
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Faculty of Pharmacy, Sigma University, Bakrol, Vadodara, Gujarat, India. -390019
Introduction: Overview of the global health and significance of CHF. Definition and classification system (e.g.-HFrEF, HFpEF, etc.). Impact of CHF, complication occurring due to CHF, the management of CHF. Epidemiology and Etiology: Prevalence and incidence of CHF. Major risk factor (e.g. Hypertension, coronary artery disease, diabetes, obesity). underlying causes (e.g. ischemic heart disease, valvular heart disease, cardiomyopathies). Pathophysiology: A section explaining the mechanism of cardiac remodelling, cellular dysfunction with the result of pulmonary and peripheral Edema. Clinical manifestations and Diagnosis: Signs and symptoms (e.g. shortness of breath, oedema, fatigue). Diagnostic modalities (e.g. clinical assessment, biomarkers, Imaging techniques like echocardiography, MRI). Management strategies/ therapeutic intervention: Lifestyle modifications (e.g. Diet, exercise, Fluid Retention). Medication (e.g. ACE inhibitor, beta blocker, diuretics). Device therapy (CRT-D device). Some other management. Conclusion: It is a summary of key finding and their implication. Early diagnosis, individualized therapy and integration of emerging treatments are essential to improving long-term outcomes in CHF patients.
Chronic Heart Failure (CHF) or Heart Failure (HF) is identified as a major clinical syndrome and public health problem that has persisted as an "emerging epidemic" since its designation in 1997.
In 2005 approximately 30% of global deaths (17.5 million) were attributable to cardiovascular disease (CVD). Chronic heart failure (CHF) significantly contributes to this disease burden and is the leading cause of all hospitalizations and readmissions in older people, accounting for a large proportion of developed countries’ national health care expenditure.
CHF is a complex clinical syndrome resulting from any functional or structural cardiac disorder that reduces the ventricle's ability to fill or expel blood. This chronic condition means the heart cannot pump enough blood required for the body’s normal functioning, leading to threatened blood supply and ineffective myocardial performance.
Stages of CHF—
HF imposes a heavy burden on health care systems. Key statistics regarding its impact include
Prevalence: The estimated prevalence of CHF in people aged 45 years or more ranges between 3% and 5% worldwide. In India, it is estimated that 8–10 million people over 20 years of age suffer from heart failure. Although the true prevalence of CHF may be higher due to under diagnosis of mild to moderate CHF.
Mortality: Despite a decline in the overall incidence of HF reported across recent studies, the burden of mortality and hospitalization remains mostly relentless. There is no cure for CHF. In its most severe form, CHF has over 50% one-year mortality. Management targets symptoms and lifestyle modifications.
CHF leading to multiple physical, psychological, and clinical complications.
Physical: Patients experience dyspnoea, fatigue, weakness, reduced exercise tolerance, and frequent respiratory symptoms such as orthopnoea and paroxysmal nocturnal dyspnoea, resulting in unpredictable life-threatening crises and repeated hospital admissions.
Psychologically: CHF imposes a significant emotional burden. Many patients suffer from social isolation, fear of symptom worsening, anxiety, depression, and loss of control over daily activities.
Comorbidities: such as diabetes, chronic kidney disease, depression, arthritis, and asthma commonly coexist, complicating disease management and worsening outcomes.
The management of Chronic Heart Failure (CHF) focuses on relieving symptoms and preventing the progression of the disease, as there is currently no specific treatment that cures the condition. Treatment plans are highly individualized, depending on the stage, type of heart failure (e.g., HFrEF or HFpEF), condition, and specific symptoms of the patient.
CLASSIFICATION
From the ‘90s clinical trials began to select patients based on left ventricular ejection fraction (LVEF), usually measured using echocardiography. To define heart failure with preserved (HFpEF), mid-range (HFmrEF) and reduced ejection fraction (HFrEF) according to ESC guidelines.
HFpEF (Heart Failure with Preserved Ejection Fraction): Ejection fraction is 50% or greater, causes due to heart’s diastolic function is impaired
HFrEF (Heart Failure with Reduced Ejection Fraction): Ejection fraction is less than 40 %, Causes due to systolic dysfunction
HFmrEF (Heart Failure with Mid-Range Ejection Fraction): Ejection fraction between 41-49%
There are another two types of heart failure, which include acute and chronic heart failure. Acute heart failure involves sudden and rapid onset, which needs a medical emergency, and chronic heart failure is developed over time, which requires long-term and manageable treatment.
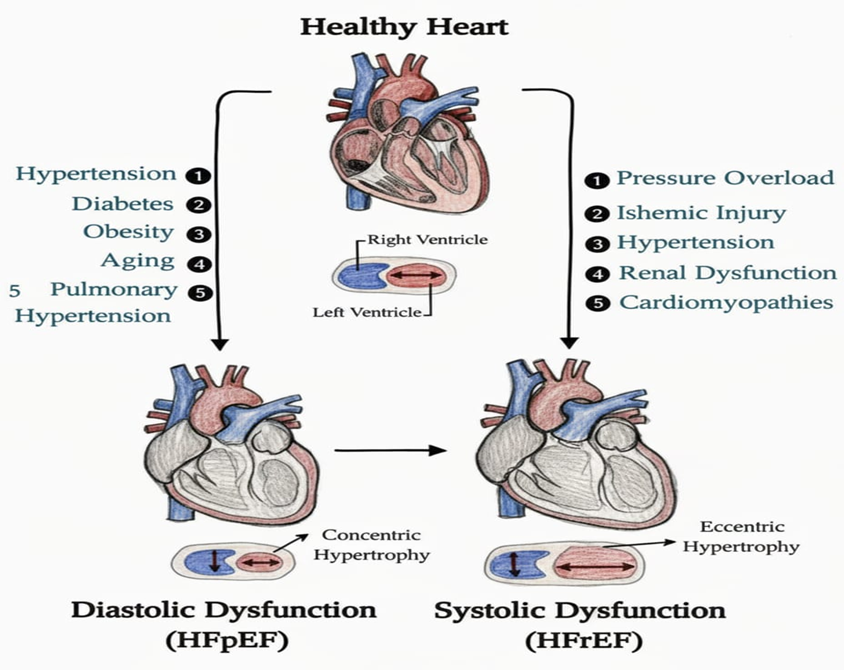
Fig.1: showing causes of HFpEF and HFrEF
ETIOLOGY OF CHF:
CHF results from abnormalities of the myocardium, valves, pericardium, rhythm, or systemic condition. Various conditions that cause heart failure:
Ischemic heart disease is the main cause of CHF. It is a condition in which, due to a lack of or decrease in blood supply. The heart muscles get damaged. It is caused due to coronary artery disease.
Hypertension may also cause CHF. When the heart works harder to pump blood, then it can lead to congestive heart failure. Hypertension induces structural and functional changes in myocardium, this includes hypertrophy of the left ventricle.
Cardiomyopathy is a disorder that affects the heart muscle. It makes it stiffen, enlarge or thicken. Cardiomyopathy makes it difficult to pump blood effectively. That's why it can lead to heart failure.
Factors like obesity, diabetes, smoking and heavy alcohol use contributes to developing heart failure.
When heart valve does not function properly, they force the heart to work harder to move blood forward.
Certain viral infections can lead to damage, to the heart muscles directly.
EPIDEMIOLOGY
CHF is a cardiac disorder that may be caused by a variety of cardiac disorders. Five million Americans should suffer from CHF. Approximately 550,000 new cases of CHF should register every year, and nearly 250,000 die every year. 2.5% of the total population has this disease. The risk for death is 5% to 10% annually in patients with mild symptoms and increases to approximately 30% to 40% annually in patients with advanced disease. Asian patients with HF are younger and have different risk factors compared with Western patients. In an analysis of the ASIAN-HF registry, the prevalence of diabetes ranged between 34.1% in Japanese/Koreans and 51.9% in Malaysian patients.
RISK FACTORS:
Like many other non-communicable diseases, HF is a preventable disease.
Women with diabetes are at high risk for developing HF. Although there may be uncertainty in the quantity of alcohol ingested and the probability of developing HF, heavy use of alcohol has been associated with increased risk for development of HF. Treating both systolic and diastolic hypertension in the long run according to contemporary guidelines reduces the risk of HF by approximately 50 percent.
PATHOPHYSIOLOGY
The pathophysiology of Chronic Heart Failure (CHF) is understood through a combination of structural and functional heart impairments, which lead to ineffective myocardial performance and the eventual failure of compensatory neurohormonal mechanisms.
Congestive heart failure can occur from two main causes that are
This all indeed leads to the decrease in the stroke volume (blood pump in each beat). Therefore, future cause to decrease in a cardiac output (blood pump in each minute). To overcome this condition, the body does a process that increases the heart rate. But that now causes less filling time.
How did this happen?
There occur some structural changes to increase the stroke volume. For that there are two changes that can occur:
When it fails to increase the stroke volume, it creates the pressure on the kidney. That leads the kidney to release renin, which further releases angiotensin, which stimulates the release of Aldosterone hence causing Na+ (salt) and water retention, therefore causing volume overload.
As a result, if the left side of the heart fails first, it will term pulmonary oedema, and if the right side of the heart fails first, it will term peripheral oedema.
CLINICAL MANIFESTATION AND DIAGNOSIS
Sign and Symptoms –
The signs and symptoms of Chronic Heart Failure (CHF) are central to its definition as a complex clinical syndrome. These manifestations vary depending on the clinical severity and whether the patient is experiencing left ventricular or right ventricular failure.
Heart failure is clinically diagnosed based on a patient's history and physical examination. The core manifestations are primarily related to exercise intolerance and fluid retention.
The most common clinical signs and symptoms of CHF include:
|
Category |
Sign / Symptoms |
Brief description |
|
Respiratory |
Exertional dyspnoea, orthopnoea, paroxysmal nocturnal dyspnoea. |
Shortness of breath on exertion due to pulmonary congestion. |
|
Respiratory |
wheezing |
Often dry or producing frothy white/pink sputum because of fluid in lungs. |
|
Circulatory |
Tachycardia |
Rapid or irregular heartbeat as compensation for reduced cardiac output. (Sensitivity% =7, Specificity% =99). |
|
Circulatory |
Elevated JVP (Jugular Venous Pressure) |
Raised jugular venous pressure indicating systemic venous congestion. (Sensitivity% =10, Specificity% =97). |
|
Oedema |
Generalized ascites |
Swelling of abdomen and sometimes hands, sacrum due to systemic congestion. |
|
Weight |
Rapid weight gain |
Sudden increase in weight over days from fluid accumulation. |
|
Fluid |
Nocturia |
Increased urination at night as recumbence improves renal perfusion. |
Diagnostic Modelist: The diagnosis of Chronic Heart Failure (CHF) relies on a combination of clinical evaluation and diagnostic testing to confirm the presence of structural or functional cardiac abnormalities, assess the severity of the syndrome, and determine the underlying cause. As there is no conclusive diagnostic test for CHF, it is primarily diagnosed clinically based on history and physical examination
|
Parameter |
Diagnose |
|
History |
Presence of symptoms such as shortness of breath (including Orthopnoea and paroxysmal nocturnal Dyspnoea), nocturia, mental status changes. Recent or previous hospitalization and symptoms suggesting Transient Ischemic Attack (TIA) are also checked. |
|
Physical Examination |
Assessment for fluid retention/congestion using markers like jugular venous pressure, peripheral oedema, pulmonary crackles, and hepatomegaly/ascites. |
|
Test |
Purpose and value |
|
Echocardiogram |
Considered the most valuable initial diagnostic test. It determines the presence of pericardial, endocardial, valvular, and vascular abnormalities. It is used to evaluate the pumping function of heart and assess systolic and diastolic abnormalities. |
|
Ejection Fraction (EF) Measurement |
EF test is very important for classifying into HF into category: HF with reduced EF (HFrEF) (≤40%) and HF with preserved EF (HFpEF) (≥50%). |
|
Electrocardiogram (ECG) |
ECG should be done compulsory because It is a basic tool for screening but ECG alone cannot give a significant diagnosis of CHF. |
|
Chest X-ray |
It is usually recommended for patients with acute, or new-onset HF to determine heart size and pulmonary oedema and to reveal other cardiopulmonary causes contributing to symptoms. |
|
Biomarkers (BNP/NT-proBNP) |
BNP and NT-proBNP are simple blood tests that help doctors check for heart failure (HF) in people short of breath. It helps to Predicts risk: Higher levels mean worse outlook or advanced HF needing special treatments. |
|
Blood Tests |
It includes complete blood count, serum electrolytes, blood urea nitrogen (BUN), serum creatinine, glucose, liver function tests, and thyroid-stimulating hormone. A high sensitivity Troponin-T test helps diagnose a heart attack. |
MANAGEMENT OF THE CHF
There is no specific treatment that cures the congestive heart failure. The main objective of the treatment is to relieve the symptoms and to prevent the progression of CHF.
ACE Inhibitors: Ex: Captopril, Enalapril, Ramipril. These drugs inhibit angiotensin-converting enzymes, so they are used in congestive heart failure. ACE catalyses the conversion of angiotensin I to pharmacologically active angiotensin II.
Beta Blocker: Ex: - Metoprolol and Carvedilol. Beta-blockers have recently emerged as a new class of drugs for heart failure patients. B-blockers prevent stimulation of the sympathetic nervous system by inhibiting the action of a catecholamine at B-adrenergic receptors; by this, they improve left ventricular function.
Diuretics: Diuretics are effective for controlling fluid retention and reducing symptoms of congestion by reducing preload, but they do not prevent disease progression.
Cardiac Glycosides: E.g., digoxin, digitoxin. Cardiac glycosides are called cardiotonic agents. They increase the mechanical efficiency of the heart as a pump without increasing oxygen consumption.
CONCLUSION
The provided source offers a comprehensive overview of heart failure (HF), Focusing on its classification, management, and recent research findings. Its and academic review details the pharmacological and device-based therapies for HF with reduced ejection fraction (HFrEF), efficiency of the medication and some other management, another part is review establishes the epidemiological burden of HF, emphasizing classification and outlining Standard treatments. Finally, a clinical trial sub-analysis investigates the impact of personalized nutritional intervention in chronic HF patient who are at risk of malnutrition, it helps us to know the Signs and symptoms of CHF, and its Diagnosis devices.
Hence it collectively, from source highlight the complete information about CHF and its Management and Diagnosis.
REFERENCES

Trupti Rajput, Taksh Patel, Brief Understanding and Treatment of Congestive Heart Failure, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 3553-3561. https://doi.org/10.5281/zenodo.18046043
 10.5281/zenodo.18046043
10.5281/zenodo.18046043