
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmaceutical Chemistry, Kamla Nehru College of Pharmacy, Butibori, Nagpur-441108, Maharashtra, India
Tolbutamide was the earliest and most widely adopted oral sulfonylurea introduced in the 1950s for managing type 2 diabetes mellitus (T2DM). Over the past seventy years, its therapeutic value, safety considerations, and overall position in diabetes treatment have been reassessed as newer medications became available. This review explores the chemical characteristics and pharmacological actions of tolbutamide, its mechanism of action, key historical studies such as the University Group Diabetes Program (UGDP), concerns related to hypoglycaemia and potential cardiovascular effects, as well as its pharmacokinetic behaviour and metabolic pathways. The evolution of its clinical use is also discussed to highlight its relevance in contemporary diabetes management. By integrating both classic and modern literature, the review evaluates tolbutamide’s contribution to current therapeutic practices. Although concerns especially regarding hypoglycaemia and early indications of cardiovascular risk led to declining use and stricter regulatory oversight, the drug served as a foundation for oral antidiabetic therapy. As newer sulfonylureas with improved profiles and alternative drug classes became available, tolbutamide was gradually replaced in many healthcare settings. Despite this decline, its role in shaping the history and development of diabetes pharmacotherapy remains substantial.
Over 400 million people worldwide suffer from diabetes mellitus (DM), a serious public health concern. Chronic microvascular, macrovascular, and neuropathic consequences that are potentially fatal are gradually brought on by this metabolic condition. DM is brought on by either insufficient insulin secretion, injury to the pancreatic β cell, or insulin resistance by not using insulin. Sedentary lifestyles may be the main cause of the ongoing increase in the number of diabetic patients worldwide, which is predicted to reach 366 million in the older population (those over 65) by 2030. Nephropathy, neuropathy, cardiovascular and renal problems, retinopathy, food-related issues, and more are among the many complications linked to diabetes mellitus. There are two forms of diabetes: type 1 and type 2. Type 2 diabetes is caused by damage to pancreatic beta cells, which makes it more difficult for a person to use insulin, whereas type 1 diabetes is an autoimmune disease that affects pancreatic cells, reducing or impairing the generation of insulin.[1]
Non-insulin-dependent diabetes mellitus (NIDDM) is treated with tolbutamide, an oral antihyperglycemic medication. It is a member of the sulfonylurea class of insulin secretagogues, which work by inducing the release of insulin from the pancreatic β cells. It shares structural similarities with acetohexamide, chlorpropamide, and tolazamide. Both basal insulin secretion and meal-stimulated insulin release are increased by sulfonylureas. The dosage, rate of absorption, duration of action, route of excretion, and binding location on the target pancreatic β cell receptor of medications in this class vary. Additionally, sulfonylureas reduce hepatic gluconeogenesis, boost peripheral glucose consumption, and perhaps increase the quantity and sensitivity of insulin receptors. Although not as much as insulin, sulfonylureas are linked to weight gain. Sulfonylureas may result in hypoglycemia due to their mode of action, hence regular food consumption is necessary to reduce this risk. Elderly, disabled, and malnourished people are more likely to have hypoglycemia. It seems that the liver is where tolbutamide is processed. Urine (75–85%) and feces contain tolbutamide and its metabolites.[2]
By attaching to receptors that inhibit potassium ATP-dependent channels, sulfonylureas cause cell depolarization and insulin exocytosis, which in turn triggers the release of insulin from pancreatic β-cells. Ruiz and associates discovered that synthesized sulfur compounds had hypoglycemic properties in 1937. A French doctor named Janbon and his associates verified hypoglycemia in patients receiving p-amino-sulfonamide-isopropyl-thiodiazole for typhoid in 1942. In August 1946, Lobatieres and associates discovered that this class of medications increased the release of insulin from β-cells. The first sulfonylurea, tolbutamide, was commercialized in Germany in 1956. The first-generation sulfonylureas, chlorpropamide, acetohexamide, and tolazamide, came next. The more powerful second-generation sulfonylureas glyburide and glipizide were made available in the US in 1984, more than 14 years after they were first introduced in Europe. The third-generation sulfonylurea glimepiride was first made available in the US in 1995. There is a 1-2% drop in the HbA1C (A1C). For over 50 years, sulfonylureas have been available on the market. Although they are dependable, inexpensive, and safe, their usage is restricted by the serious adverse effect of hypoglycemia.[3]
Table No.1: Evolution of Tolbutamide and Sulfonylureas in the Management of Diabetes Mellitus (1955–2025)
|
Sr. No. |
Year |
Event |
Note |
|
1. |
1955 |
Discovery of Tolbutamide (first-generation sulfonylurea) |
Introduced by Hoechst AG; first oral hypoglycemic drug. |
|
2. |
1959-1960 |
Tolbutamide approved for clinical use |
Revolutionized non-insulin therapy in type 2 diabetes. |
|
3. |
1961-1971 |
UGDP Trial |
Evaluated cardiovascular safety; controversy over increased CV mortality. |
|
4. |
1979 |
Second-generation sulfonylureas introduced (glibenclamide, glipizide) |
Improved potency and fewer side effects. |
|
5. |
1998 |
UKPDS results |
Confirmed glycemic benefit of sulfonylureas in long-term outcomes. |
|
6. |
2000-2010 |
Comparative safety re-evaluations |
Tolbutamide largely replaced by modern agents. |
|
7. |
2018 |
Reappraisal of sulfonylurea safety |
Re-established clinical utility in select patients. |
|
8. |
2020-2025 |
Repurposing studies for Tolbutamide |
Investigated for anticancer, anti-inflammatory, and neuroprotective roles. |
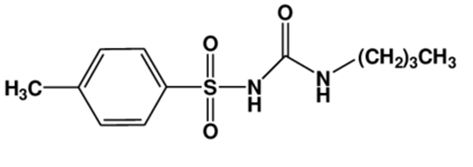
IUPAC Name :- 1-butyl-3-(4-methylphenyl)sulfonylurea
Molecular Formula :- C12H18N2O3S
Molecular Weight :- 270.35 g/mol
Melting Point :- 126-130 ͦ C
Organoleptic Properties :-
Colour :- White crystalline powder
Odour :- Odourless
Taste :- Slightly bitter
Solubility :- It is sparingly soluble in water, freely soluble in alcohol and acetone and
insoluble in ether.[4]
• Tolbutamide attaches itself to the sulfonylurea receptor 1 (SUR1), a regulatory subunit of
the pancreatic β-cells' ATP-sensitive potassium (K ATP) channel.[5]
• Tolbutamide reduces potassium (K +) efflux by blocking the K ATP channel when it binds
to SUR1.[7]
• Because K + can no longer exit as readily, this impact causes the β-cell membrane to
depolarize.[7]
• Voltage-gated Ca 2+ channels open as a result of membrane depolarization, allowing Ca
2+ to enter the β-cell.[8]
• An increase in intracellular Ca 2+ promotes insulin-containing granule exocytosis, which
raises insulin production.[7]
• According to some research, tolbutamide may also improve insulin exocytosis through
pathways connected to protein kinase C (PKC), independent of merely raising Ca 2+.[9]
• Tolbutamide has a substantially lower affinity for channels with other SUR subtypes, such
as SUR2A in cardiac tissue, and predominantly impacts KATP channels with SUR1 (found
on β-cells).
Table No. 2: Pharmacokinetic Parameters of Tolbutamide and Representative Sulfonylureas
|
Sr No. |
Parameter |
Tolbutamide (1st Gen) |
Glibenclamide (2nd Gen) |
Gliclazide (2nd Gen) |
Glimepiride (3rd Gen) |
|
1. |
Molecular Weight (g/mol) |
270.35 |
494.00 |
323.40 |
490.62 |
|
2. |
Bioavailability (%) |
~95 |
50-60 |
~100 |
~100 |
|
3. |
t₁/₂ (Half-life) |
4-8 h |
10 h |
8-12 h |
5-9 h |
|
4. |
Protein Binding (%) |
96-99 |
99 |
85-95 |
99 |
|
5. |
Metabolism |
Hepatic (CYP2C9) |
Hepatic (CYP3A4,2C9) |
Hepatic |
Hepatic |
|
6. |
Excretion |
Renal (~80%) |
Biliary +Renal |
Renal |
Renal |
|
7. |
Onset of Action |
30-60 min |
60 min |
60 min |
60-90 min |
|
8. |
Duration of Action |
6-12 h |
18-24 h |
16-24 h |
24 h |
|
9. |
Dose Range (mg/day) |
250-2000 |
2.5-15 |
40-320 |
1-8 |
|
10. |
Adverse Effects |
Hypoglycemia (less severe), rash, GI upset |
Hypoglycemia, weight gain |
Mild hypoglycemia |
Low hypoglycemia risk |
4.1. Early efficacy trials and clinical adoption
Tolbutamide was quickly adopted in the late 1950s and early 1960s after early clinical studies and short-term trials showed consistent glucose decrease and symptom relief. Its clinical zeal and commercial dissemination are documented in historical chronicles. [3]
4.2. University Group Diabetes Program (UGDP) — a turning point
Commencing in 1961, the UGDP was one of the first large-scale randomized studies intended to determine whether decreasing blood sugar with particular medications decreased vascular problems. Concerns over the cardiovascular safety of sulfonylureas were raised in 1970 when the UGDP team reported an unexpected rise in cardiovascular mortality among patients allocated to tolbutamide versus diet alone. This led to controversy and the early withdrawal of tolbutamide from that trial arm. The UGDP findings had a lasting impact on clinical and regulatory thinking regarding oral hypoglycemic safety, but they also sparked a great deal of methodological discussion and follow-up analyses.[11]
4.3. Later large trials and meta-analyses (UKPDS and beyond)
Subsequent long-term trials, such as the UK Prospective Diabetes Study (UKPDS) and meta-analyses, made it clear that strict glycaemic control lowers microvascular outcomes and that the relative cardiovascular risk differences between agents are subtle. However, when confounding and variations in study design were taken into account, many analyses failed to confirm a significant class-wide excess mortality attributable to sulfonylureas. However, direct comparisons between tolbutamide and later medications are complicated by agent and trial era heterogeneity. [12]
Occasionally, tolbutamide caused severe and extended hypoglycemia; case reports from the 1960s showed fatal or prolonged episodes, particularly in older patients or those with impaired drug clearance. The greatest safety concern with sulfonylureas is still hypoglycemia risk, which was a major factor in both clinical caution and the subsequent preference for drugs with lower hypoglycemia risk.[13]
Results from the UGDP era indicated that tolbutamide was associated with a higher risk of cardiovascular death; later re-analyses and trials yielded conflicting results. The results of contemporary systematic reviews and observational studies have been inconsistent. While some analyses indicate a slight increase in specific cardiovascular endpoints with older sulfonylureas or in combination with metformin, other large contemporary datasets and meta-analyses do not consistently demonstrate a class-wide increase in all-cause mortality. According to the general interpretation, cardiovascular risk is influenced by the agent, patient group, glycaemic management, and research design; hence, where appropriate, doctors should prioritize medicines with positive cardiovascular outcome data.[14]
The side effects of first-generation sulfonylureas, such as weight gain, possible SIADH with long-acting congeners, and infrequent hypersensitivity, are typical of tolbutamide. Patients at high risk of hypoglycemia, the elderly, and those with liver disease should not use it. Current clinical resources include advice for dosage, contraindications, and monitoring.[7]
The use of tolbutamide decreased over time due to safety concerns, the introduction of longer-acting or more β-cell-specific sulfonylureas (such as glimepiride and gliclazide), and later the introduction of metformin, DPP-4 inhibitors, SGLT2 inhibitors, and GLP-1 receptor agonists with varying safety and efficacy profiles and demonstrated cardiovascular and renal benefits in recent outcome trials. In many areas, guidelines recommended metformin as the first-line treatment; sulfonylureas, which are often later-generation drugs, were still an option when newer drugs were too expensive or difficult to obtain or when strong glucose lowering was needed.[15]
The UGDP experiment and ensuing disputes influenced labeling, regulatory advice, and the design of future outcome trials. The history of tolbutamide inspired the big cardiovascular outcome trial paradigm needed for many new antidiabetic drug approvals, as well as a more cautious approach to long-term safety surveillance for glucose-lowering drugs.[11]
The journey of tolbutamide from widespread use to its current decline teaches us numerous things:
Table No. 3:- Clinical Legacy and Emerging Repurposing Roles of Tolbutamide
|
Sr. No. |
Domain |
Key Findings/ Applications |
Proposed Mechanism of Action |
|
1. |
Classical Antidiabetic Use |
First‐generation sulfonylurea used for T2DM; effective glucose lowering but shorter duration of action. |
Closure of pancreatic KATP channels via SUR1 → depolarization → Ca²⁺ influx → insulin release.[17] |
|
2. |
Comparative Safety Evaluation |
UGDP raised early concerns over cardiovascular mortality; later trials found neutral CV outcomes. |
No direct cardiotoxicity; effects linked to hypoglycemia and insulin levels. |
|
3. |
Metabolic Benefits Beyond Glucose Control |
Possible improvement in microvascular outcomes with long-term glycemic control. |
Reduced oxidative stress from improved β-cell function. |
|
4. |
Anti-Inflammatory Activity |
Reduces TNF-α and IL-6 production in activated macrophages; modulates NF-κB pathway. |
Suppression of inflammatory cytokine gene expression via KATP-independent pathways. |
|
5. |
Anticancer Potential |
Demonstrates cytotoxicity in colon, breast, and liver cancer cell lines; induces apoptosis and inhibits glycolysis. |
Inhibits SUR1 expression, disrupts mitochondrial membrane potential, enhances AMPK activation. |
|
6. |
Neuroprotective Effects |
Shown to protect neurons in ischemic injury and Alzheimer’s models. |
Modulation of KATP channels in neurons; reduced excitotoxicity and oxidative stress. |
|
7. |
Cardioprotection |
At low doses, improves cardiac preconditioning and post-ischemic recovery. |
Controlled opening of cardiac mitochondrial KATP channels. |
|
8. |
Anti-Microbial/Adjunctive Therapy |
Synergistic effect with β-lactam antibiotics against Staphylococcus aureus. |
Interference with bacterial energy metabolism. |
|
9. |
Future Directions |
Drug repurposing for metabolic-inflammatory-neurodegenerative axis; potential repositioning as a KATP modulator scaffold. |
Structure–activity optimization for multi-target effects. |
CONCLUSIONS
The first effective oral medication for type 2 diabetes was tolbutamide, which was crucial in the early development of diabetic medications. It helps the body release more insulin by blocking the pancreatic KATP channels. Early research demonstrated that it might effectively drop blood sugar, but subsequent studies particularly the UGDP study raised questions about potential hazards associated to the heart. This led to more stringent safety testing for all diabetes medications and increased caution among medical professionals and researchers. New medications that are safer, more effective, and less likely to result in hypoglycemia have gradually replaced tolbutamide. Tolbutamide is still significant in medical history even though it is no longer widely used. It affected the development of current diabetic treatments and assisted scientists in understanding how insulin-releasing medications function. Additionally, research indicates that it may have potential applications outside of diabetes, such as anti-inflammatory or anticancer benefits. Overall, the tale of tolbutamide demonstrates the importance of both long-term safety and efficacy in the treatment of diabetes.
REFERENCES

Ankit Borkar, Pranali Darro, Lokesh Thote, Jagdish Baheti, Exploring Of Tolbutamide in The Treatment of Diabetes Mellitus, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 5, 7722-7729, https://doi.org/10.5281/zenodo.20430575
 10.5281/zenodo.20430575
10.5281/zenodo.20430575