemiparesis, Parkinson’s disease, and drug-induced Parkinsonism, especially neurodyslectic syndrome. Other conditions that may benefit from this medication include both acute and chronic lower back and sciatic pain, cervico-brachial neuralgia, persistent torticollis, and pain after trauma or surgery[2].
Penetration And Distribution Through Skin:
The percutaneous absorption and distribution profile of thiocolchicoside from a commercially available foam formulation (0.25% w/v) was investigated across human excised full-thickness skin using two distinct in vitro diffusion systems: the Franz diffusion cell and a Saarbruecken model-based diffusion cell. To assess the intrinsic permeation capacity of thiocolchicoside, an aqueous solution of the drug at an equivalent concentration was also evaluated. Results demonstrated that both experimental models were appropriate for characterizing thiocolchicoside skin penetration. Comparable levels of drug permeation were observed between the two systems, likely attributable to the reservoir (sink) behavior of the skin. Importantly, the foam formulation significantly enhanced thiocolchicoside accumulation within the full-thickness skin compared to the aqueous control. This enhancement is primarily associated with the presence of propylene glycol and propylene glycol diperlargonate in the foam vehicle, which act as effective permeation enhancers, facilitating deeper and more efficient dermal delivery of thiocolchicoside[16].
Therapeutic Uses:
Analytical Development Methods:
a) For zero order derivative method:
Stock solutions were prepared by transferring measured volumes into individual 10?mL volumetric flasks, followed by dilution to the mark with 0.1?N NaOH to obtain final concentrations ranging from 2.5 to 50.0?µg/mL. These solutions were then scanned in the wavelength range of 400?nm to 200?nm using a blank as reference. The maximum absorbance (λmax) was observed at 259.0?nm and 374.0?nm[3].
b) For first order derivative method:
To determine the appropriate analytical wavelength for the estimation of thiocolchicoside, a standard solution was prepared by dissolving the drug in methanol to obtain a final concentration of 100 µg/mL. This solution was then subjected to a UV spectrophotometric scan using a UV-Visible spectrophotometer in the spectrum mode, covering the wavelength range of 200 nm to 350 nm. Methanol was used as the blank to eliminate solvent interference during the measurement. The obtained zero-order UV absorption spectrum was then processed using UV Probe software version 2.42 to convert it into the first-order derivative spectrum. The derivative mode enhances the resolution of overlapping peaks and improves selectivity in the quantitative analysis. Upon analysis of the first-order derivative spectrum, a well-defined peak with significant amplitude was observed at 251.8 nm. This wavelength was selected as the analytical wavelength for further quantitative studies, as it provided optimal sensitivity and reproducibility for the estimation of thiocolchicoside [23].
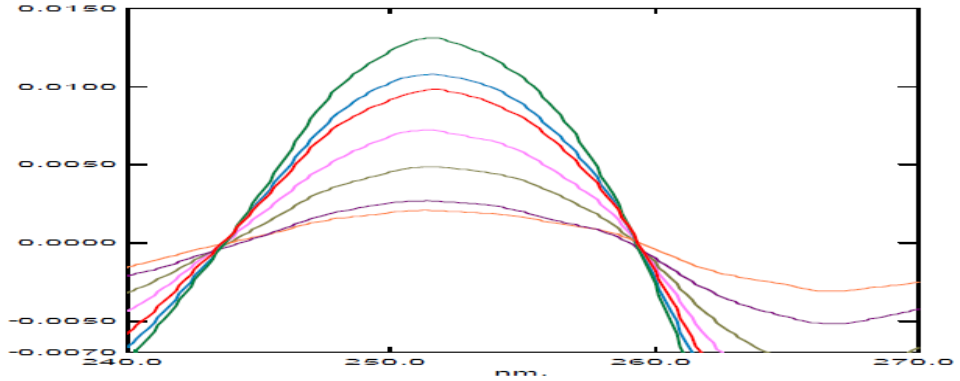
Fig. 4(a): Overlay spectra of first order derivative of thiocolchicoside in the concentration range of 2 and 14 μg/ ml at 251.8 nm[23]
c) For second order derivative method:
To select an appropriate analytical wavelength for the estimation of thiocolchicoside, a standard solution with a concentration of 100 μg/ml was prepared using methanol as the solvent. This solution was then subjected to UV spectrophotometric scanning in spectrum mode over a wavelength range of 350 nm to 200 nm, with methanol used as the blank for baseline correction. The obtained zero-order spectrum was further processed using the UV Probe 2.42 software to generate its first-order derivative spectrum. Subsequently, the second derivative of the spectrum was derived to enhance the resolution and eliminate background noise. From this second derivative spectrum, the amplitude was measured at 224 nm, which was identified as a suitable analytical wavelength for further analysis based on its distinct and reproducible response[23].
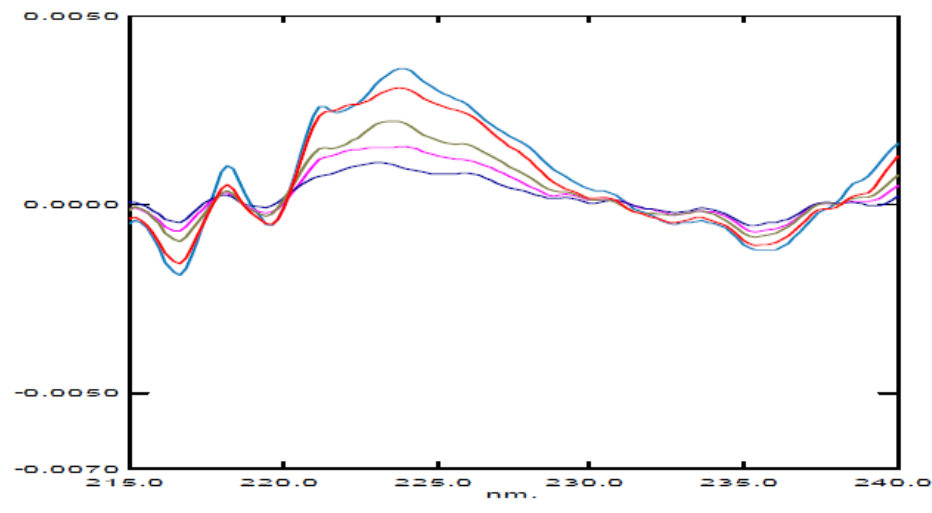
Fig.(4b): Overlay spectra of second order derivative of thiocolchicoside in the concentration range of 2 and 14 μg/ ml at 224 nm [23]
Area Under Curve Method:
The Area Under the Curve (AUC) method is particularly useful when the spectrum lacks a distinct peak or displays broad absorbance bands. This technique involves determining the total absorbance across a specific wavelength range, defined by two selected wavelengths, λ1 and λ2. The area is computed as the region under the absorbance curve and above the baseline (horizontal axis) within this defined range. The wavelength interval for this calculation is chosen based on repeated trials to ensure a linear relationship between the AUC and the analyte concentration. Using the obtained spectra, the AUC values were determined, and a calibration curve was then plotted by graphing concentration against the corresponding AUC values [3].
2) HPLC Method:
A simple and accurate HPLC method was developed and tested to measure the amount of thiocolchicoside in capsule form. The test was done using a special type of column called Thermo Hypersil Silica (250 mm × 4.6 mm, with 5-micron particles). A mixture of four liquids—n-heptane, methanol, chloroform, and acetic acid (in the ratio 70:20:10:0.2)—was used as the mobile phase to carry the drug through the column. The flow of this liquid was set at 1 ml per minute, and the drug was detected using a UV light detector at a wavelength of 360 nm. Thiocolchicoside showed a clear peak at around 7.787 minutes. The method was carefully tested for different qualities like accuracy, precision, sensitivity, and reliability. The method showed a straight-line relationship of 5 to 15 µg/ml, with a high correlation (r² > 0.99). The smallest amount that could be detected (LOD) was 0.15 µg/ml, and the smallest amount that could be measured accurately (LOQ) was 0.46 µg/ml, showing that the method is sensitive. Accuracy was checked by adding known amounts of the drug at 80%, 100%, and 120% levels, and the recovery was between 98% and 102%, which is very good. The method also showed good precision, as the variation between results (%RSD) was less than 2% when tested on the same day and on different days. Even when small changes were made to the method, the results remained consistent, proving that it is robust. Overall, this HPLC method is simple, reliable, and suitable for regular testing of thiocolchicoside in capsules[24].
Standard Chromatograms of Thiocolchicoside:

(Fig. 5a): Blank chromatogram [24]
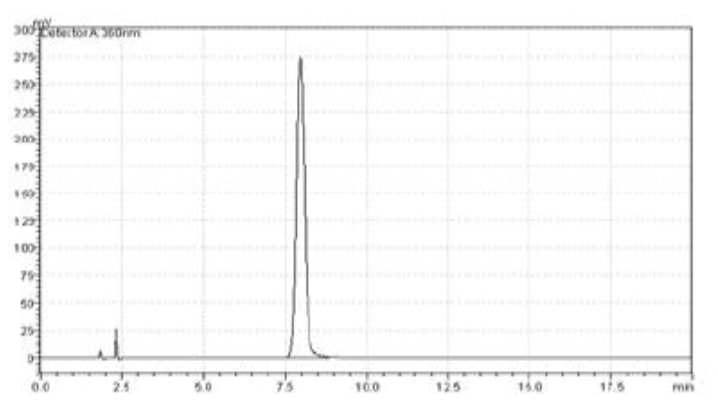
(Fig. 5b): Chromatogram for drug sample [24]
Forced Degradation of Thiocolchicoside [25]:
A precisely weighed 10 mg of thiocolchicoside was separately dissolved in methanolic solutions of 1.0 M HCl and 0.5 M NaOH. Both solutions were refluxed at 60°C for 30 minutes in the dark to prevent light-induced degradation. After cooling, 1.0 mL of each was taken, neutralized, and diluted to 10 mL with methanol. These were applied onto RP-HPTLC plates in triplicate (5 µL per spot, 500 ng per band). Under acid hydrolysis, thiocolchicoside showed degradation with two additional peaks at Rf 0.33 and 0.71(Fig.6a). In alkaline hydrolysis, one extra peak appeared at Rf 0.72, while the main drug peak was at Rf 0.60 (Fig.6b). All degradation spots were well separated from the drug spot.
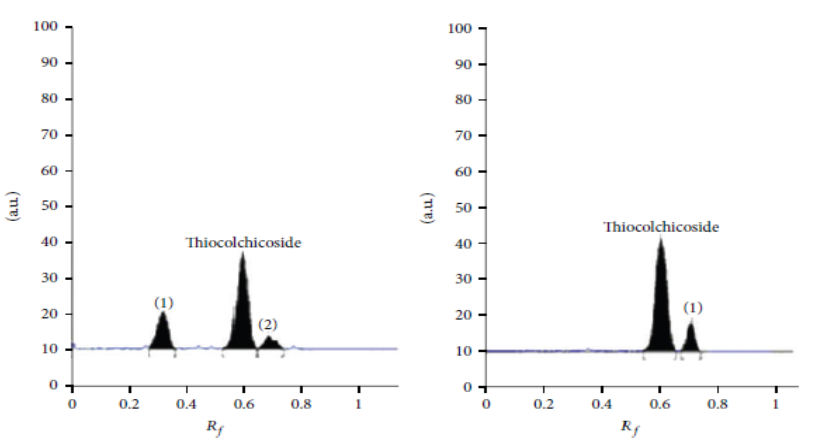
(Fig.6a) Acidic hydrolysis (1M HCl) [25] (Fig.6b) Alkaline hydrolysis (0.5M NaOH) [25]
Oxidative Degradation:
For oxidative degradation, 10 mg of thiocolchicoside was accurately weighed and dissolved separately in 10 mL of methanolic solutions containing 1% v/v and 3% v/v hydrogen peroxide (H2O2). These solutions were kept in the dark at room temperature for 30 minutes. After this period, 1.0 mL from each solution was taken and diluted to 10 mL with methanol. The resulting solutions were applied on RP-HPTLC plates in triplicate (5 µL per spot, 500 ng per band), and chromatograms were developed and scanned. Due to the presence of a sulfur atom in thiocolchicoside, it is more prone to oxidation. After treatment with 1% H, three H2O2 additional peaks appeared at Rf 0.38, 0.46, and 0.70, while the drug remained at Rf 0.60 (Fig.6c). With 3% H2O2, the drug underwent complete degradation, forming two major peaks at Rf 0.58, 0.64, and Rf 0.70 (Fig.6d). Peak purity spectra of thiocolchicoside after degradation in 1M HCl, 0.5M NaOH, and 1% H2O2 showed that the method is specific, with clear separation between the parent drug and its degradation products. Additionally, no degradation was observed when the drug was exposed to sunlight or heat, indicating its stability under photo and thermal conditions.

(Fig.6c) oxidative stress (1% v/v H2O2) [25] (Fig.6d) oxidative stress (3% v/v H2O2) [25]
Dry Heat Degradation:
A precisely weighed 10 mg of thiocolchicoside was kept in an oven at 70°C for 8 hours. After heating, it was transferred to a 10 mL volumetric flask containing methanol, and the volume was adjusted to the mark. From this solution, 1.0 mL was taken and further diluted to 10 mL with methanol. The final solution was then applied onto an RP-HPTLC plate in triplicate (5 µL per spot, equal to 500 ng per band).
A precisely weighed 10 mg of thiocolchicoside was dissolved in 10 mL of methanol and the solution was exposed to light for 24 hours. After the exposure period, 1.0 mL of this solution was taken and diluted to 10 mL with methanol. The final solution was applied in triplicate onto an RP-HPTLC plate (5 µL per spot, equivalent to 500 ng per band).
(Table: 1) Forced degradation studies [25]

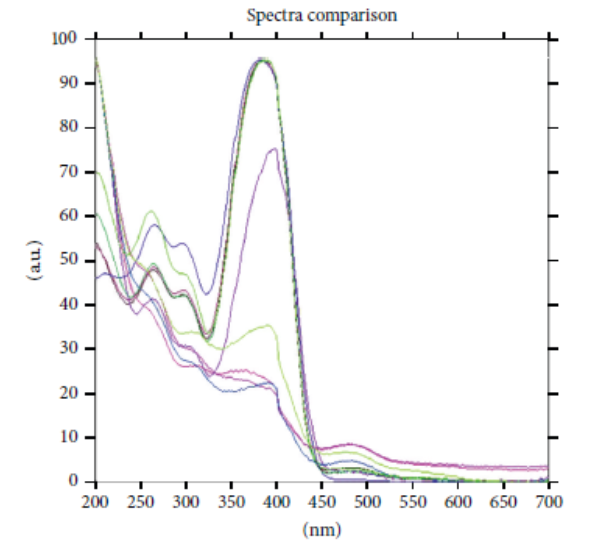
(Fig.7) Peak-purity spectra of thiocolchicoside recovered after degradation in 1M HCl, 0.5M NaOH, 1%v/v H2O2, degradants and thiocolchicoside standard scanned at peak-start, peak-apex and peak-end positions [25]
CONCLUSION:
Thiocolchicoside (TCC) is a semi-synthetic muscle relaxant with strong analgesic and anti-inflammatory effects. It works by selectively binding to GABA-A and glycine receptors, offering relief from muscle spasms with minimal sedation. TCC shows good absorption and tissue distribution but may cause mild side effects in some cases. Validated analytical methods like UV spectroscopy and HPLC have been successfully used to estimate TCC accurately. Forced degradation studies show TCC is unstable in acidic, alkaline, and oxidative conditions but stable under light and heat. These findings confirm the specificity and reliability of the analytical methods. In conclusion, TCC is a clinically valuable drug with proven therapeutic benefits and a strong analytical profile, supporting its continued use and further research in pharmacotherapy.
REFERENCES

K. S. S. Chakravarthi*, K. B. Ilango, E. D. Ananya, D. Dinesh, A. Karthikeyan, P. Suwathi, R. Rathi, Thiocolchicoside: A Brief Review, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 2239-2251 https://doi.org/10.5281/zenodo.17165632
 10.5281/zenodo.17165632
10.5281/zenodo.17165632