
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Anangpuria School of Pharmaceutical Sciences, Ballabgarh-Sohna Road, Faridabad, Haryana
Dementia encompasses a spectrum of syndromes characterized by progressive cognitive decline that impairs memory, behavior, and activities of daily living. Among the various subtypes, Alzheimer’s disease (AD) is the most prevalent, accounting for up to 75% of cases, followed by vascular dementia (VaD), which represents the second most common cause, particularly among older adults. VaD results from diminished cerebral perfusion secondary to vascular pathology such as stroke, which leads to neuronal death and subsequent cognitive impairment. The prevalence of VaD varies geographically, with estimates ranging from 10-15% in developed nations and reaching up to 30% in developing countries. Pathophysiologically, VaD is associated with reduced cerebral blood flow, small vessel disease, and oxidative stress. Major contributory factors include advancing age, cardiovascular risk factors, and lifestyle elements. Vascular damage induces neuroinflammation, oxidative damage, and neuronal necrosis, thereby exacerbating cognitive deficits. Experimental models for studying VaD include techniques such as cerebral vessel occlusion, high-fat diet models, and chemical induction, each designed to replicate different aspects of the disease’s underlying mechanisms. Clinically, VaD presents with cognitive and behavioral deficits similar to those observed in AD but is often distinguished by a stepwise progression of symptoms and evidence of vascular pathology in the brain. Risk factors for VaD strongly overlap with those for cerebrovascular disease, including hypertension, diabetes mellitus, and hyperlipidemia. A comprehensive understanding of these mechanisms and risk factors is essential for the development of effective therapeutic and preventative interventions for vascular dementia.
Dementia is a syndrome characterized by a progressive decline in memory, cognition, behavior, activities of daily living, and overall quality of life. Several distinct types exist, each with unique etiologies and clinical features. The most common subtypes include Alzheimer’s disease (AD), vascular dementia (VaD), Lewy body dementia, frontotemporal dementia, Huntington’s disease, and dementia associated with Parkinson’s disease. Vascular dementia, often resulting from cardiovascular and cerebrovascular pathologies, is particularly prevalent among older adults and ranks as the second most common cause of dementia after AD (Kalaria et al., 2008).
Types of Dementia
Vascular Dementia
Vascular dementia (VaD) predominantly affects the elderly and is recognized as the second most common dementia after Alzheimer’s disease (Kalaria et al., 2008). It results from cerebrovascular abnormalities that impair cerebral blood flow, leading to neuronal damage affecting cognitive, behavioral, and memory functions (Aarsland, 2010). Post-mortem studies reveal that approximately 40% of clinically diagnosed VaD cases exhibit mixed pathology, notably AD-type neurodegeneration (Nolan et al., 1998).
Epidemiology of VaD
Following AD, VaD is the most frequently encountered dementia, with an incidence rate of approximately 15-30% depending on geographic location—higher in developing nations (Davis et al., 2018). Stroke survivors are at increased risk, with estimates suggesting that around 7% of the general population develops post-stroke dementia. The risk is notably higher—up to 40%—in individuals with pre-existing cognitive impairment before a stroke (Kalaria et al., 2016). Longitudinal data show that around 25% of stroke survivors develop new-onset dementia within a year, with annual incidence rates ranging from 5% post-transient ischemic attacks to 34% after major strokes (Pendlebury et al., 2019). Globally, over 47.5 million individuals suffer from dementia, with more than 7.7 million new cases annually (WHO, 2016).
Etiology of Vascular Dementia
Research identifies multiple risk factors for VaD, many overlapping with those for other cerebrovascular diseases. These include age, hypertension, insulin resistance, hyperlipidemia, atherosclerosis, and diabetes. Lifestyle factors such as smoking, diet, physical inactivity, and genetic predispositions also contribute. Protective factors encompass higher educational attainment, regular physical activity, a Mediterranean diet rich in omega-3 fatty acids, vitamins B12, E, and C, which may mitigate vascular and oxidative stress (Fratiglioni et al., 1996; Hachinski et al., 1993).
AD and VaD share a few common causes, including:
Alzheimer’s disease (AD) and vascular dementia (VaD) share several common etiological factors, including age, gender, genetic predispositions, inflammatory processes, and specific atherogenic conditions or vascular risk factors. Additional potential risk factors encompass a family history of stroke, psychological stress, exposure to pesticides, and diets high in saturated fats. Conversely, certain protective factors have been identified, such as higher educational attainment, regular physical activity, consumption of fish or shellfish, intake of vitamin B12, adherence to a Mediterranean diet, and the supplementation of antioxidants including vitamins E and C.
Pathophysiology of Vascular Dementia
Cognitive impairment in VaD is not a uniform disease entity but exhibits heterogeneous presentations. It is often accompanied by stroke-related symptoms and may result from multiple minor thromboembolic events, or localized damage to critical brain regions such as the thalamus or frontal lobes which serve strategic cognitive functions. In most cases, individuals with VaD exhibit diffuse cerebral injury attributable to microangiopathy, which is frequently followed by nonspecific neuronal symptoms (Fratiglioni et al., 1996). The specific brain regions affected in vascular dementia are illustrated in Figure 1.
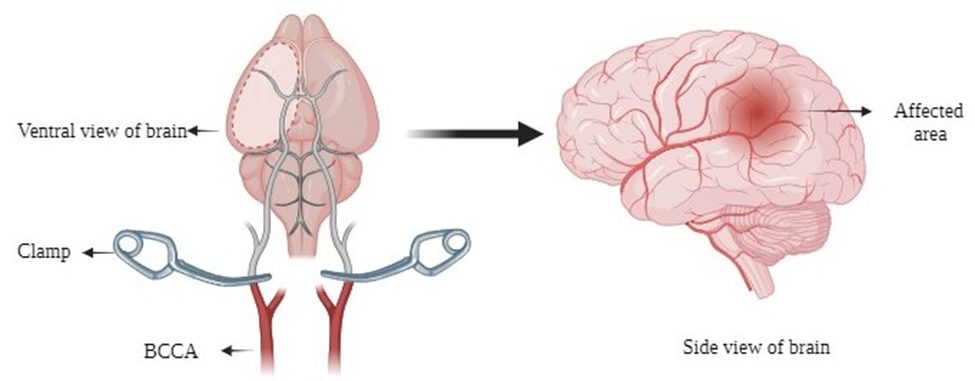
Fig. 1: Vascular dementia-affected brain region
Several pathways contribute to the development of dementia in stroke patients, including:
The pathophysiology of ischemic vascular dementia primarily involves the management of major vessel diseases. However, it is also recognized that the effects of vascular stenosis may impair cerebral blood flow even in the absence of infarction, such as in cases of atherosclerosis and other arterial diseases, whose clinical implications require further investigation.
The two main components of vascular dementia (VaD) are the clinical manifestations of dementia and the underlying vascular pathology. According to current clinical criteria, VaD has traditionally been considered distinct from Alzheimer’s disease (Bir et al., 2021). Nonetheless, these conditions share several common features. For example, the accumulation of amyloid beta 1-42 (Aβ1-42) and amyloid precursor protein—hallmarks of AD—have also been observed in animal models of cerebral ischemia and in patients with multi-infarct dementia, which represents the most prevalent form of VaD. Cognitive impairment in VaD results from vascular neuronal damage caused by hemodynamic abnormalities such as intracranial hemorrhage, cortical strokes, lacunar infarctions, small vessel disease, and recurrent microbleeds (Wiesmann et al., 2013). It is widely accepted that obstructive hemodynamic events affecting the periventricular white matter, hippocampal cortex, and prefrontal cortical-basal ganglia networks are initial insults that lead to broader pathological consequences, including hypoperfusion-driven neurodegeneration. These include thromboembolism, decreased cerebral blood flow, oxidative and nitrosative stress from oxygen deprivation, glial cell activation eliciting neuroinflammation, and neuronal necrosis (Venkat et al., 2015). Research particularly emphasizes the involvement of hyperhomocysteinemia, hypoxia-induced oxidative stress, and reactive nitrogen species in the pathogenesis of VaD (Wiesmann et al., 2013). Reduced basal levels of nitric oxide (NO) in the brain—a common feature of age-related and cerebrovascular diseases—compromise vascular dilation, leading to decreased regional cerebral blood flow (CBF). This reduction fosters the accumulation of oxygen and nitrogen free radicals, which disrupt redox homeostasis and promote oxidative and nitrosative stress (Li et al., 2013). According to Venkat et al. (2015), hypoxic conditions can impair mitochondrial function, aggravating neuronal injury and potentially triggering apoptotic cell death.
Inflammatory alterations and reactive white matter inflammation have been identified in both clinical and research studies as key components in the pathophysiology of vascular dysfunction (Bir et al., 2021). Limited blood supply and insufficient collateral circulation in deep brain regions contribute to the heightened vulnerability of cerebral white matter to hypoxia-induced injury. Demyelination, primarily resulting from oligodendrocyte destruction caused by hypoxia, is the main pathological substrate of white matter damage in vascular dementia (VaD) (Youssef et al.,., 2013). Moreover, the extent to which white matter pathology and lacunar infarcts, in conjunction with subcortical VaD, are influenced by large vessel disease remains unclear. Statistically, these relationships suggest a potential impact on the pathophysiology of small vessel disease. Additionally, evidence indicates that microvascular changes play a significant role in cerebral tissue impairment and the progression of cognitive deficits. Small vessel lesions associated with extensive lacunar infarcts and white matter alterations are frequently observed in subcortical forms of vascular cognitive impairment (Vinters et al., 2000). In summary, the primary mechanisms underlying VaD involve vascular pathology and oxidative stress, which can be summarized as follows:
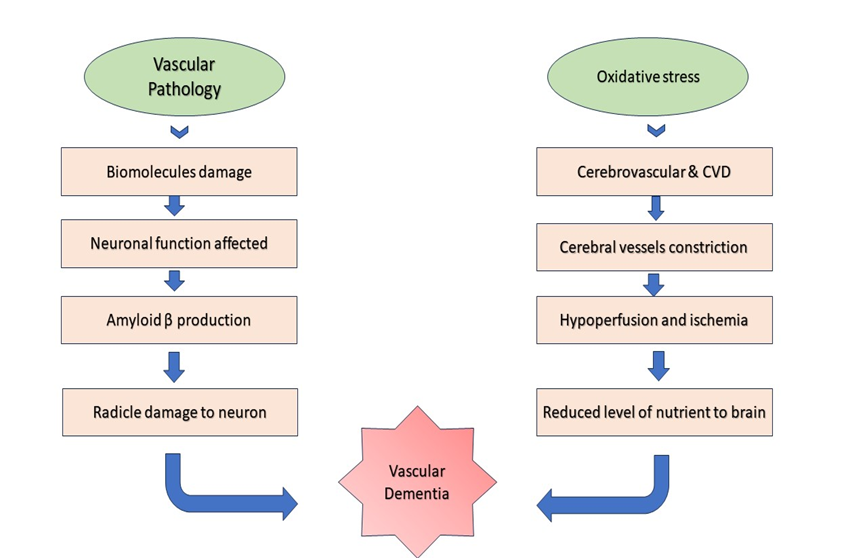
Fig.2: Pathophysiology of Vascular dementia
Models for Vascular Dementia
Currently, there are no FDA-approved treatments specifically for vascular dementia (VaD). Consequently, researchers have focused on developing reliable animal models to better understand the disease mechanisms and to facilitate the discovery of potential therapeutic interventions. An ideal animal model should accurately replicate the pathophysiological features of VaD and produce results that are translatable to human conditions. It is important to recognize that VaD may arise from various pathophysiological processes and risk factors, either independently or in combination. Despite this heterogeneity, most existing models share the common feature of cognitive decline.
1. Blood Vessel Occlusion Models
i) Bilateral Common Carotid Artery Occlusion (BCCAO) or Two-Vessel Occlusion (2VO)
This model aims to induce global cerebral hypoperfusion, mimicking conditions observed in aging or after certain vascular events in humans. It involves the permanent occlusion of both carotid arteries bilaterally (Huang et al., 2017). Variations in this model include differences in the resulting pathophysiology, such as white matter diffusion, white matter damage, disruption of the blood-brain barrier (BBB), and neuronal damage in the hippocampus and cortex—often confirmed via MRI. Additionally, this model induces inflammation and gliosis predominantly affecting white matter (Soria et al., 2013). Cognitive deficits are primary outcomes in this model, with impairments observed in learning and memory tasks, such as increased latency in the Morris water maze, reduced performance in the Y maze, object recognition deficits, and motor coordination abnormalities in tests like the foot fault and beam balance (Sarti et al., 2002).
ii) Four-Vessel Occlusion (4VO):
In this model, both the common carotid arteries (CCAs) and the vertebral arteries (VAs) are occluded on successive days (Pulsinelli et al., 1979). The occlusion of these vessels is typically permanent, with variations involving the duration of carotid artery occlusion—from approximately 10 minutes to permanent occlusion (Neto et al., 2005). Vertebral artery occlusion is most often achieved via electrocauterization (Pulsinelli et al., 1988). Different classification schemes exist for permanent vessel occlusion, with some studies reporting higher mortality rates with two-stage occlusion (bilateral CCA followed by VA occlusion) versus three-stage procedures. This model induces significant cognitive impairment, as demonstrated by performance deficits in the elevated plus maze, radial maze, and spatial learning tasks, alongside early neuronal damage characterized by Fluoro-Jade staining and increased glial fibrillary acidic protein (GFAP) expression within 24 hours—gradually increasing over 72 hours—and elevated tau protein expression (Bir et al., 2021).
iii) Unilateral Common Carotid Artery Occlusion (UCCAO):
In this model, one carotid artery is permanently ligated. Rats subjected to UCCAO experience chronic cerebral hypoperfusion, leading to white matter damage, increased inflammatory responses, decreased anti-inflammatory cytokines, and reduced synaptic plasticity and neuronal integrity (Zhao et al., 2014). Behaviorally, these animals do not exhibit significant deficits in learning and memory, but they display heightened anxiety (not depression) and reduced exploratory behavior, as assessed by the elevated plus maze and open field tests. Short-term memory impairments have been observed via the Novel Object Recognition Test (Yoshizaki et al., 2008). However, a limitation of this model is the lack of clear histological evidence of tissue damage.
iv) Bilateral Common Carotid Stenosis (BCAS)
This approach involves occluding both CCAs successively with micro-coils, with a brief interval between occlusions (Shibata et al., 2004). The diameter of the micro-coils must be carefully selected to regulate the severity of cerebral injury. In rats, white matter lesions develop within one week post-procedure, whereas in mice, similar changes appear within two weeks, likely due to differences in baseline cerebral blood flow reductions (Nishio et al., 2010). This model results in decreased cerebral glucose uptake, hippocampal atrophy, white matter gliosis, disruption of the BBB, and inflammatory responses (Nakaji et al., 2008). Cognitive deficits, including impaired learning, memory, and motor coordination, persist for months post-occlusion, although early (30-day) assessments often do not detect memory deficits (Shibata et al., 2007). Notably, this model does not fully replicate the small vessel disease (SVD) pathology but rather induces chronic hypoperfusion leading to vascular cognitive impairment (Khan et. al.,2015).
Abundant evidence suggests a strong link between cognitive deficits and a high-fat diet, particularly in activities associated with the hippocampus in the elderly population. Although the implications and mechanisms are not yet fully understood, studies have demonstrated that rats on a high-fat diet for two months displayed impairments in learning and memory. The extent of cognitive damage was comparable to that observed in rats on a normal diet that were either old or had suffered cerebral strokes or brain injuries (Winocur et al., 2005). The Rotterdam Study, also known as ERGO, examined the prevalence, risk factors, and causal factors of various neurological illnesses in the elderly. It reported an association between a high-fat diet and circulatory risks, as well as cognitive impairment and memory decline. In individuals over 55 years old, high cholesterol and increased total fat intake were linked to a higher incidence of dementia, particularly vascular dementia (VaD). Research indicated that rats on a diet high in fat, cholesterol, and non-reducing sugars showed declines in cognitive, learning, and memory abilities, with cognitive decline potentially leading to weight gain. Some studies have found that cognitive impairment and high-fat diet-induced oxidative injury occurred only with a diet composed of 60% lard-based fat, as opposed to a general diet containing less than 40% fat (Pistell et al., 2010).
3. Chemical Method of VaD
VaD can also be induced by certain chemicals through multiple pathways, including alcohol, lipopolysaccharide, L-Cysteine (L-Cys), aluminum trichloride, and streptozotocin (STZ). L-Cys, classified as a semi-essential amino acid, is vital for regulating metabolism in humans (Ripps et al., 2012). There are three primary endogenous sources of L-Cys: dietary absorption, the trans-sulfuration process, and protein degradation. Disruptive changes in the extracellular L-Cys/L-Cys ratio may be associated with oxidative stress (Li et al., 2017). STZ, a naturally occurring chemical, is derived from the fungus species Streptomyces achromogenes. It contains a nitrosourea moiety that interacts between glucosamine and a methyl group. The molecular mechanism of STZ involves inhibiting DNA formation in mammalian and bacterial cells, attributable to the presence of a cytosine moiety, leading to bacterial DNA degradation (Szkudelski et al., 2001). Additionally, STZ prevents cell division during the mitotic phase. In mammals, STZ induces potential toxicity to insulin-producing beta cells in the pancreas. While STZ is sometimes used to treat specific cancers in Islets of Langerhans cells, it serves experimentally to induce dose-dependent type 1 and type 2 diabetes mellitus, primarily in rodents such as rats and mice. Recently, unilateral or bilateral intracerebroventricular injections of STZ and L-Cys have been recognized to cause neuronal damage, mainly in the hippocampus, through the production of oxidative stress and phosphatase activation due to insulin dysfunction (Genrikhs et al., 2017). Insulin dysfunction can also lead to memory deficits by initiating inflammatory responses and the expression of apoptotic proteins, affecting tau protein pathology.
Signs & Symptoms of Vascular Dementia
Clinical signs of sub-cortical and vascular conditions may not be immediately apparent and include subtle and mild deficits associated with impaired decision-making, facial motor symptoms, walking difficulties with unpredictable and recurring falls, increased urination, mild confusion, and changes in behavior and mood (Meiron et al., 2017). Multi-infarct dementia is considered the most typical form of vascular dementia. It is thought to result from multiple minor or major cerebral infarcts that affect cortical and sub-cortical regions. Arterial occlusion typically occurs in large-caliber cerebral arteries, often leading to atherosclerotic thrombosis or cardiogenic embolism (Moorhouse et al., 2008; Aggarwal et al., 2007). Vascular dementia, the most severe form of vascular cognitive impairment (VCI), is characterized by cognitive impairment, clinical stroke, or vascular brain injury (Gorelick et al., 2011).
Clinical Examination of Vascular Dementia
Vascular dementia typically progresses either in a "step-wise" manner or through a gradual decline in cognition and memory. In the case of subcortical vascular dementia, the clinical presentation is characterized by a subcortical syndrome with symptoms such as the inability to perform normal daily activities, decline in psychomotor activity, pseudobulbar palsy, and gait disturbances. Vascular dementia and Alzheimer's disease often coexist, making differentiation challenging. Signs such as dysphasia, dyspraxia, and neglect may also be present in vascular dementia cases with cortical lesions (Gorelick et al., 2011). Currently, the most active therapeutic options for Alzheimer's disease involve cholinesterase inhibitors and glutamate receptor antagonists (Meiron et al., 2017). However, there is uncertainty regarding the long-term benefits of these treatments for VaD, although they are used off-label in some countries to alleviate symptoms in patients with vascular dementia (Farlow et al., 2008). Geriatric clinical examination methods to distinguish vascular dementia from Alzheimer's disease focus on identifying the primary site of vascular damage in VaD compared to the neurodegeneration in AD, which primarily affects sub-cortical and cortical regions (Staekenborg et al., 2008). Damage to larger blood vessels in cortical regions often leads to lateralized sensory motor symptoms, while injury to subcortical regions can cause brain parenchyma damage or chronic atherosclerosis due to thrombosis in small vessels and embolism. These subcortical vascular disease disorders significantly impact white matter pathways (such as commissural/projection fibers) and cerebral nuclei (such as basal ganglia).
Risk Factors for Vascular Dementia
Numerous studies suggest that the risk factors for VCI and vascular dementia are often similar. Common risk factors include hypertension, insulin resistance, hyperlipidemia, hyperhomocysteinemia, atherosclerosis, and diabetes, evident in both humans and animal models (Cohen et al., 2010; Sahathevan et al., 2012). Age is another risk factor, with a significant increase in dementia prevalence observed in individuals over the age of 65, which also impacts vascular dementia (Corrada et al., 2008). Furthermore, cerebrovascular dysfunction is a risk factor for the decline of cerebrovascular function in dementia patients (Sabayan et al., 2012). Additionally, several studies reveal a connection between cognitive decline and metabolic syndrome, which includes common symptoms of vascular dementia such as hypertension, insulin resistance, and dyslipidemia (Yates et al., 2012).
CONCLUSION
Vascular dementia (VaD) is a prevalent form of dementia characterized by cognitive decline due to impaired cerebral blood flow. It is the second most common type of dementia after Alzheimer's disease. VaD often presents with symptoms similar to other dementias, but it is primarily associated with vascular damage to the brain, including strokes and chronic small vessel disease. The pathophysiology of VaD involves complex mechanisms such as oxidative stress, white matter damage, and impaired neurovascular function. Epidemiologically, VaD affects a significant proportion of older adults, with its prevalence varying across different regions and populations. Risk factors for VaD include age, hypertension, diabetes, hyperlipidemia, and smoking, all of which contribute to the vascular lesions and cognitive impairments observed in VaD patients. Research into animal models of VaD, such as blood vessel occlusion models and high-fat diet-induced models, is crucial for understanding the disease mechanisms and developing potential treatments. Despite advances, there remains no FDA-approved treatment specifically for VaD, underscoring the need for continued research. Effective clinical management of VaD requires distinguishing it from other types of dementia, particularly Alzheimer's disease, as they can coexist and present overlapping symptoms. Identifying and targeting the underlying vascular and oxidative stress mechanisms are essential for improving patient outcomes and developing therapeutic strategies.
In summary, addressing the risk factors and understanding the pathophysiology of VaD are key to advancing both preventive and therapeutic measures for this debilitating condition.
REFERENCES


Naveen Kumar, Jyoti Malik, Shiv Kumar Yadav, Deepika Yadav, Clinical Insights into Vascular Dementia: From Pathophysiology to Risk Assessment, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 7, 1635-1647. https://doi.org/10.5281/zenodo.15869483
 10.5281/zenodo.15869483
10.5281/zenodo.15869483