Department of pharmacology Vidyabharti college of pharmacy Amravati Maharashtra India
Hyperlipidemia is characterized by unusually high levels of lipids and/or lipoproteins in the bloodstream. It can be categorized into two main types: familial hyperlipidemia and acquired hyperlipidemia. Additionally, hyperlipidemia can be influenced by both modifiable and non-modifiable risk factors. Effective management of this condition necessitates a collaborative approach involving medical professionals, nutritional experts, and lifestyle changes. The primary sources of information for this review included online research via the Google search engine and various books. This review aims to provide an overview of hyperlipidemia, including its risk factors and management strategies. Adiposopathy can result from an unhealthy diet and a sedentary lifestyle, particularly in individuals who are genetically or environmentally predisposed. Management approaches are tailored to the specific lipid abnormalities present. Numerous countries and regions have established their own guidelines for dyslipidemia. The prevention and treatment of dyslipidemia involve assessment, setting treatment goals, increasing physical activity, dietary changes, medical interventions, follow-up evaluations, reassessments, and adjustments to the treatment plan as needed.
Hyperlipidemia is characterized by unusually high levels of lipids and/or lipoproteins in the bloodstream. It can be categorized into two main types: familial hyperlipidemia and acquired hyperlipidemia. Additionally, hyperlipidemia can be influenced by both modifiable and non-modifiable risk factors. Effective management of this condition necessitates a collaborative approach involving medical professionals, nutritional experts, and lifestyle changes. The primary sources of information for this review included online research via the Google search engine and various books. This review aims to provide an overview of hyperlipidemia, including its risk factors and management strategies. Adiposopathy can result from an unhealthy diet and a sedentary lifestyle, particularly in individuals who are genetically or environmentally predisposed. Management approaches are tailored to the specific lipid abnormalities present. Numerous countries and regions have established their own guidelines for dyslipidemia. The prevention and treatment of dyslipidemia involve assessment, setting treatment goals, increasing physical activity, dietary changes, medical interventions, follow-up evaluations, reassessments, and adjustments to the treatment plan as needed (1-4). The small intestine plays a crucial role in the absorption of dietary fats, converting them into chylomicrons that are then transported to peripheral tissues through the bloodstream. The enzyme lipoprotein lipase facilitates the breakdown of chylomicrons, allowing fatty acids to be delivered to adipose tissue and muscle. The liver processes the remnants of chylomicrons and initiates the synthesis of very-low-density lipoproteins (VLDLs). High-density lipoprotein (HDL) is synthesized in the liver and is responsible for transporting cholesterol from the body back to the liver, earning it the designation of "good cholesterol." (1,3-5).In addition to its role in cholesterol transport, HDL exhibits anti-inflammatory, antioxidant, and antithrombotic properties, making it a cardioprotective molecule. Hyperlipidemia is primarily categorized into two types: primary (familial), which arises from specific genetic defects, and secondary (acquired), which is linked to other underlying health conditions. In some cases, hyperlipidemia may be idiopathic, occurring without a known cause. Furthermore, extensive research has established a significant correlation between elevated lipoprotein(a) [Lp(a)] levels and the incidence of heart disease. Hyperlipidemia is categorized based on the specific types of elevated lipids, including hypercholesterolemia and hypertriglyceridemia. Secondary hyperlipidemia frequently resembles familial hyperlipidemia (2,6) and can produce comparable effects. Both conditions may elevate the risk of early-onset atherosclerosis, and in cases of severe hypertriglyceridemia, they can lead to pancreatitis and other complications associated with chylomicronemia syndrome (7). Addressing the underlying causes, when feasible, or altering the medications responsible for the condition typically leads to an improvement in hyperlipidemia. Hypertriglyceridemia is characterized by elevated levels of triglycerides in the bloodstream. While a certain level of triglycerides is necessary for providing energy, they do not directly contribute to the fatty deposits associated with atherosclerosis (6,8). However, cholesterol particles contained within triglyceride-rich particles known as very low-density lipoproteins (VLDLs) can facilitate plaque formation. Another acquired cause of hyperlipidemia is postprandial hyperlipidemia, which refers to the normal increase in lipid levels that occurs after eating (8,9).
2. MATERIALS AND METHODS
The primary method of data collection involved utilizing the Google search engine. The search focused on keywords such as "risk factor" and "management of dyslipidaemia." This process yielded approximately 88 sources, of which 37 were ultimately selected for use. These 37 articles were deemed pertinent as they addressed the aims and objectives of the review. All selected articles were published in English. The inclusion criteria encompassed studies related to epidemiology, risk factors, pathogenesis, diagnosis, prevention, and management. The timeframe for the study spanned from October 1, 2016, to March 31, 2017.
3. DISCUSSION
3.1 Risk Factors
The mutations in one or more genes lead to excessive production and inadequate clearance of cholesterol, triglycerides (TG), and low-density lipoprotein (LDL). These are referred to as non-modifiable risk factors, also known as primary causes. Primary disorders are prevalent causes of dyslipidemia in children, although they may not significantly impact most cases of dyslipidemia in adults.
I. Non-modifiable Risk Factors
Age, Gender, and Genetics: While unhealthy lifestyle choices are the primary contributors to hyperlipidemia, it can also be inherited. The risk increases naturally when men reach the age of 45 and women reach 55, due to age-related physiological changes [13,15,17]. As individuals age, the efficiency of the heart muscle declines, which can elevate arterial pressure [18,19]. For women, this increase in risk occurs later, typically after menopause, when cholesterol levels often rise. Post-menopausal women tend to exhibit higher levels of total cholesterol and LDL-C. Apolipoprotein B levels are different in postmenopausal women compared to premenopausal women. Additionally, total HDL levels decline in postmenopausal women. While individuals cannot change their age or genetic predispositions, it is important to note that the condition can still be managed effectively (10,12,20).
Chronic Disease : Chronic illnesses that place additional strain on the cardiovascular system can lead to elevated cholesterol levels. When a test indicates high cholesterol and the cause is not immediately apparent, a physician may investigate potential underlying conditions. These may include kidney disorders, liver diseases, thyroid dysfunctions, pituitary gland abnormalities, and diabetes. In many instances, managing these conditions can result in improved cholesterol levels. Elevated blood sugar levels are associated with increased LDL cholesterol and decreased HDL cholesterol. Additionally, high blood sugar can harm the arterial lining. Other cholestatic liver diseases, including primary biliary cirrhosis, also heighten the risk of dyslipidemia (16,20).
II. Modifiable Risk Factors
Medications: Certain medications, including thiazides, retinoids, estrogens, and glucocorticoids, among others, can elevate the risk of dyslipidemia [10,12,20,21].
Nutrition: An unhealthy diet contributes to an increased risk of hyperlipidemia in two primary ways. Firstly, the composition of the diet plays a significant role; high intake of fats and cholesterol can lead to elevated lipid levels in the bloodstream. Secondly, excessive calorie consumption results in surplus calories being stored as fat in the body [11,17,19]. The National Cholesterol Education Program (NCEP) indicates that weight loss and a nutritious diet can reduce levels of harmful cholesterol stored in the body while increasing levels of beneficial cholesterol that is typically excreted [19,21].
Physical inactivity : Physical inactivity is associated with a decrease in levels of harmful cholesterol and an increase in beneficial cholesterol. A sedentary lifestyle can contribute to weight gain, which is why it is recognized as a risk factor for hyperlipidemia. Additionally, cigarette smoking harms the blood vessel walls, increasing the likelihood of fatty deposits forming. It may also reduce levels of HDL cholesterol. The risk is heightened for men with a waist circumference of 102 cm or more, and for women with a waist circumference of 89 cm or more. Figure 1 illustrates the relationship between these factors.
3.2 Global Risk Assessment
The initial step in preventing dyslipidaemia is to identify risk factors [10,19,22]. It is advisable to conduct more frequent evaluations for individuals with a family history of early-onset coronary artery diseases, particularly those who have experienced a definite myocardial infarction or sudden death before the age of 55 in a father or other male first-degree relative, or before the age of 65 in a mother or other female first-degree relative. Additionally, it is crucial to perform annual screenings for all adult patients with diabetes to check for dyslipidaemia. In the absence of coronary artery diseases, dyslipidaemia screening should occur at least every 1 to 2 years [15,23]. For children over the age of 2, screening is recommended every 3 to 5 years.
3.3 Pathogenesis, Symptoms, and Diagnosis
Fatty acid synthesis begins with acetyl-CoA and involves the sequential addition of two-carbon units. This process takes place in the cytoplasm of cells, whereas fatty acid oxidation occurs within the mitochondria. The primary locations for fatty acid synthesis are the liver and adipose tissue. Hyperlipemia arises when the rate of lipolysis in adipose tissue (dependent on hormone-sensitive lipase and adipose triglyceride lipase) and the subsequent synthesis of hepatic VLDL (which is substrate-dependent and reliant on microsomal triglyceride transfer protein) surpasses the clearance rate of plasma VLDL (which depends on lipoprotein lipase and VLDL receptors). A sedentary lifestyle and an unhealthy diet can exacerbate hyperlipidemia, particularly in individuals who are genetically or environmentally predisposed. Impaired adiposity in subcutaneous and peripheral lipid tissues during a positive caloric balance may lead to an accumulation of lipids in non-adipose organs, such as muscle and the pancreas, resulting in lipotoxicity (13,25,26). The endocrine dysfunction associated with adiposopathy is directly harmful to the cardiovascular system and other bodily functions. Furthermore, adiposopathy indirectly contributes to additional atherosclerotic risk factors, including hypertension and type 2 diabetes mellitus (22,27). Adipose tissue serves as a significant, non-embryonic source of mesenchymal cells, which are relatively easy to access and possess the ability to differentiate into cells of blood vessels and cardiac tissue. This characteristic has important medical implications for cardiovascular diseases, including regenerative medicine, cell replacement therapies, and tissue engineering, offering potential therapeutic strategies for repairing post-infarcted hearts or ischemic tissues (22,23). Patients with dyslipidemia may remain asymptomatic for many years before exhibiting physical signs of hyperlipidemia. These signs can include tuberous xanthomas located in the Achilles tendon, hands, feet, elbows, and/or knees, as well as corneal arcus in the eyes. Symptoms associated with dyslipidemia may encompass dyspnea, paresthesia, and confusion. Although dyslipidemia itself may not present any symptoms, it can lead to other symptomatic vascular diseases, such as coronary artery disease (10,24,25).
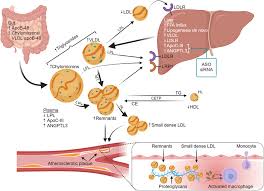
Fig 1. Causes of hyperlipidemia (15, 17)
The primary objective in managing dyslipidaemia is to prevent atherosclerotic coronary diseases, which encompass conditions such as stroke, acute coronary syndromes, transient ischemic attacks, and peripheral arterial disorders (26). Treatment approaches are tailored to the specific lipid abnormalities present, although it is common for multiple lipid issues to occur simultaneously. A single lipid abnormality may necessitate various interventions, while in some cases, a single treatment may suffice for multiple lipid disorders (13.25,28). Effective management should always incorporate smoking cessation, as well as the treatment of diabetes and hypertension (10,24,25,29-31). For high LDL cholesterol, management strategies include lifestyle changes (such as exercise and dietary adjustments), medications, dietary supplements, experimental therapies, and procedural interventions (10,14,25). These strategies are also applicable to other lipid abnormalities. Dietary changes should focus on reducing saturated fats and cholesterol intake, increasing dietary fiber consumption, and achieving and maintaining a healthy body weight (6,21,29). Referrals to dietitians can be particularly beneficial, especially for elderly patients. Regular physical activity can aid in weight management and may help lower LDL cholesterol levels in certain individuals. While dietary changes and exercise should be encouraged whenever possible, the use of medications may be warranted for specific patient groups after a thorough discussion of the associated risks and benefits (10,24,25). The American Heart Association recommends statin therapy for four patient categories: individuals with any form of clinical coronary artery disease, those with LDL cholesterol levels of 190 mg/dL or higher, patients aged 40 to 75 with diabetes and LDL cholesterol levels between 70 and 189 mg/dL, and individuals aged 40 to 75 with LDL cholesterol levels between 70 and 189 mg/dL who have a 10-year risk of coronary artery disease of 7.5% or greater (1,14,15). The management of dyslipidaemia in children remains a contentious issue; implementing dietary modifications can be challenging, and current research does not conclusively demonstrate that maintaining low lipid levels in children effectively reduces the risk of heart disease in adulthood (10,24,33). The primary approach involves implementing lifestyle changes, including increasing physical activity, achieving weight loss, and minimizing the intake of high-alcohol and sugary foods. Consuming two to four servings of omega-3 fatty acid-rich fish weekly may be beneficial; however, supplements might be necessary as dietary sources alone often fall short of meeting the required levels 10,24,25,29,34). For individuals with diabetes, it is crucial to maintain strict control over glucose levels. Those with elevated triglycerides (TGs) may need to initiate medication therapy at the time of diagnosis to swiftly mitigate the risk of acute pancreatitis. Fibrates can lower TG levels by approximately 50% (32). Statins are recommended for patients with TGs below 500 mg/dL, particularly if high levels of LDL cholesterol are also present, as they can effectively reduce both LDL and TGs by lowering very-low-density lipoprotein (VLDL). If only TGs are elevated, fibrates are the preferred treatment option. High doses of eicosapentaenoic acid and docosahexaenoic acid have shown effectiveness in managing hyperlipidemia. Prescription omega-3 fatty acid formulations are advised for triglyceride levels exceeding 500 mg/dL Strategies aimed at reducing TGs and LDL cholesterol often result in an increase in HDL cholesterol, and it is typically possible to achieve all three objectives simultaneously (10,24,35). There are no specific guidelines addressing the management of low HDL cholesterol in children. Treatment strategies include lifestyle changes such as weight loss and increased physical activity. When lifestyle modifications alone are insufficient, medications can effectively raise HDL levels. Niacin (nicotinic acid) is recognized as the most potent medication for enhancing HDL levels, while also lowering LDL cholesterol and decreasing TGs at doses ranging from 1500 to 2000 mg per day. Top of Form
phrase
Bottom of Form
1856 characters · 265 words · ???? Formal · English Prescription omega-3 fatty acid supplements are recommended for individuals with triglyceride levels exceeding 500 mg/dL (33,35). The management of triglycerides (TG) and low-density lipoprotein (LDL) cholesterol often results in an increase in high-density lipoprotein (HDL) cholesterol, and it is typically possible to achieve all three objectives simultaneously. Currently, there are no specific guidelines addressing the management of low HDL cholesterol in children. Treatment strategies include lifestyle changes such as weight reduction and increased physical activity. When lifestyle modifications alone are insufficient, medications may effectively raise HDL levels. Niacin (nicotinic acid) is recognized as the most potent medication for enhancing HDL levels (17,28,36). Additionally, niacin lowers LDL cholesterol and reduces triglycerides at doses ranging from 1500 to 2000 mg per day (10,24,35). For patients with below-average HDL cholesterol and average LDL cholesterol levels, a combination of statins and niacin may be beneficial in preventing cardiovascular diseases. However, niacin does not seem to provide additional benefits for patients already treated with statins to reduce LDL to below 70 mg/dL (32) . Fibrates may help lower cardiovascular risk in patients with triglyceride levels above 200 mg/dL and HDL cholesterol below 40 mg/dL. There is limited research guiding the management of elevated lipoprotein(a) [Lp(a)]. Niacin is the only treatment that directly reduces Lp(a), with the potential to decrease it by up to 20% at higher doses. The standard approach for patients with high Lp(a) is to aggressively lower LDL levels. Management of diabetic dyslipidemia should always include lifestyle modifications along with statins to reduce LDL levels. To reduce the risk of pancreatitis, fibrates can be utilized to lower triglycerides when levels exceed 500 mg/dL.
5. TREATMENT GOALS AND RECOMMENDATIONS
In adults of both sexes, the target for LDL cholesterol should be below 100 mg/dL, and for individuals at very high risk, it should be below 70 mg/dL. For patients with diabetes mellitus, the LDL goal is also set at under 100 mg/dL, while those with additional risk factors, such as cardiovascular diseases, should aim for an LDL level below 70 mg/dL. Another objective is to increase HDL cholesterol levels as much as possible, with a minimum target of above 40 mg/dL for both men and women. However, simply raising HDL levels is not effective on its own. Additionally, it is recommended that the optimal level of apolipoprotein B (apo B) for patients at risk of coronary artery disease or diabetes should be less than 90 mg/dL, while those with established diabetes and coronary conditions should adhere to similar guidelines. ndividuals with artery diseases or one or more additional risk factors should aim for an apo B target of less than 80 mg/dL. It is advisable for both men and women to maintain triglyceride levels below 150 mg/dL. Managing lipid levels should involve a comprehensive approach that addresses modifiable risk factors and metabolic issues such as diabetes, hypertension, obesity, and smoking. The primary strategy for preventing lipid disorders includes lifestyle modifications, which encompass medical nutrition therapy and regular exercise. Treatment may also incorporate patient education initiatives and pharmacotherapy to further reduce risks through weight loss and smoking cessation. Physical activity should consist of at least 30 minutes of moderate-intensity exercise 4 to 6 times a week, aiming for a caloric expenditure of at least 200 kcal per day. Recommended activities include brisk walking, cycling, water aerobics, cleaning, lawn mowing, and various sports. For adults, international guidelines suggest a low-calorie diet rich in vegetables and fruits (at least 5 servings per day), grains (at least 6 servings per day, with one-third being whole grains), and lean meats and fish. It is important to limit the intake of cholesterol, trans fats, and saturated fats. Nutrients that help lower LDL-C include plant stanols/sterols (approximately 2 g/day) and soluble fiber (10-25 g/day). Smoking is a significant risk factor, particularly for myocardial infarction, stroke, and peripheral vascular disease. Research has consistently shown that smoking adversely affects the LDL-C to HDL-C ratio and reduces HDL levels.
6. CONCLUSION
Lipid disorders, known as dyslipidaemia, refer to irregularities in lipoprotein metabolism, characterized by elevated levels of total cholesterol, LDL-C, or triglycerides (TG), as well as reduced levels of HDL-C. These conditions can be either acquired or hereditary. Over the past five years, dyslipidaemia has emerged as one of the three most prevalent disorders globally, influenced by various modifiable and non-modifiable risk factors. Modifiable factors encompass diet, physical activity, and smoking habits, while non-modifiable factors include age and gender. Adiposopathy can be exacerbated by an unhealthy diet and a sedentary lifestyle, particularly in individuals who are genetically or environmentally predisposed. Most patients remain asymptomatic for many years before any physical symptoms manifest. Although multiple lipid abnormalities may coexist, management strategies are tailored to the specific lipid irregularity present. Numerous countries and regions have established their own guidelines for dyslipidaemia. The prevention and treatment of this condition involve a range of procedures, including risk assessment, setting treatment goals, increasing physical activity, dietary changes, medical therapy, follow-up, reassessment, and necessary adjustments to the treatment plan.
REFERENCES

Bhakti Nagare*, Dr. Anjali Wankhade, Dr Vivek Paithankar, A Comprehensive Review of Risk Factor and Management of Hyperlipidemia, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 4, 2471-2478. https://doi.org/10.5281/zenodo.15258519
 10.5281/zenodo.15258519
10.5281/zenodo.15258519
