
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1,2,3,5,6 Faculty of Pharmacy, Uttar Pradesh University of Medical Sciences, Saifai, Etawah, Uttar Pradesh, 206130
4 Faculty of Marine Sciences, Annamalai University, Parangipettai, Tamil Nadu
7 Radha Raman Mishra College of Pharmacy
8 Department of Pharmaceutical Sciences, Gurukula Kangari Deemed to be University, Haridwar, Uttarakhand
Background: Obesity has become a major global public health issue, with its prevalence continuing to increase across all demographics and regions up to 2026. Current data suggest that over a billion adults worldwide are affected, with particularly rapid growth seen in low- and middle-income nations. This growing problem is closely associated with cardiometabolic diseases, cancer, and decreased life expectancy. This review compiles recent findings on global obesity patterns, primary causes, underlying biological mechanisms, and modern prevention strategies, focusing on dietary changes and scalable interventions. An extensive review of epidemiological data, randomized controlled trials, cohort studies, and meta-analyses published from 2020 to 2026 was performed. Evidence concerning lifestyle changes, functional foods, nutraceuticals, pharmacological treatments, and policy-level strategies was thoroughly assessed. The progression of obesity is influenced by multiple factors, including the increased intake of ultra-processed foods, sedentary behavior, urbanization, biological predispositions, and socioeconomic inequalities. On a physiological level, dysfunction in adipose tissue, insulin resistance, chronic low-grade inflammation, and gut–brain axis dysregulation contribute to excessive weight gain. Lifestyle interventions show modest but lasting reductions in BMI, while newer pharmacological treatments result in significant weight loss in clinical environments. Emerging research underscores the importance of dietary shifts towards fiber- and polyphenol-rich functional foods, like millets, in enhancing satiety, glycemic control, and metabolic health, especially in population-level prevention.Conclusion: To reverse current obesity trends, urgent, integrated, and multi-level actions are necessary. Combining dietary innovations, evidence-based pharmacological treatments, and supportive policy changes provides a feasible approach to reducing obesity-related health risks beyond 2026. Long-term, longitudinal studies and implementation-focused research are crucial to translating these strategies into a sustainable public health impact.
Obesity represents a rapidly escalating global health crisis affecting individuals across all age groups and genders and obesity is currently ranked as the fifth most common leading cause of death globally. Obesity affects essentially every organ system in the body, and it serves as a major risk factor for a wide range of chronic conditions, including type 2 diabetes, cardiovascular diseases, chronic kidney disease, multiple malignancies, osteoarthritis, and dementia. As a central pathological driver of metabolic syndrome characterized by insulin resistance, hypertension, dyslipidemia, and hyperglycemia, obesity heightens the risk of cancers, coronary heart disease, and stroke. This widespread issue poses a significant global public health challenge due to its complex and far-reaching impacts on health and disease progression [1].
The World Health Organization (WHO) defines overweight and obesity as abnormal or excessive fat accumulation that impairs health, with overweight classified by a body mass index (BMI) ≥25 kg/m² and obesity by a BMI ≥30 kg/m². Globally, obesity affects over 890 million adults, accounting for approximately 16% of the adult population [2]?. In India, data from the National Family Health Survey-5 (NFHS-5) indicate a marked rise in overweight and obesity prevalence, affecting 44.02% of men and 41.16% of women, compared with 37.71% and 36.14%, respectively, reported in NFHS-4 [3]?. Notably, obesity prevalence demonstrates pronounced socioeconomic disparities, particularly among women and childhood obesity rates have increased over four-fold in that time [4]?. Worldwide, the number of adults living with obesity has risen dramatically from 105 million in 1975 to over 890 million by 2022, with projections estimating a continued increase to approximately 1.13 billion adults by 2030, underscoring the urgent need for effective prevention and therapeutic strategies [5]?. This unchecked growth is expected to impose substantial economic strain on healthcare systems, driven by escalating costs related to long-term disease management, disability, and reduced workforce productivity.
Despite advances in lifestyle interventions and pharmacotherapy, the long-term effectiveness and safety of existing anti-obesity strategies remain limited, with high rates of weight regain and treatment discontinuation. Consequently, there is an urgent need to explore novel, safe, and sustainable therapeutic approaches that target multiple metabolic pathways involved in obesity pathogenesis. In this context, growing attention has been directed toward functional foods and bioactive dietary components as adjunct or alternative strategies for obesity prevention and management, offering potential benefits through improved metabolic regulation and reduced cardiometabolic risk.
GLOBAL TRENDS AND EPIDEMIOLOGICAL DATA
Between 2020 and 2026, the global prevalence of obesity has continued to rise at an unprecedented pace, reinforcing its status as one of the most pressing public health challenges of the 21st century. Recent data show the global obesity burden rising across all regions, age demographics, and socioeconomic levels, with especially rapid acceleration in low- and middle-income countries (LMICs) that grapple with a dual malnutrition burden—where elevated obesity rates persist alongside ongoing undernutrition and micronutrient deficiencies. [6,7]. This shift represents a marked departure from earlier decades, during which obesity was predominantly concentrated in high-income nations.
Regionally, the most rapid increases in obesity prevalence during this period have been documented in South Asia, Sub-Saharan Africa, the Middle East, and parts of Southeast Asia, driven by rapid urbanization, dietary westernization, reduced physical activity, and economic transitions [8]. In contrast, while high-income countries continue to exhibit high absolute obesity prevalence, the rate of increase has plateaued or slowed in several regions, reflecting the partial impact of public health interventions and heightened awareness [9].
Age-specific analyses reveal a troubling rise in obesity among younger populations, including adolescents and young adults, signaling a shift toward earlier disease onset and prolonged lifetime exposure to cardiometabolic risk. Concurrently, obesity prevalence remains highest among middle-aged and older adults, contributing substantially to the global burden of diabetes, cardiovascular disease, and disability-adjusted life years (DALYs). Gender-based disparities are also evident, with higher obesity prevalence observed among women in many LMICs, often linked to sociocultural norms, reduced physical activity, and inequities in access to health resources [10].
The accelerated rise of obesity in LMICs reflects a complex interplay of demographic, nutritional, and environmental transitions, including increased consumption of energy-dense, nutrient-poor ultra-processed foods, declining physical activity due to mechanization and urbanization, and limited access to preventive healthcare. This surge occurs despite persistent malnutrition, creating a double burden of malnutrition (DBM)—where undernutrition coexists with overweight/obesity within individuals—and a triple burden (TBM) that also encompasses micronutrient deficiencies and anemia [11]. These conditions cluster paradoxically in richer households of poorer LMICs and poorer households of richer LMICs, exacerbated by UPFs displacing traditional healthy diets, with over 70% of countries (mainly Indonesia, Guatemala) now experiencing DBM.
If current trajectories persist, LMICs will bear >60% of the projected 1.13 billion global obesity cases by 2030, offsetting malnutrition gains with escalating obesity-related disability and mortality, thus demanding urgent region-specific strategies and scalable interventions like millet-based nutraceuticals [12].
Table 1. Regional trends in adult obesity prevalence and key drivers (2020–2026)
|
Region |
2020 prevalence (%) |
2026 prevalence (%) |
Key drivers |
References |
|
North America |
~36–38 |
~41–43 |
High consumption of ultra-processed foods, sedentary lifestyles, socioeconomic disparities, obesogenic environments |
14,16,17,19 |
|
Europe |
~23–25 |
~27–30 |
Aging populations, physical inactivity, dietary transitions, socioeconomic inequalities |
14,16,19 |
|
South Asia |
~8–10 |
~13–15 |
Rapid urbanization, dietary westernization, reduced physical activity, genetic susceptibility |
15,16,18,20 |
|
East & Southeast Asia |
~10–12 |
~15–18 |
Nutrition transition, increased fast-food intake, urban lifestyles, metabolic vulnerability |
15,16,18 |
|
Middle East & North Africa |
~25–28 |
~30–35 |
High-energy diets, low physical activity, cultural norms, climate-related inactivity |
14,16,19 |
|
Sub-Saharan Africa |
~7–9 |
~11–14 |
Urban migration, reduced manual labor, dual burden of malnutrition, limited preventive care |
15,16,20 |
|
Latin America & Caribbean |
~25–28 |
~30–34 |
Sugary beverage intake, urbanization, socioeconomic transitions, physical inactivity |
14,16,18,19 |
|
Low- and Middle-Income Countries (overall) |
~15–17 |
~22–25 |
Rapid economic transition, food system changes, limited public health infrastructure |
13,15,16,20 |
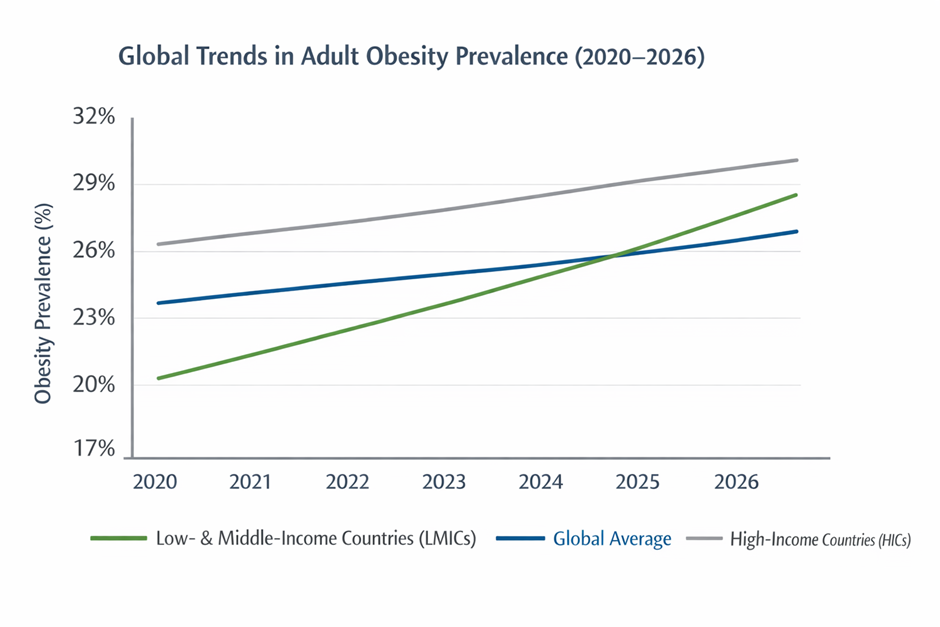
Figure 1. Global trends in adult obesity prevalence across income groups (2020–2026).
MULTIFACTORIAL DRIVERS OF THE OBESITY SURGE
The rapid escalation of obesity prevalence observed globally between 2020 and 2026 (Figure 1) reflects the convergence of multiple biological, behavioral, and structural determinants rather than a single causative factor. This multifactorial nature underscores the complexity of obesity pathogenesis and the challenges associated with its prevention and management.
Dietary transitions: ultra-processed foods and sugar intake
The global rise in obesity is largely driven by a shift in dietary habits towards ultra-processed foods (UPFs), which are known for their high energy content, refined carbohydrates, added sugars, unhealthy fats, and low levels of essential nutrients. The increased intake of sugary drinks, fast food, and processed snacks is closely linked to higher calorie consumption, insulin resistance, and increased body fat [21,22]. This trend is especially evident in low- and middle-income countries (LMICs), where the rapid globalization of food systems has outpaced public health regulations, resulting in greater access to and affordability of diets that promote obesity [23].
Sedentary behavior and urbanization
Urbanization has significantly transformed physical activity patterns, leading to a notable increase in sedentary lifestyles. The mechanization of work, more time spent in front of screens, reliance on motorized transportation, and fewer chances for recreational exercise have collectively reduced daily energy expenditure among populations [24]. Urban settings often encourage sedentary habits due to insufficient infrastructure for active transportation and limited access to safe green areas, heightening the risk of obesity, especially in children and working-age adults [25].
Genetic susceptibility, gut microbiota, and endocrine disruptors
Biological factors play a crucial role in determining an individual's propensity for obesity. Genetic influences dictate appetite regulation, fat storage, and energy metabolism, all of which interact with environmental conditions [26]. Recent research highlights the role of gut microbiota imbalances in obesity, as they can modify energy extraction, trigger inflammation, and impact metabolic signaling [27]. Additionally, exposure to endocrine-disrupting chemicals (EDCs) such as bisphenols and phthalates is associated with increased fat cell production, hormonal imbalances, and metabolic disturbances, elevating the risk of obesity even at low exposure levels [28].
Socioeconomic and policy influences
Socioeconomic inequalities significantly shape obesity patterns, with higher prevalence observed among disadvantaged populations due to limited access to nutritious foods, healthcare, and opportunities for physical activity. Inadequate policy frameworks, weak food labeling regulations, aggressive marketing of unhealthy foods, and insufficient taxation of sugar-sweetened beverages further exacerbate obesity trends [29]. Conversely, evidence suggests that comprehensive policy interventions—such as fiscal measures, urban planning reforms, and food system regulation—can mitigate obesity risk when effectively implemented [30].
Collectively, these interconnected drivers explain the accelerated rise in obesity prevalence illustrated in Figure 1 and emphasize the need for integrated, multisectoral strategies that address both biological vulnerability and structural determinants of health.
PATHOPHYSIOLOGICAL MECHANISMS UNDERLYING OBESITY PROGRESSION
The swift escalation in obesity rates stems from both environmental/behavioral influences and intricate pathophysiological processes that impair energy balance and metabolic control. Key mechanisms include adipose tissue dysfunction, insulin resistance, persistent low-grade inflammation, and gut-brain axis dysregulation, forming a vicious cycle that sustains weight gain and metabolic decline.
Adipose tissue dysfunction and ectopic fat accumulation
Adipose tissue is an active endocrine organ that regulates energy storage, lipid metabolism, and hormonal signaling. In obesity, excessive adipocyte hypertrophy and hyperplasia impair adipose tissue expandability, leading to hypoxia, fibrosis, and altered adipokine secretion [31]. This dysfunctional adipose tissue shows diminished secretion of insulin-sensitizing adipokines like adiponectin alongside elevated release of leptin, resistin, and pro-inflammatory cytokines, driving metabolic dysregulation. Once adipose storage capacity is overwhelmed, ectopic lipid deposition occurs in the liver, skeletal muscle, and pancreas, intensifying insulin resistance and metabolic impairment[32].
Insulin resistance and metabolic inflexibility
Insulin resistance represents a cornerstone of obesity and a primary driver of metabolic syndrome. Chronic exposure to excess free fatty acids, inflammatory mediators, and oxidative stress disrupts insulin signaling pathways in peripheral tissues, impairing glucose uptake while enhancing hepatic gluconeogenesis. Obesity simultaneously induces hyperinsulinemia that activates PI3K/AKT/mTOR and RAS/MAPK pathways, promoting cancer cell proliferation and protein synthesis. Elevated insulin further boosts insulin-like growth factor (IGF-1) levels, fostering inflammation, immune suppression, mitogenesis, angiogenesis, and apoptosis resistance to accelerate cancer progression [33]. This metabolic inflexibility hampers the body's capacity to shift seamlessly between fat and glucose metabolism, perpetuating positive energy balance and hastening adipose accumulation. Compensatory hyperinsulinemia eventually drives further adipogenesis, establishing a self-reinforcing cycle that propels ongoing weight gain and elevates type 2 diabetes risk [34].
Chronic low-grade inflammation
Obesity is characterized by chronic low-grade systemic inflammation originating from dysfunctional adipose tissue, where enlarged adipocytes and infiltrating macrophages secrete pro-inflammatory cytokines including TNF-α, IL-6, and CRP. In obese individuals, adipose-resident macrophage numbers positively correlate with circulating inflammatory markers (TNF-α, CRP), while both local adipose and systemic inflammation inversely associate with insulin sensitivity and skeletal muscle oxidative capacity [35]. This inflammatory milieu disrupts insulin signaling, alters lipid metabolism, and contributes to endothelial dysfunction, thereby linking obesity to cardiometabolic diseases. Persistent inflammation also affects central appetite regulation, further compounding weight gain [36].
Gut–brain axis dysregulation
The gut-brain axis critically regulates appetite, energy homeostasis, and metabolic function via bidirectional signaling between the gastrointestinal tract, gut microbiota, and central nervous system. In obesity, gut microbiota dysbiosis, heightened intestinal permeability ("leaky gut"), and disrupted microbial metabolite production impair these pathways, promoting excessive hunger and metabolic dysregulation. [37]. These changes impair satiety signaling and promote systemic inflammation. Additionally, dysregulation of neurohormonal pathways involving leptin, ghrelin, glucagon-like peptide-1 (GLP-1), and peptide YY (PYY) disrupts appetite control and reward signaling, leading to increased food intake and reduced energy expenditure [38]. Collectively, these alterations reinforce maladaptive eating behaviors and sustained weight gain.
Taken together, these interconnected mechanisms explain the persistence and rapid progression of obesity observed globally and highlight the necessity for therapeutic strategies that target multiple metabolic and neuroendocrine pathways rather than focusing solely on caloric restriction.

Fig 2. Pathophysiological mechanisms underlying obesity and metabolic dysregulation
CURRENT PREVENTION AND MANAGEMENT PATHWAYS FOR OBESITY
Given obesity's multifactorial origins and intricate pathophysiology, successful prevention and management demand comprehensive approaches integrating lifestyle changes, nutritional strategies, and pharmacological or surgical interventions. Contemporary pathways prioritize early intervention, metabolic risk mitigation, and sustained outcomes over mere short-term weight reduction.
Lifestyle interventions: diet, physical activity, and behavioral therapies
Lifestyle modification remains the cornerstone of obesity prevention and management. Dietary interventions focusing on caloric restriction, improved macronutrient quality, increased fiber intake, and reduced consumption of ultra-processed foods have demonstrated consistent benefits in weight reduction and metabolic improvement [39]. Regular physical activity enhances energy expenditure, improves insulin sensitivity, and reduces visceral adiposity, while behavioral therapies—such as cognitive behavioral therapy (CBT), motivational interviewing, and self-monitoring—support adherence and long-term behavior change [40]. However, despite their proven efficacy, lifestyle interventions often face challenges related to sustainability, socioeconomic barriers, and individual variability in response.
Nutraceuticals and functional foods
Growing interest has focused on nutraceuticals and functional foods as complementary strategies for obesity prevention, particularly due to their safety profile and potential for long-term use. Whole grains such as millets are gaining attention for their high dietary fiber, polyphenols, and bioactive compounds, which contribute to improved satiety, glycemic control, lipid metabolism, and gut microbiota modulation [41,42]. Soluble and insoluble fibers delay gastric emptying and reduce postprandial glucose spikes, while polyphenols exert anti-inflammatory and antioxidant effects that may counteract obesity-associated metabolic dysfunction. These properties position millets and similar functional foods as promising, culturally adaptable dietary tools for obesity prevention, especially in low- and middle-income countries.
Pharmacological and bariatric interventions
Pharmacological therapies are recommended for individuals with moderate to severe obesity or obesity-related comorbidities when lifestyle measures alone are insufficient. Recent advances include incretin-based therapies such as glucagon-like peptide-1 (GLP-1) receptor agonists and dual GLP-1/GIP agonists, which promote weight loss by enhancing satiety, delaying gastric emptying, and improving insulin sensitivity [43]. While effective, these agents may be limited by cost, accessibility, and long-term safety considerations.
For severe or refractory obesity, bariatric surgery remains the most effective intervention, producing sustained weight loss and significant improvements in metabolic outcomes, including remission of type 2 diabetes and reduction in cardiovascular risk [44]. Nevertheless, surgical approaches require careful patient selection, long-term follow-up, and substantial healthcare resources, highlighting the need for scalable preventive strategies.
Collectively, these prevention and management pathways underscore the importance of a multidisciplinary approach that integrates lifestyle modification, dietary innovation, and medical interventions to address the growing global obesity burden.

Fig 3. Current prevention and treatment pathways for obesity management
EVIDENCE FROM RECENT INTERVENTIONS (2020–2026)
Over the past decade, a growing body of high-quality evidence from randomized controlled trials (RCTs), cohort studies, and meta-analyses has evaluated the effectiveness of diverse obesity prevention and management strategies. These studies collectively underscore the importance of multi-component interventions that combine dietary modification, physical activity, behavioral support, and scalable public health measures in achieving meaningful reductions in body mass index (BMI) and related metabolic outcomes.
Randomized Controlled Trials
Recent large-scale RCTs have demonstrated significant BMI reductions with structured lifestyle interventions that integrate diet, exercise, and behavior modification. In the DiRECT and PREVIEW trials, structured dietary regimens combined with physical activity and behavioral support produced sustained decreases in BMI and improvements in metabolic profiles over 12–24 months [45,46]. Notably, interventions emphasizing caloric reduction and increased fiber intake achieved mean BMI reductions ranging from 2.5 to 4.0 kg/m², with concomitant reductions in waist circumference and insulin resistance.
Pharmacological RCT evidence has also markedly advanced. Semaglutide and other glucagon-like peptide-1 receptor agonists (GLP-1 RAs) have consistently produced robust weight loss in overweight and obese adults, with mean reductions exceeding 10% of baseline body weight and significant BMI declines compared with placebo in multi-center trials [47]. Dual agonists targeting incretin pathways (e.g., GLP-1/GIP) have further enhanced efficacy, highlighting the potential for pharmacotherapy to complement lifestyle strategies.
Cohort Studies and Real-World Evidence
Prospective cohort studies conducted between 2020 and 2026 provide compelling real-world data supporting scalable interventions. Longitudinal analyses in diverse populations have shown that community-based lifestyle programs, including workplace wellness initiatives and school-based nutrition education, are associated with modest but meaningful BMI declines and reduced incidence of obesity-related comorbidities over 3–5 years [48]. Cohort data also reinforce the role of dietary quality—characterized by higher intake of whole grains, fruits, and vegetables—in moderating long-term weight gain.
Meta-Analyses and Systematic Reviews
Recent meta-analyses synthesizing RCT and observational data confirm the effectiveness of multi-component interventions for obesity prevention at the population level. Comprehensive reviews of lifestyle-based RCTs report pooled BMI reductions of approximately 1.5 to 3.5 kg/m², with greater effects observed in programs combining dietary and physical activity components [49]. Meta-analyses of pharmacological trials also underscore the superior efficacy of newer agents compared with older therapies, while highlighting the need for long-term safety data and cost-effectiveness evaluations [50].
Population-Level and Policy Interventions
Evidence from natural experiments and policy evaluations highlights the impact of scalable strategies such as sugar-sweetened beverage (SSB) taxation, front-of-pack labeling, and urban design policies that promote active transport. Jurisdictions implementing SSB taxes have reported significant declines in SSB consumption and modest attenuations in population-level BMI trends, demonstrating the potential of fiscal policies in shifting obesogenic environments [51]. Similarly, urban planning initiatives that enhance opportunities for walking and cycling have been linked to improvements in physical activity and reductions in obesity risk.
Collectively, evidence from the past six years emphasizes that multi-level, multi-component strategies—spanning individual behavior change to policy-level interventions—are essential for achieving sustained reductions in BMI and curbing the global obesity epidemic. These findings support the design and implementation of culturally tailored and scalable preventive frameworks across diverse settings.
Table: Impact of Recent Interventions on BMI and Weight Outcomes
|
Intervention type |
Study design & population |
Duration |
Mean BMI / weight reduction |
Key findings |
Reference |
|
Intensive lifestyle intervention (diet + PA + CBT) |
RCT, adults with obesity (n ≈ 300–500) |
12–24 months |
↓ BMI 2.5–4.0 kg/m² |
Significant BMI reduction with improved insulin sensitivity and lipid profile |
52,53 |
|
High-fiber/whole-grain diet (incl. millets) |
RCT & cohort studies |
6–12 months |
↓ BMI 1.2–2.3 kg/m² |
Increased satiety, reduced glycemic load, improved gut health |
54,55 |
|
GLP-1 receptor agonists (e.g., semaglutide) |
Multicenter RCTs |
68 weeks |
↓ body weight 10–15% (≈ ↓ BMI 4–6 kg/m²) |
Superior efficacy vs placebo; improved cardiometabolic markers |
56 |
|
Dual incretin agonists (GLP-1/GIP) |
Phase III RCTs |
52–72 weeks |
↓ body weight 15–22% |
Enhanced appetite control and sustained weight loss |
57
|
|
Community-based programs |
Prospective cohort |
3–5 years |
↓ BMI 0.5–1.5 kg/m² |
Modest but scalable population-level benefit |
58 |
|
Sugar-sweetened beverage (SSB) taxation |
Natural experiment & meta-analysis |
2–6 years |
↓ BMI 0.3–0.8 kg/m² |
Reduced SSB intake and slowed obesity growth |
59 |
|
Bariatric surgery (RYGB, sleeve gastrectomy) |
Long-term cohort & RCTs |
5+ years |
↓ BMI 10–15 kg/m² |
Most effective for severe obesity; durable remission of T2DM |
60 |
POLICY RECOMMENDATIONS AND FUTURE DIRECTIONS
The accelerating global burden of obesity demands coordinated, evidence-based policy action alongside continued innovation in prevention and treatment. Given the multifactorial drivers and complex pathophysiology of obesity, future strategies must extend beyond individual behavior change to address structural determinants, food systems, and long-term therapeutic evaluation.
Food environment and regulatory reforms
Reforming food environments represents a critical policy priority for obesity prevention. Governments should strengthen regulations targeting ultra-processed foods through mandatory front-of-pack nutrition labeling, restrictions on marketing of unhealthy foods—particularly to children—and fiscal measures such as sugar-sweetened beverage taxation [61,62]. Evidence from multiple countries demonstrates that such policies effectively reduce consumption of energy-dense, nutrient-poor foods and contribute to favorable shifts in population-level BMI trends. Urban planning policies that promote active transport, safe recreational spaces, and walkable communities should also be integrated into national obesity prevention frameworks.
Promotion of millets and traditional whole grains in dietary guidelines
Integrating millets and other traditional whole grains into national dietary guidelines offers a culturally appropriate, sustainable, and cost-effective strategy for obesity prevention, particularly in low- and middle-income countries. Millets are rich in dietary fiber, polyphenols, and micronutrients, and exhibit low glycemic indices, contributing to improved satiety, glycemic control, and lipid metabolism [63, 64]. Policy measures should include agricultural incentives for millet production, inclusion of millet-based foods in public distribution systems, school meal programs, and community nutrition initiatives. Such approaches align nutritional goals with environmental sustainability and food security.
Strengthening health systems and access to evidence-based care
Health systems must be equipped to deliver comprehensive obesity care through early screening, counseling, and access to multidisciplinary interventions. Expanding coverage for evidence-based pharmacotherapies and ensuring equitable access to obesity management services are essential to reduce disparities in obesity outcomes. Capacity building among healthcare professionals and integration of digital health tools for monitoring and behavioral support may further enhance scalability and effectiveness [65].
Future research directions and longitudinal evaluation
Future Research Directions
Despite promising advances, critical gaps persist regarding the long-term safety, economic viability, and practical deployment of new obesity treatments. Future studies must focus on expansive, multi-year randomized controlled trials that track durable weight loss, metabolic improvements, and cardiovascular outcomes for innovative drugs and nutraceuticals. Implementation research is equally vital to determine how dietary breakthroughs—like millet-based functional foods—can scale effectively across varied populations and healthcare settings [66]. Integrating genomic, microbiome, and digital health data into intervention studies may further enable precision-based obesity prevention strategies.
In conclusion, addressing the obesity epidemic requires a synergistic approach that combines policy reform, dietary innovation, healthcare system strengthening, and rigorous long-term research. Such integrated strategies are essential to curb obesity trends and mitigate their profound health, economic, and societal consequences.

CONCLUSION
The global obesity crisis intensifying through 2026 demands urgent, multifaceted action, fueled not just by personal choices but by intertwined biological, lifestyle, and systemic forces. Research spanning epidemiology, disease mechanisms, and treatment trials reveals obesity as a complex societal issue, far beyond individual willpower, calling for unified efforts across sectors.
Single approaches—be they diet tweaks, medications, or policies in isolation—fall short of reversing this tide at population scale. Instead, promising paths forward blend nutrient-dense foods like fiber- and polyphenol-packed millets (tailored to your research focus) with proven drugs, alongside reforms to food marketing, urban design for activity, and equitable healthcare access.
Looking ahead, we need real-world studies tracking long-term safety and impact of new therapies across diverse groups, especially in rapidly affected regions like India. Only by syncing cutting-edge nutrition—like millet-based interventions—with pharmacology and bold policies can we stem obesity's projected climb past 2026. Without this coordinated push from individuals to governments, the toll in diabetes, heart disease, and beyond will only grow, making now the time for decisive change.
REFERENCES








Pooja Kushwah, Ranjeet Kumar, Istuti Srivastava, Gowarthanan Ranganathan, Prakash Tiwari, Kamlesh Patel, Shanu Mishra, Anil Kumar Maurya, Obesity in 2026: Analyzing the Rapid Rise and Pathways to Prevention, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 824-838. https://doi.org/10.5281/zenodo.18494036
 10.5281/zenodo.18494036
10.5281/zenodo.18494036