
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Krantiveer Vasantrao Narayanrao Naik Shikshan Prasarak Sanstha's, Institute of Pharmaceutical Education & Research, Canada Corner, Nashik - (422002) Maharashtra, India.
Pharmacovigilance (PV), which involves the evaluation, tracking, and identification of drug interactions and their effects on humans, is essential to the healthcare system. Although pharmaceutical and biotechnological medications are intended to prevent, cure, or treat illnesses, there are hazards associated with them as well. In particular, adverse drug reactions (ADRs) have the potential to seriously injure patients. ADR monitoring is therefore necessary for medication safety at every stage of a drug's life cycle, including pre-marketing, which includes early phases of drug design, clinical trials, and post-marketing surveillance. PV is concerned with the identification, evaluation, comprehension, and avoidance of adverse drug reactions. Clinical research relies heavily on pharmacogenetics and pharmacogenomics. Pharmacovigilance is becoming more and more popular in many nations these days as a crucial and essential component of clinical research. Although there are numerous pharmacovigilance centers trying to monitor medication safety in this global arena today, pharmacovigilance faces significant obstacles in improving drug safety and monitoring at the turn of the millennium. This review will cover medication safety, global pharmacovigilance centers, their function, the advantages and disadvantages of pharmacovigilance, and its potential applications in the healthcare industry. In order to improve their contribution to public health, industry, drug regulators, clinicians, and other healthcare professionals must work together to help patients recover and manage their conditions as best they can, ideally preventing illness. This paper provided a critical analysis of PV's current state in India, obstacles to overcome, and potential future developments in relation to the Indian setting, while also summarizing the goals and approaches employed in the field.In addition to outlining the new paths that pharmacovigilance has taken, this review defines the science of pharmacovigilance and the adverse event reporting process. It also gives HCPs who manage dialysis patients insight into the critical role they play in influencing the understanding of a drug's safety profile in order to continuously improve patient safety.
Pharmacovigilance is defined as the pharmacological science relating to the detection, assessment, understanding, and prevention of adverse effects, particularly long-term and short-term side effects, of medicines. [1] Recently, there has been a lot of interest in the area of drug safety. Both scientific journals and tabloids publish articles about medications that result in unexpected adverse drug reactions (ADRs) almost every week. Unfortunately, these stories have the effect of making people anxious about using these medications, both patients and medical professionals. A more catastrophic outcome could be that the patient quits taking the drug as directed, which could result in a scenario that is even more serious than the ADR that initially worried him.[2] Pharmacovigilance serves as a watchful guardian while a medication moves from preclinical research to human trials and eventually hits the market, constantly keeping an eye out for any adverse effects that might manifest in a variety of patient demographics and real-world situations. The systematic collection and analysis of adverse event reports is a crucial part of pharmacovigilance. Adverse events might range from mild, expected reactions to severe, unanticipated, or protracted consequences. It is essential to categorize and comprehend these occurrences in order to differentiate between typical pharmacological side effects and those that actually endanger patient safety. This classification serves as the foundation for the subsequent processes in risk management. Pharmacovigilance is closely related to the regulatory frameworks established by international organizations such as the European Medicines Agency (EMA), the U.S. Food and Drug Administration (FDA), and other national regulatory authorities. These organizations set up guidelines and protocols that regulate the collection, sharing, and evaluation of safety data during a drug's lifecycle. These guidelines must be scrupulously followed by pharmaceutical corporations and medical professionals to ensure that a drug's safety profile is continuously assessed. Pharmacovigilance has grown as a result of both technology advancements and shifts in cultural expectations. Early pharmacovigilance mostly depended on patients' and healthcare providers' unprompted reporting. Modern pharmacovigilance, on the other hand, uses real-world data, electronic health records, and advanced data mining tools to proactively find possible safety warnings. Pharmacovigilance procedures are changing to meet the problems presented by biologics, gene therapies, and other cutting-edge treatments as pharmaceutical goods get more complicated. Additionally, the field is embracing patient viewpoints more and more as it recognizes the importance of patient-reported results and insights in determining the actual effects of medications on people. [3]

Fig No. 1. Introduction to PV
Historical Perspectives of WHO - Drug Safety Monitoring
In 2002, there were pharmacovigilance facilities in over 65 countries. The Uppsala Monitoring Centre (UMC), also known as the WHO Collaborating Centre for International Drug Monitoring, is responsible for coordinating WHO membership for international drug monitoring. Effective clinical practice currently relies heavily on pharmacovigilance, which is founded on solid scientific concepts. To satisfy the needs of contemporary public health and public expectations, the field must advance. A resolution was adopted by the Sixteenth World Health Assembly [4]. which ultimately resulted in the establishment of the WHO Pilot Research Project for International Drug Monitoring and reiterated the necessity of prompt action with relation to the quick distribution of information on adverse drug reactions. The goal was to create a method that could be used globally to identify previously unidentified or poorly understood side effects of medications. [5]
Scope of PV
Since the WHO technical report in 1972, PV has advanced significantly and is still a dynamic clinical and scientific field. It has been crucial to address the challenges of the growing variety and potency of pharmaceutical and biological medicines, including vaccines, which carry with them an unavoidable and occasionally unpredictable potential for harm. The risk of harm is reduced, however, when medications are used by knowledgeable medical professionals and by patients who are aware of and take responsibility for their medications. When side effects and toxicity arise, especially when they were previously unidentified in relation to the medication, it is crucial that they are properly evaluated and conveyed to a knowledgeable audience. This is PV's role, and it has already seen significant progress. However, more is needed to incorporate the subject into public policy and clinical practice. A pharmaceutical business in India must fundamentally perform tasks like collection and prompt reporting of major unexpected adverse drug reactions (ADRs) in order to meet the PV responsibilities for its marketed goods under laws. [6] A typical setup for PV studies, including people involved on various levels, organizational units and their functions are shown in Figure 2.
Fig No.2. A Typical Pharmacovigilance
Pharmacovigilance And International Health
The Erice Declaration offers a framework of values and practice for the collection, analysis, and subsequent communication of drug safety issues. Today, the burden of ADRs on public health remains significant despite the progress made in pharmacovigilance. The Uppsala Monitoring Center coordinates the current global network of pharmacovigilance centers, which would be strengthened by an independent system of review. This would consider crucial and contentious drug safety issues that have the potential to negatively affect public health beyond national boundaries.[7] According to pharmacoeconomic studies on the expenses of adverse reactions, governments provide a sizeable portion of their health budgets to pay for these expenses. [8] But it's becoming more and more obvious that sociopolitical, economic, and cultural issues have a direct impact on the safety profile of medications, which in turn influences public perceptions, usage trends, and access to medications. [9,10]
Drug Utilization:
One of the main factors influencing drug safety is drug usage patterns. For example, developing nations are more likely to use injectable medications. [11] In many nations, direct marketing of prescription medications to consumers has been the norm. With this knowledge, patients feel more capable of choosing their own treatments without the help of a physician or pharmacist. Self-medication, the legal and illegal online sale of medications, and doctors writing excessive prescriptions on patients' requests have all increased as a result. The rise in prescriptions has been significantly impacted by this. [12, 13] However, these public health initiatives don't have to solely target patients; they can also be used to benefit the broader population. Partnerships with the media, educational institutions, and governmental and non-governmental groups could significantly aid in these awareness-raising and educational efforts, which should also involve the elderly and children. National pharmacovigilance centers' contributions are crucial to the WHO International Drug Monitoring Programs' performance. A pharmacovigilance center should ideally exist in every nation. [14]
Regulatory Framework
A strong regulatory framework that sets rules, standards, and processes for the observation and evaluation of drug safety is essential to the efficient operation of pharmacovigilance.
This framework is necessary to guarantee the methodical identification, assessment, and prevention of adverse outcomes associated with pharmaceutical products. International and state regulatory bodies play a crucial role in the creation and upkeep of these frameworks. [15] Global regulatory organizations that offer comprehensive guidelines and standards for pharmacovigilance practices include the World Health Organization (WHO), the European Medicines Agency (EMA), the Pharmaceuticals and Medical Devices Agency (PMDA) in Japan, and the U.S. Food and Drug Administration (FDA). These organizations work together to create standardized guidelines that enable reliable cross-border medication safety monitoring. National regulatory bodies use the principles established by these organizations as a basis for creating their own pharmacovigilance frameworks. [16]
National Regulatory Authorities and their Roles:
Pharmacovigilance efforts within their respective jurisdictions are supervised by the regulatory bodies of each nation at the national level. These authorities establish certain rules and practices that are suited to the distinct healthcare environment and demographics of their various nations. [17] National regulatory bodies are responsible for approving and overseeing pharmaceutical goods from preclinical research to post-marketing. In the context of pharmacovigilance, they set deadlines for submitting safety data, mandate that adverse events be reported, and cooperate with foreign organizations to solve issues related to international safety. Additionally, national authorities check pharmaceutical businesses to make sure they are adhering to pharmacovigilance requirements. [18]
Key Components of Pharmacovigilance:
The field of pharmacovigilance is broad and includes a number of essential elements, all of which are vital to the methodical detection, evaluation, and control of side effects linked to pharmaceutical products. To guarantee the safety of medications at every stage of their lifespan, from development to post-marketing surveillance, it is crucial to comprehend these elements. [19]
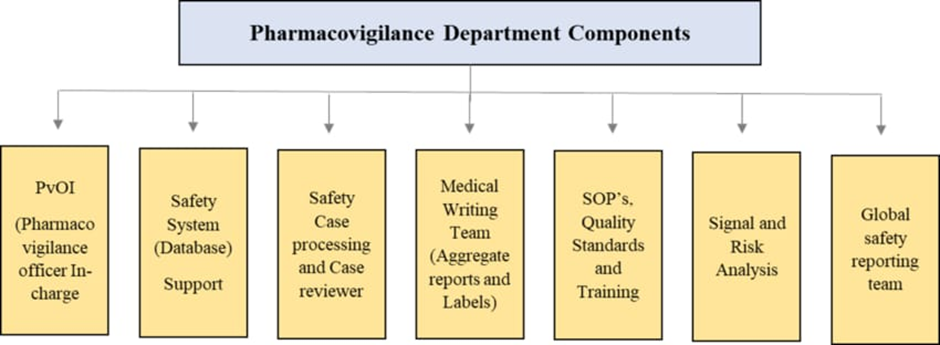
Fig No. 3. Pharmacovigilance Components
Worldwide Soldiers of Pharmacovigilance
In the process of drug safety monitoring, a wide range of partners have intricate and crucial relationships. Together, these partners must foresee, comprehend, and address the ever-increasing needs and expectations of the general public, lawmakers, policymakers, health administrators, and medical professionals.
The Quality Assurance and Safety:
The group is a member of the WHO Health Technology and Pharmaceuticals cluster's Department of Essential Drugs and Medicines Policy. By bridging the enormous gap between the potential that essential drugs have to offer and the fact that, for millions of people, especially the poor and disadvantaged, medications are unavailable, unaffordable, unsafe, or misused, the department hopes to improve health and save lives. [20]
The Uppsala Monitoring Centre:
The Uppsala Monitoring Center's main responsibility is to oversee the global database of ADR reports that National Centers provide. To encourage quick signal detection, the UMC standardized reporting by all National Centers and eased international communication. [21]
The National Pharmacovigilance Centers:
Raising public knowledge of medication safety has been greatly aided by National Centers. The fact that many national and regional centers are located outside the boundaries of a drug regulating body, in hospitals, medical colleges, or poison and drug information centers, is partially to blame for this growth. To gather epidemiological data on adverse medication reactions, major centers in industrialized nations have set up active surveillance programs that use prescription event monitoring systems (PEM) and record linkage. The United States of America, Sweden, the United Kingdom, and New Zealand have already adopted such systems. When weighed against the national spending on medications or the cost of adverse drug reactions to the country, the total cost of a pharmacovigilance system is incredibly low. [22, 23]
Hospitals and Academia:
In their clinics, wards, and emergency rooms, several medical facilities have implemented close watch systems for medication errors and adverse reactions. The use of case-control studies and other pharmacoepidemiological techniques to calculate the harm caused by medications after they are put on the market has grown. The teaching, training, research, policy formulation, clinical research, ethical committees (institutional review boards), and clinical services offered by academic centers of pharmacology and pharmacy have all contributed significantly. [24,25,26]
Health Professionals:
Originally physicians were the only professionals invited to report as evaluating whether disease or medicine causes a given symptom by applying the skill of differential diagnosis. Various types of drug-related issues will be observed by various groups of medical professionals today. [27,28]
Patients:
The true benefits and risks of a medication are only known by the patient. Direct patient involvement in drug-related problem reporting will improve the pharmacovigilance system's effectiveness and make up for some of the drawbacks of systems that rely solely on reports from medical experts
Pharmacovigilance In Drug Regulation
Partnerships with regulators strengthen pharmacovigilance programs. Regulators are aware that pharmacovigilance is essential to maintaining the continuous safety of pharmaceuticals.
Clinical trial regulation:
The number of clinical trials in both industrialized and developing nations has significantly increased in recent years. Regulatory agencies consider the safety and effectiveness of newly developed products while approving clinical trials. Clinical practice should incorporate safety monitoring of commonly used medications. Effective patient care is improved by health professionals receiving education and training on medication safety, by national pharmacovigilance centers exchanging information, by coordinating this exchange, and by connecting clinical experience with research and health policy. This kind of consistent information flow and interchange puts national pharmacovigilance programs in a prime position to spot knowledge gaps about diseases brought on by medications. [29]
Post marketing safety drug monitoring:
These include monitoring the negative effects of drug residues in animals, such as hormones and antibiotics, on human health, detecting drug interactions, calculating the environmental burden of medications used by large populations, evaluating the contribution of "inactive" ingredients to the safety profile, and comparing the safety profiles of similar medications. A more methodical approach to evaluating the merits of currently accessible medications has been facilitated by the Council for International Organizations of Medical Sciences' (CIOMS) study on benefit-risk assessment of medications after marketing. [30]
Pharmacovigilance in national drug Policy:
National governments are in charge of providing high-quality, safe, and effective medications and ensuring that they are used appropriately. Particularly important is multidisciplinary collaboration; connections must be made between the various health ministry departments as well as with other stakeholders, including the pharmaceutical industry, academic institutions, nongovernmental organizations (NGOs), and professional associations in charge of educating the public about pharmacotherapy monitoring and rational medication use.
Pharmacovigilance in Disease Control Public Health Programmes:
Concern has been raised about the monitoring of medication safety in nations lacking regulatory or safety monitoring systems, as well as in isolated locations with inadequate infrastructure or health care surveillance. The issues are particularly noticeable when it comes to the usage of medications in particular communities, such as when treating HIV/AIDS and tuberculosis, or when treating tropical diseases like malaria, leishmaniasis, and schistosomiasis. Every nation with a public health disease control program should prioritize pharmacovigilance. [31]
International Response to Drug Safety Issues
Some safety concerns are probably going to affect the entire world, with potentially detrimental effects on public health. A coordinated worldwide assessment and response are required when this occurs. Clinical pharmacologists, regulators, academics, epidemiologists, and representatives from a wide range of medical specialties make up the independent advisory council that the WHO has backed. This panel's duties will include advising WHO on matters pertaining to medication safety, including its Collaborating Center for International Drug Monitoring, and communicating that advice to WHO Member States. [32]
Clinical Trials in India:
India's clinical research space and prospects are highly appealing, which has made it a favourite location for clinical trials for multinational pharmaceutical companies [33].
Some of the advantages for clinical trials that India has as are as follows:
Scientific viability, medical infrastructure, clinical trial experience, regulations, commercialization potential, and cost competitiveness are some of the growth drivers that have led to the recent transformation of Indian clinical research, according to a recent report from the Federation of Indian Chambers of Commerce and Industry (FICCI) [35]. Compared to the more recent arrivals in the market, Indian-born contract research organizations (CROs) were able to offer the advantages of having a better awareness of the Indian scenario, offering services at more affordable pricing, and having greater knowledge of investigator locations around the nation. Some of the primary factors driving the expansion of clinical research in India are the country's current supportive regulatory environment and international-standard rules, as well as rising clinician awareness of and adherence to good clinical practice guidelines [36,37]. The therapeutic area wise distribution of clinical trials and availability of diverse patient population across major therapeutic segments in India is shown in Figure 3 [38].
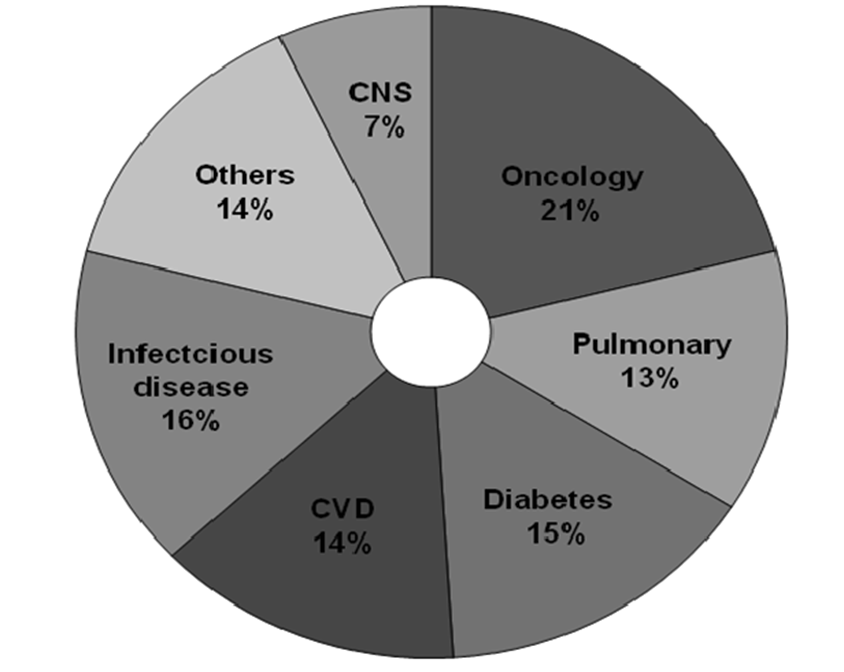
Fig No. 4. Therapeutic area wise distribution of clinical trials outsourced to India
SWOT Analysis of Indian Clinical Trial Sector:
Strengths:
A sizable population of approximately 1.2 billion, or roughly 16% of the global population; A robust biotech and pharmaceutical industry with a large pool of highly qualified workers.
With 500 distinct active medicinal compounds, they are the third-largest players globally.[39]
Currently ranks fourth in the world and contributes 8% of global pharmaceutical production.[40]
The government's supportive measures to capitalize on India's inventive potential.
Due to the big population, there is a lot of data mining about the safety profile of pharmaceuticals. [41]
Weaknesses:
According to projections from 2009–10, spending on the health sector accounted for 2.1% of the overall budget and 0.35 percent of India's GDP [42]. The United States, France, Switzerland, and Germany are examples of developed nations that spend approximately 16%, 11%, 10.8%, and 10.4% of its GDP, respectively. Programs and challenges of national relevance, including PV, are being implemented with less financing [43].
Opportunities:
With 4635 culturally and anthropologically distinct populations, India is the largest source of human biodiversity. It is also a perfect model for studying the efficacy, disease susceptibility, etiology, molecular pathology, and safety profile of drugs in relation to genetic diversity. More than 300 medical, 230 dental, 830 pharmacy, and more than 650 recognized nursing colleges in India provide excellent potential for skilled human resources needed for an efficient PV system [44].
Threats:
Role Of Pharmacogenomics In PV
Pharmacogenomics (PGx) integrates annotated knowledge of genes, proteins, and single nucleotide polymorphisms (SNP) with conventional medicinal sciences like biochemistry. It is the technology that addresses how genetic diversity affects a patient's reaction to medication by linking single-nucleotide polymorphisms (SNP) or gene expression to the toxicity or effectiveness of a medication. By doing this, PGx hopes to create logical ways to maximize medication therapy while taking into account the patient's genotype in order to guarantee optimum effectiveness and few side effects.[45] With these methods, "personalized medicine"—drugs and drug combinations tailored to each person's particular genetic composition—is a reality. The study of a few uncommon and occasionally coincidental severe reactions (phenotypes) seen in certain people gave rise to the field of pharmacogenetics (PG). These characteristics were caused by hereditary illnesses, aberrant medication reactions, or other environmental influences [46].
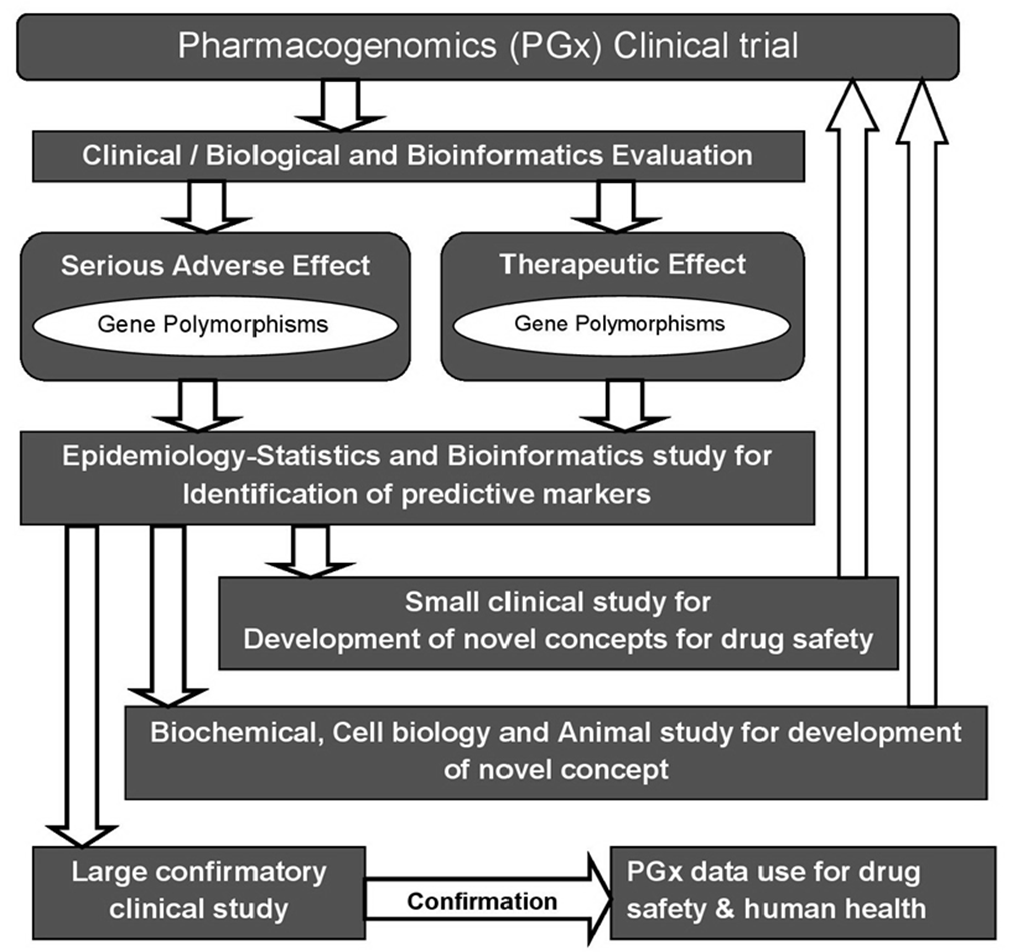
Fig No. 5. The Pathways of Pharmacogenomic Research in Clinical
Find the gene for disease risk:
The main focus of PG is on the positive and negative impacts that medications, poisons, and other substances and environmental elements can have on people. Soon after the discipline of PG was established, however, this focus was expanded, and genetic polymorphisms were thoroughly investigated as susceptibility factors for diseases in general as well as in connection to known specific exposures. The conditions that caused the sickness were unknown in several of these trials. Simultaneously, the functional makeup of the genes taken into account in PG research expanded beyond enzymes that metabolize drugs to nearly every other class, including drug transport, DNA repair, cell cycle regulation, and signal transduction. A meaningful summary of the research on the hundreds of candidate genes as disease susceptibility factors is impossible due to the fact that the total number of publications examining PG polymorphisms in relation to disease risk is many times greater than those examining polymorphisms in relation to drug response. The identification of genotypes predisposing to certain multifactorial and polygenic disorders was the main goal of all recent genome-wide screenings, rather than the response to medication.[47]
Data Mining For PV
PV, sometimes referred to as drug safety surveillance, is the study of improving patient safety and care with regard to medication use by gathering, tracking, analyzing, and evaluating data from patients and healthcare professionals. According to that perspective, PV can be separated into two phases: premarketing surveillance, which gathers data on adverse drug reactions (ADRs) from preclinical screening and phases I through III clinical trials, and postmarketing surveillance, which gathers data during a drug's postapproval phase and during its entire life on the market. [48] PV has historically relied on biological experiments or the manual review of case reports, but because of the large amounts and complexity of data that need to be analyzed, computational techniques that can quickly and accurately identify ADRs have become essential to PV. Computerized ADR detection methods now rely on extensive clinical data sets, such as electronic medical record (EMR) databases, and large-scale compound databases that contain genomic, bioassay, and structure information [49].
Premarketing surveillance:
Early in the medication development process, PV has been used to forecast or evaluate possible adverse drug reactions. Using preclinical in vitro Safety Pharmacology Profiling (SPP) to test substances using cellular and biochemical tests is one of the basic techniques. According to the theory, a compound's activity may result in the potential development of an adverse drug reaction (ADR) in humans if it binds to a specific target. However, in terms of cost and efficiency, experimental detection of ADRs is still difficult. Many studies have focused on creating computational methods to forecast possible adverse drug reactions (ADRs) based on screening data or preclinical properties of the compounds. The majority of current research falls into one of two categories: methods based on chemical structure or protein targets. The integrative approach has also been investigated by others.[50]
Post-marketing surveillance:
The Food and Drug Administration (FDA) screens drugs thoroughly before approving them, but many adverse drug reactions (ADRs) may still go unnoticed because clinical trials are frequently brief, small, and biased by excluding patients with comorbid conditions. It is crucial to maintain postmarket surveillance since premarketing trials do not accurately reflect real clinical use scenarios for a variety of (such as inpatient) populations. In the post-market examination of recently produced medications, PV is crucial [51,52] Before a new drug is introduced to the market, a thorough research and development process is facilitated by the competition among pharmaceutical companies and strict regulatory evaluation procedures. For postmarketing PV, there are numerous distinct data sources available [53]. The examination of "signals" is the foundation of PV research. Signals are defined by the World Health Organization (WHO) as unreported claims about a direct correlation between a drug's ability to cause adverse events and its effects on human organisms [54]. Researchers and clinicians use spontaneous reporting systems (SRS) to create extensive signal datasets. There are already electronic SRSs in place in the US and a few European nations. Similarly, a number of additional options are being carefully investigated, including post-market research, prescription tracking, and study of general practitioners' databases. However, most data is not publically accessible to researchers, which significantly restricts signal discovery when combined with additional obstacles [55–57]. The detection method primarily depends on the doctor's ability to identify a certain trait as a drug adverse event, even if pharmaceutical corporations are obligated to monitor and handle adverse occurrences reported by physicians, attorneys, or patients. Although the issue of gathering and sifting ADR data from numerous dispersed nodes has previously been examined, researchers are still looking for the most effective ways to explore the abundance of data gathered in combination with other post-drug administration inputs [58]. PV researchers now have to deal with the challenge of providing knowledge-oriented tools and services that take advantage of the volume of data gathered, while data and text-mining techniques are sifting through millions of electronic medical records. The proper investigation of these data will ultimately lead to better drug evaluations, which are essential for researchers, regulatory bodies, and pharmaceutical companies [59].
Spontaneous Reports:
An unsolicited report that describes one or more adverse drug reactions (ADRs) in a patient who received one or more medications and is not the result of a study or other structured data collection plan is sent to a business, regulatory body, or other organization by consumers or medical professionals. Once a drug is on the market, spontaneous reports are crucial in identifying safety signals. Rare adverse events that were missed in previous clinical trials or other pre-marketing studies can frequently be reported to a company [60, 61]. One crucial method for obtaining safety data for early detection is the spontaneous reporting of adverse events and ADRs. Such a system's collection of case reports serves as the information source with the least amount of proof and the greatest degree of doubt about causality. The benefits of spontaneous reporting include being accessible as soon as a new product is put on the market, continuing indefinitely, and covering every patient taking the medication. It is the most reliable technique for finding novel, uncommon ADRs and regularly produces safety flags that require additional investigation. [62] The primary drawbacks are under-reporting, which is erratic, sensitive to reporting stimuli, and challenging to measure, as well as the challenge of identifying previously unidentified reactions, especially those that are not typically considered ADRs. It normally does not confirm assumptions; but scenarios arise where spontaneous reporting data alone allow inferences that a signal truly represents a true ADR [63].
Yellow Card Scheme:
Systems for spontaneous reporting were subjected to yellow card schemes (YCS). The thalidomide disaster led to its establishment in 1964. The system has since grown to be one of the most important global PV resources [64].
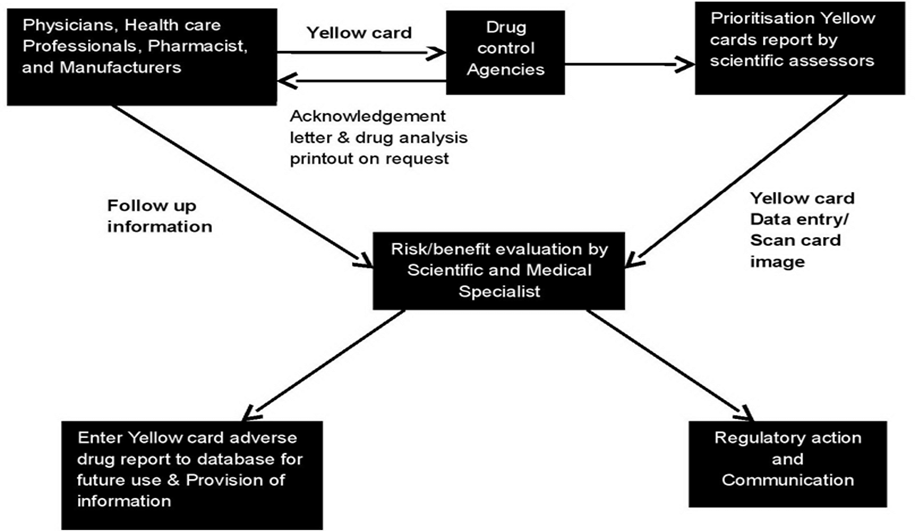
Fig No. 6. Adverse drug reaction online information tracking and yellow card system sources of data.
The YCS is run jointly by the Medicines Control Agency (MCA) which is the regulatory agency and the Committee on Safety of Medicines (CSM) which is the experts committee. Since 1991, the YCS has been enhanced by a new computer system, the ADROIT (Adverse Drug Reaction Online Information Tracking) system. ADROIT is different from other databases. Not only does it store the details of the report, but also the image of the yellow card in the optical system. Multiple users can view any yellow card on screen at the same time. The reports are prioritized so that serious adverse drug reactions receive early attention [65].
Detection and reporting:
A PV center receives a report of suspected adverse drug reactions (ADRs) involving one or more pharmaceutical items from a healthcare provider or marketing authorization holder. Reports can be submitted electronically, over the phone, on written report forms, or in any other authorized manner [66]. Serious responses should be dealt with the highest priority. Potential signals are found in the database, and data is analyzed to elucidate risk variables, apparent changes in reporting profiles, etc. [67] Methodical techniques have been employed to identify safety signals from unplanned reports. These techniques involve using Bayesian and other signal identification methods, as well as calculating the proportional reporting ratio. Drug-drug interactions have also been investigated using data mining techniques [68] Data mining techniques should always be used in conjunction with, and not in place of, analyses of single case reports. Data mining techniques facilitate the evaluation of spontaneous reports by using statistical methods to detect potential signals for further evaluation (Figure 6).
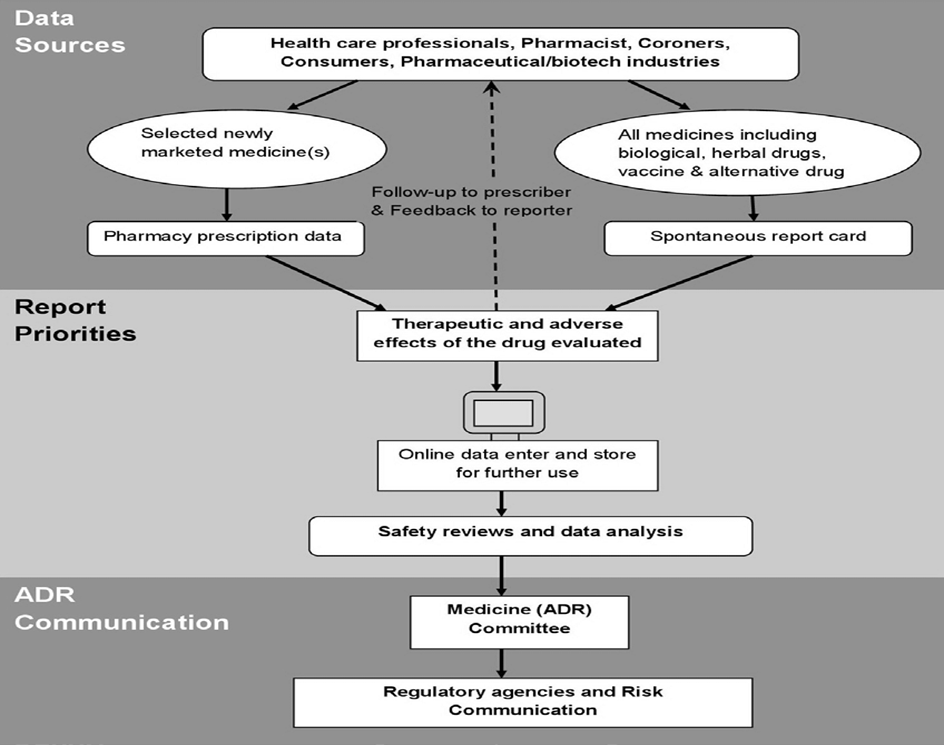
Fig No. 7. Pharmacovigilance systematic methods for the Evaluation of spontaneous reports collected from different data sources.
When comparing medications, care should be taken because this tool does not measure the level of risk. Additionally, the threshold set for signal detection should be taken into account when employing data mining techniques, as this will affect the method's sensitivity and specificity (high threshold is associated with high specificity and low sensitivity). Data mining does not eliminate confounding variables that affect spontaneous adverse event reporting. Data mining findings should be understood in light of the spontaneous reporting system's shortcomings, particularly the wide variations in ADR reporting rates between medications and the numerous potential biases that come with spontaneous reporting. It is important to consider the potential for false positives while evaluating any signals. Furthermore, the lack of a signal does not imply that there is no issue.[69]
PV In India
Since the idea of medication surveillance was not previously established in India, consideration of ADR surveillance emerged relatively late. Despite its youth, PV is not a novel concept in India. It wasn't until 1986 that a small number of doctors, mostly from academic institutions, demanded that more focus be placed on the possible negative effects of prescription drugs and the prudent prescription of medications. As a result, the first ADR monitoring program was established, with 12 regional centers serving 50 million people each. However, this program was a failure [70] Not much occurred until 1997, when India became a member of the WHO Adverse Drug Reaction Monitoring Programme, which is headquartered in Uppsala, Sweden. Three ADR monitoring centers were found, most of which were situated in teaching hospitals: two WHO special centers in Mumbai (KEM Hospital) and Aligarh (JLN Hospital, Aligarh), as well as a National Pharmacovigilance Center housed in the Department of Pharmacology at the All India Institute of Medical Sciences (AIIMS), New Delhi. These centers were required to notify India's drug regulatory body of ADRs. These centers primary responsibility was to keep an eye on adverse drug reactions (ADRs) to medications sold in India. They were non-functional, nevertheless, because prescribers were never informed about the necessity of reporting adverse drug reactions (ADRs) or the operations of these monitoring centers, and the government did not provide adequate funds. After this failed attempt, the WHO-sponsored and World Bank-funded National Pharmacovigilance Program (NPVP) for India was created once more on January 1, 2005 [71]
The challenges of PV in India:
The PVPI's largest problem is the egregious underreporting of negative consequences. This is due to a number of factors, such as a lack of medical knowledge regarding medicine administration, a shortage of qualified personnel in PV, and a lack of awareness of PV across the country. The additional difficulties are infrastructure that is still conservative, a long gap between regulations and guidelines, a traditional approach to the development of new drugs, and virtually nonexistent PV and regulatory inspections. Given that India has a highly developed IT sector, the system needs to be improved with the assistance of PV specialists working in tandem with IT. Given that PV handles a lot of ADRs, it would be prudent for PV specialists to work with software specialists to create and construct a reliable system. The software applications that are created can be utilized. for gathering and analyzing data sets, identifying patterns in drug use across different disease domains, compliance, prescription mistakes, and drug interactions that result in adverse drug reactions. Furthermore, it has been worthwhile for the DCGI to invest in a strong PV system to allow assessors and decision-makers to evaluate safety data and make regulatory decisions without relying on other nations, as more clinical research and PV outsourcing work is currently being carried out in India [72] ADRs may be the cause of many patient deaths, but occasionally the doctors do not recognize them at the time of admission. ADRs also have a significant financial impact on the healthcare system [73] The primary cause of exposure to adverse drug reactions (ADRs) is people self-medicating and switching from prescription-only medications (POM) to over-the-counter (OTC) more frequently when new medications are introduced to the market without extensive safety assessments conducted by regulatory bodies. Drug manufacturers and regulatory bodies in India used long-term usage data to inform their safety evaluations in the past. Many Indian businesses have been investing more in R&D in recent years, strengthening their ability to create and sell novel medications through in-house research. New information will be produced after a product is marketed, and this could affect the product's benefit-risk profile. To guarantee the safe use of all products, a thorough assessment of the new data produced by PV activities is crucial. Therefore, DCGI needs to make some difficult choices and pledge to impose PV as a requirement and establish a PV inspection culture.[74]
Future prospects:
PV systems that can identify novel ADRs are becoming more and more necessary, and regulatory measures are required to safeguard public health. The creation of information that can help a patient or healthcare provider make decisions has received little attention. One of PV's main objectives is to collect and disseminate this data. [75] Information regarding the security of active drug surveillance is required. It is crucial to gather comprehensive and precise data on each significant reported event when creating new techniques for active post-marketing surveillance. Although spontaneous reporting is a good way to generate signals, it is less effective in identifying patient features and risk factors because of the comparatively small number of reports collected for a given association. [76] Additionally, PV techniques need to be able to identify whether patients are susceptible to an adverse drug reaction. The PV approach would be in line with the expanding patient base as a source of information. participation in medication safety. Finding personal risk factors for the occurrence of specific ADRs may be a function of the PG. PV must focus on patients as a source of information going forward, in addition to more conventional groups like medical professionals. To help assure regulatory compliance, improve clinical trial safety, and improve post-marketing surveillance, the DCGI should move swiftly to improve PV and incorporate Good Pharmacovigilance Practice (GPP) into the processes and procedures. A functional PV system is necessary for the careful use of medications. Consumers, pharmaceutical businesses, regulatory bodies, and healthcare professionals will all gain from it. It assists pharmaceutical corporations in keeping an eye on the risks associated with their medications [77] PV post-marketing is currently a difficult and time-consuming procedure for regulatory bodies as well as the industry as a whole. The purpose of the PV is to get the information, documentation of the work and expertise online while giving attention to the new and important safety issues. While less relevant than major events, non-serious ones are nonetheless crucial for comparing health changes, even though they are regularly examined as well. [78] By combining disproportionality and data visualization tools with conventional, case-based PV techniques, GlaxoSmithKline has developed a potent new strategy for PV in the modern era. These tools are part of a system structure that makes knowledge management, safety issue monitoring, and in-stream review easier [79]. By increasing efficiency and offering new analytical capabilities, this highly inventive instrument and the procedures will contribute to the advancement of PV. Pharmaceutical businesses may use a similar strategy to quickly identify and analyze ADRs. Transparency and communication would increase consumer reporting, which are excellent steps towards incorporating consumers more in PV.
CONCLUSION
In order to ensure the efficacy and safety of pharmaceutical products, pharmacovigilance is at the forefront, and recent developments demonstrate its dynamic evolution. Revolutionary changes in the field have been facilitated by advancements in technology, a growing focus on real-world data, and a movement toward patient-centered care. Pharmacovigilance has expanded beyond conventional clinical settings with the use of empirical data made possible by the application of numerous data sources, including as electronic health records and pragmatic trials. Pharmacovigilance is still essential for addressing the problems caused by the growing variety and strength of medications, each of which has an unavoidable and occasionally unanticipated risk of side effects. When toxicity and negative consequences do manifest, particularly when they were previously unidentified, it is crucial that they be documented, examined, and their importance clearly conveyed to the audience so they are equipped to understand the data. The community may benefit from the adverse events reported by the PV system because of their closeness to the general public and public health professionals, who are able to communicate easily with reporters via phone, email, and text messages on mobile devices and have a language understanding of patient lifestyles and habits. Individuals' health and well-being are positively impacted by the creation of novel and efficient pharmaceutical items. To increase their contribution to public health, PV systems must be improved in order to monitor and address medication safety concerns more successfully. Therefore, industry, drug regulators, physicians, and other healthcare professionals share responsibility for PV for medical product safety in order to assist patients recover and manage their conditions as best they can, or ideally, prevent disease. Future initiatives and funding should contribute to a more extensive PV industry in India. To overcome obstacles, promote innovation, and guarantee the ongoing enhancement of pharmacovigilance procedures, the interdependent network of stakeholders—which includes regulatory bodies, pharmaceutical firms, medical professionals, and patients—must keep cooperating. Pharmacovigilance continues to play a crucial role in protecting public health by keeping an eye on and responding to the ever-changing environment of drug safety as it adjusts to these current trends.
REFERENCES



Kunal G. Kothawade*, Akshay R. Wagh, Anjali G. Kute, Sakshi S. Jadhav, Dr. A. B. Darekar, Pharmacovigilance: A Comprehensive Review of Drug Safety Monitoring Practices, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 8, 2523-2544 https://doi.org/10.5281/zenodo.16932824
 10.5281/zenodo.16932824
10.5281/zenodo.16932824