Sri Raghavendra College of Pharmacy, Bangalore, Karnataka, India
Drug–drug interactions are an important concern in patients receiving multiple therapies, especially when treatments for chronic conditions overlap. Pyridostigmine [4,5,6], a cholinesterase inhibitor used in myasthenia gravis, and glimepiride [1,2,3,7], a sulfonylurea antidiabetic, are rarely studied together. Interaction checkers list this combination as a “possible risk,” mainly due to the potential for enhanced hypoglycaemia, but the evidence behind this warning is weak. In this review, we explain why doctors might be cautious about using pyridostigmine and glimepiride together, summarize what has been reported so far, and point out the important questions that research still hasn’t answered.
Patients with neuromuscular disorders such as myasthenia gravis may also suffer from type 2 diabetes, especially with increasing age. This raises the possibility of concurrent use of pyridostigmine [4,5,6] and glimepiride [1,2,3,7]. While no strong clinical reports confirm a dangerous interaction, online drug-interaction tools often flag this pair as a “moderate risk.” The problem is that these warnings are not backed by solid clinical studies. This paper reviews what is currently known, the theoretical concerns, and where further research is needed.
2. Pharmacology of the Two Drugs
3. Theoretical Basis for Interaction
Pharmacokinetically, there is no significant overlap—pyridostigmine [4,5,6] is not metabolized by the liver to any major extent, whereas glimepiride [1,2,3,7] is largely metabolized by CYP2C9 [2,3,7]. So, metabolism is not the issue.
The concern is pharmacodynamic. Pyridostigmine [4,5,6] can increase vagal tone, which may indirectly enhance insulin release or worsen hypoglycaemic episodes triggered by glimepiride [1,2,3,7]. Add to that the possibility that cholinergic side effects—like sweating, dizziness, or fatigue—can mimic or mask hypoglycaemia, making detection harder for patients.
4. What the Evidence Says
At present, very little real-world data exists:
In short, the cautionary label seems to be based more on theory than on clinical evidence.
5. Why This Matters Clinically
Even without hard data, patients on both drugs deserve careful monitoring. Hypoglycaemia remains the most serious concern—especially in elderly patients, those with irregular eating habits, or those on other antidiabetic medications.
A practical step for clinicians is to educate patients about recognizing and managing low blood sugar. If pyridostigmine [4,5,6] is added to a diabetic patient’s regimen, closer glucose monitoring may be justified.
6. Areas Needing More Study
At this point, what stands out most is how little we actually know. The caution about combining pyridostigmine [4,5,6] and glimepiride [1,2,3,7] is mostly theoretical, and there are no strong studies to confirm it. To move forward, a few things are especially important:
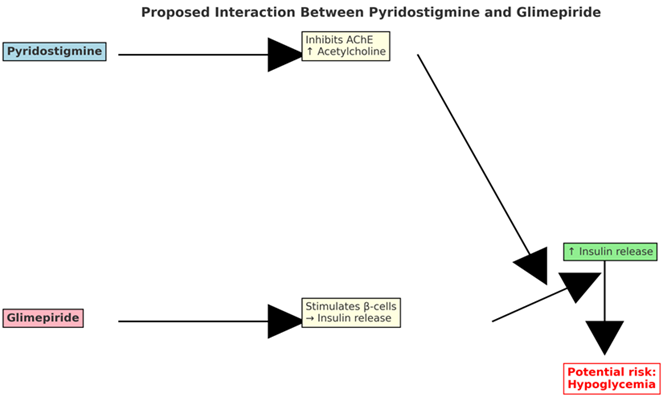
Figure 1. Proposed interaction between pyridostigmine and glimepiride.
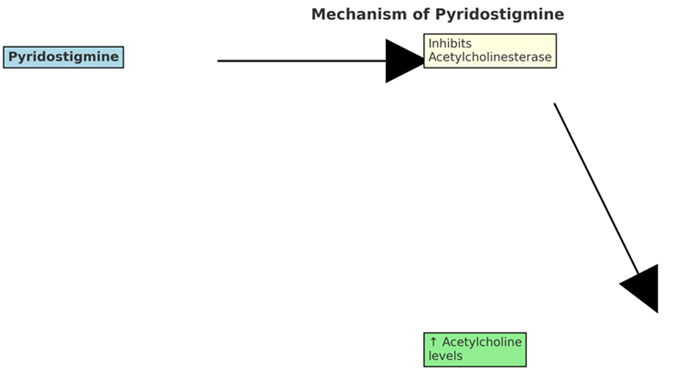
Figure 2. Mechanism of pyridostigmine.
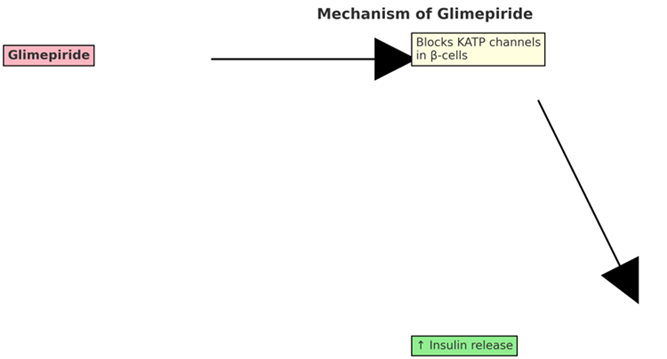
Figure 3. Mechanism of glimepiride.
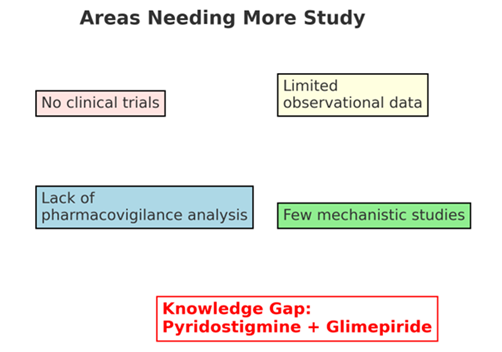
Figure 4. Areas needing more study regarding pyridostigmine–glimepiride interaction.
CONCLUSION
Right now, the evidence for an interaction between pyridostigmine [4,5,6] and glimepiride [1,2,3,7] is more theoretical than proven. While most interaction checkers err on the side of caution, no convincing clinical studies confirm the risk. Until stronger data emerge, clinicians should remain alert, educate patients about hypoglycaemia, and monitor carefully when these drugs are co-prescribed.
REFERENCES


Gudladona Raghava Ravali, M Durga Bhavani, A Review on the Potential Interaction Between Pyridostigmine and Glimepiride, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 1773-1776. https://doi.org/10.5281/zenodo.17136131
 10.5281/zenodo.17136131
10.5281/zenodo.17136131
