
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Quality Assurance Technique, R. G. Sapkal College of Pharmacy, Anjaneri, Nashik
Principal of KCT'S R. G. Sapkal College of Pharmacy, Anjaneri, Nashik
Professor at KCT'S R. G. Sapkal College of Pharmacy, Anjaneri, Nashik
“Diabetes mellitus” is one of the most prevalent non-communicable diseases in the world. Diabetes mellitus is the most common endocrine disorder that impairs the body's capacity to produce or utilize insulin. Conventionally, diabetes has been divided into three types, Type 1 DM, or insulin-dependent diabetes mellitus (IDDM), in which the body fails to produce insulin and presently requires the person must inject insulin or use an insulin pump. This is also termed "juvenile diabetes." Type 2 DM, or non-insulin-dependent diabetes mellitus (NIDDM), results from insulin resistance, a condition in which cells fail to use insulin properly, with or without an absolute insulin deficiency. This type was previously referred to as "adult-onset diabetes." The third main type is gestational diabetes, which occurs when women without a previous history of diabetes develop a high blood glucose level during their pregnancy. It may precede the development of type 2 DM. A person with diabetes mellitus (DM), also known as simply diabetes, has an excessive blood sugar level over a prolonged period due to chronic metabolic diseases caused by insufficient insulin production by the pancreas or ineffective insulin uptake or response by the body's cells. People managing diabetes encounter a number of obstacles, such as the disease's increasing incidence in both urban and rural areas, low disease knowledge, a shortage of medical facilities, expensive treatment, inadequate glycemic control, and an increase in the frequency of diabetic complications. Typically, subcutaneous injections are used to deliver insulin therapy for diabetes, up to four times per day. Long-term insulin therapy has led to issues with patient compliance, which has an impact on patient outcomes. These issues are further exacerbated by the intrusive nature of insulin delivery. Type 2 diabetes mellitus, which accounts for more than 90% of all diabetes occurrences, is the primary cause of the diabetic epidemic, while type 1 diabetes incidence is also on the rise. Together with additional risk factors like obesity and a sedentary lifestyle, type 2 diabetes is a dangerous and prevalent chronic illness that is brought on by a complicated interaction between heredity and environment.
Diabetes mellitus (DM), also referred to as "sugar,” and it is the most prevalent endocrine disorder. It typically arises from an insufficient or absent insulin supply or, in rare cases, from impaired insulin action (insulin resistance) [1]. The pancreas secretes both the hormones glucagon and insulin. beta (ß) cells secrete insulin while alpha (?) cells secrete glucagon, both are situated in the islet of Langerhans[2]. Insulin lowers blood glucose levels via glycogenesis and transports glucose to the muscles, liver, and adipose tissue[3]. Insulin aids in transporting glucose (blood sugar) from the bloodstream to the cells, where it may be broken down and used for fuel[4]. Insufficiency or inadequate synthesis of pancreatic insulin results in an increase or decrease in glucose concentrations in the blood, causing hyperglycemia. It has been discovered to harm several body systems, including the blood vessels, eyes, kidneys, heart, and nerves[5].
Diabetes mellitus has been classified into: insulin-dependent diabetes mellitus (IDDM, Type 1 DM), non-insulin-dependent diabetes mellitus (NIDDM, Type 2 DM), gestational diabetes mellitus, and other specific types[6]. Type I diabetes is an autoimmune condition marked by a local inflammatory response in and around the islets, followed by the selective destruction of insulin-secreting cells[7]. T1DM occurs when pancreatic cells are unable to produce adequate insulin[8]. whereas Type II diabetes is characterized by peripheral insulin resistance and decreased insulin secretion[7].T2DM causes insulin resistance, which is when cells do not effectively respond to insulin[8].T2DM accounts for 80% to 90% of all diabetes cases[9]. GDM develops when pregnant women without a history of diabetes have high blood sugar levels. T1DM can be managed with insulin injections. T2DM treatment entails a good diet, weight management, and physical activity[8].
Diabetes increases the risk of various consequences, including cardiovascular and peripheral vascular disorders, stroke, neuropathy, renal failure, retinopathy, blindness, and amputations[10].Type 1 diabetes symptoms include polyuria (frequent urination), polydipsia (increased thirst), polyphagia (increased hunger), and weight loss[11]. The World Health Organization (WHO) has just declared it a pandemic[12]. According to WHO forecasts, the number of diabetic patients globally will increase from 171 million in 2000 to 366 million by 2030[13]. India has been called “the diabetes capital of the world” due to its high diabetes rates. Approximately 41 million Indians suffer from diabetes, accounting for one-fifth of all diabetes cases globally[14].
Drugs are employed primarily to save lives and treat symptoms. Secondary goals include preventing long-term diabetic problems and increasing longevity by removing various risk factors. Insulin replacement therapy is the mainstay for individuals with type 1 diabetes, but diet and lifestyle adjustments are considered the cornerstones for the treatment and management of type 2 diabetes[15]. Diabetes can be treated with a variety of hypoglycemic medications, including biguanides and sulfonylureas. However, none of these drugs is perfect because of their toxic side effects, and a reduction in responses is sometimes noted in their continuous usage[16].However, none of these drugs is perfect because of their toxic side effects, and a reduction in responses is sometimes noted in their continuous usage[17].
Etymology
The terms "Diabetes" and “Mellitus” are derived from Greek. The term “Diabetes” means "a passer through; a siphon" whereas the "Mellitus" means "sweet". It is believed that the Greeks named it such because the enormous amounts of urine produced by diabetics attracted flies and bees. In ancient China, diabetes mellitus was diagnosed by examining whether or not ants were attracted to a person's urine. In medieval times, European doctors diagnosed diabetes by tasting their own urine, which is occasionally shown in Gothic beliefs[18].
Types of DM
The first widely accepted classification of diabetes mellitus was published by the WHO in 1980[19] and it is modified in the year 1985[20].The classification includes both clinical phases and aetiological kinds of diabetes mellitus, as well as other hyperglycemic classifications[21].
The previous and new terms of insulin-dependent (IDDM) or non-insulin-dependent (NIDDM), suggested by WHO in 1980 and 1985, have disappeared and terms of the New Classification The system recognizes four forms of diabetes mellitus: type 1(IDDM), type 2(NIDDM),“other specific types” and gestational diabetes (WHO Expert Committee 1999). These were incorporated in the subsequent International Nomenclature of Diseases (IND) in 1991, and the tenth revision of the International Classification of Diseases (ICD-10) in 1992[21]. Hence, classification of diabetes mellitus is as follows:
Type 1 diabetes is also known as autoimmune diabetes and was previously referred to as juvenile-onset or ketosis-prone diabetes[22,23,24]. Type I diabetes mellitus is also called as insulin-dependent diabetes mellitus (IDDM), this happens primarily in children and young people; the onset is typically rapid and can be life-threatening[2,23]. Type 1 diabetes (due to the destruction of beta-cell which is usually leading to absolute insulin deficiency) (American Diabetes Association, 2014). Insulin production is severely reduced or absent as a result of the loss of pancreatic ß-islets cells. Treatment with insulin injections is required [2,25]. When fasting diabetic hyperglycemia is first discovered, 85-90% of persons with Type 1 diabetes mellitus have immune destruction markers, such as islet cell auto-antibodies, insulin auto-antibodies, and glutamic acid decarboxylase (GAD) auto-antibodies[26]. The actual origin of diabetes mellitus is still unknown, however in most people, there is evidence of an autoimmune process involving auto-antibodies that kill the beta islet cells[2]. A high sugar level in the blood can cause both short term and long-term complications. T1DM is a chronic metabolic condition marked by the inability to produce insulin. Glucose from your food cannot enter cells, resulting in higher concentration in the bloodstream. About 10% of people suffer with type1 diabetes[27].
Type 2 diabetes is also known as "Non-Insulin-Dependent Diabetes Mellitus" (NIDDM) or "adult-onset diabetes”[28]. In type 2 diabetes, the body either does not produce enough insulin to meet its own specific challenges or the cell does not respond effectively to insulin. This is referred as insulin resistance[29,30]. People with this kind of diabetes commonly have insulin resistance[31].The long-term complications in blood vessels, kidneys, eyes and nerves occur in both types and are the primary causes of morbidity and death from diabetes[32]. The causes are multifaceted, and predisposing factors include obesity, sedentary lifestyle, rising age (affecting middle-aged and older adults), and genetic factors[1]. Such patients are at an elevated risk of developing macrovascular and microvascular difficulties[33,34].
Gestational diabetes mellitus (GDM) is a kind of glucose intolerance that develops or is diagnosed during pregnancy[1]. Women who develop Type 1 diabetes mellitus during pregnancy and women with undetected asymptomatic Type 2 diabetes mellitus that is identified during pregnancy are classed as Gestational Diabetes Mellitus (GDM)[35]. Gestational diabetes mellitus (GDM) (diabetes diagnosed during pregnancy that is not clearly over diabetes)[22]. The gestational diabetes mellitus may develop throughout pregnancy and may subside after delivery; In the long run, children born to women with GDM are at higher risk of obesity and type 2 diabetes in later life, a condition related to the consequences of intrauterine exposure to hyperglycemia.
It is also caused by genetic anomalies in insulin hormone secretion within the body. Mutations cause it to affect 1 to 5% of those who have experienced it. This includes pancreatic disorders, some surgeries, genetic problems in beta cells, cancer treatments, drugs, infections, and so forth. Some medications are used or combined with the treatment of HIV/AIDS or organ transplantation [36].
It has three sub-types: MOODY, LADA, and Endocrinopathies.
MODY
MODY (maturity onset diabetes of young)[23]. They may or may not be required insulin. MODY is inherited diabetes mellitus caused by a genetic mutation in an autosomal dominant gene that alters insulin secretion or production; it is not an insulin-dependent diabetes. Individual diagnosis is often in children less than the age of 25 with hereditary variables. The HNF1-Alpha (Hepatocyte Nuclear Factor) gene is responsible for approximately 70% of instances of MODY[37]. It is associated with a genetic impairment of the ?-cells. This kind causes hyperglycemia at a young age. They are clinically similar to T2DM.
LADA
LADA refers to latent autoimmune diabetes in adults. Insulin is not necessary for months or years after diagnosis. They do not create any insulin, and it is clinically identical to T1DM. LADA arises when pancreas cells stop producing insulin. LADA occurs in young adults in their twenties and might be misdiagnosed with type 2 diabetes mellitus due to age[38]. Type1DM differs from LADA.
Endocrinopathies
Several hormones either stimulate or decrease insulin action. Impaired fasting blood glucose is characterized by an FBG higher than 100mg/dl but less than 126 mg/dL[38]. It may include polycystic ovarian syndrome, pancreatic cancer or tumours, and other hormonal Disruptions in insulin production.
Signs and Symptoms
The signs and symptoms of diabetes mellitus. This is why diabetes is called the silent killer. It is crucial to remember that these symptoms can be misinterpreted as an ailment or another sickness. The most commonest and typical symptoms of diabetes are as follows [39,40]:
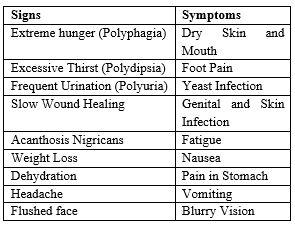
Other Symptoms include:
Other sign include, sexual dysfunction in men, vaginal infections in women, numbness or tingling in hands and feet, itchy or flaky skin, skin and yeast infections plus frequent gum and bladder infections.
COMPLICATIONS
As the disease progresses tissue or vascular damage occurs leading to severe diabetic complications such as retinopathy with potential blindness, neuropathy with risk of foot ulcer, nephropathy, which may lead to renal failure, Charcot joint and features of autonomic dysfunctions and sexual dysfunction41, cardiovascular complications and ulceration. Long-term type 1 diabetes patients are susceptible to microvascular problems and macrovascular disease (coronary artery, heart, and peripheral vascular disease)[42,43]. Type 2 diabetes raises the risk of large vessel atherosclerosis, which is often linked to hypertension, hyperlipidemia, and obesity. Cardiovascular problems and end-stage renal disease are the leading causes of death among persons with type 2 diabetes[15].
ETIOLOGY
Chemicals and medications can sometimes cause type 1 diabetes. Its cause’s autoimmune disorders such as Graves’ Disease, Hashimoto’s Thyroiditis and Addison’s disease[23], Which can seriously causes that type of diabetes mellitus. In around 70-80% of cases, the immune system destroys beta cells. In T1DM, the beta cells fail to produce Insulin. T1DM is commonly caused by the destruction of beta-cells. The reason for this autoimmune response is uncertain. T1DM is characterized by Anti-Glutamic acid decarboxylase[44]. The glucose level in the body reduced due to poor insulin usage, which is the major cause of Type 2 Diabetes. It’s also caused by Overeating, smoking, alcoholism, dysfunction of the endocrine & nervous system[45]. 33% of American people suffer from renal disease. African Americans, Latinos, Native Americans, Asian Americans, and Pacific Islanders all face a significant risk of renal disease[46]. T2DM occurs when the body fails to use insulin. Certain traditional tribes have a greater inherited incidence of it. The body produces a hormone known as Insulin that maintains proper blood sugar levels. During pregnancy, the placenta produces greater pregnancy hormones that may interfere with insulin. During pregnancy, the body can produce extra insulin to regulate blood glucose levels. Still, in certain women, the body cannot produce sufficient insulin during pregnancy, and blood sugar levels rise, producing GDM. The main cause of diabetic Retinopathy is blindness, which accounts for 2.6% of global blindness[47].
DIAGNOSIS
Diabetes mellitus diagnosis includes urine sugar, blood sugar, glucose tolerance test, renal glucose threshold, diminished glucose tolerance, increased glucose tolerance, renal glycosuria, extended glucose tolerance curve, cortisone-stressed glucose tolerance test, intravenous glucose tolerance test, oral glucose tolerance test[13].
Diabetes is diagnosed by the folloing blood tests[40]. They are;
This test can diagnose diabetes if there are diabetic symptoms and a blood glucose level of 11.1 mmol/L (200 mg/dl) or above.
Diabetes is diagnosed when the fasting blood glucose level is 7.0 mmol/L (126 mg/dL) or greater on at least two tests. A value of 100-125 mg/dL indicates pre-diabetes. A normal fasting blood sugar level is less than 100 mg/dL.
Diabetes is diagnosed with this test if the two-hour blood glucose level is 200 mg/dl or greater. Pre-diabetes is diagnosed when the two-hour blood glucose level is 140-199 mg/dL.
Blood glucose levels are measured two hours after a meal. Postprandial blood glucose testing is typically performed in persons who have hyperglycemia symptoms or when the results of a fasting glucose test indicate probable diabetes but are inconclusive. Values of 200 mg/dL or higher suggest diabetes.
TREATMENT
Diabetes treatment focuses mostly on controlling blood sugar levels and preventing diabetic complications. Treatment includes medications, a healthy diet, and regular exercise. For the initial treatment of DM, lifestyle modifications and oral anti-diabetic medicines are suggested [48].
A] Drug Treatment
Anti-diabetic drugs treat diabetes mellitus by reducing the blood glucose levels. With the exception of insulin, Exenatide, and Pramlintide, all are administered orally and are thus also called as oral hypoglycemic agents or oral anti-hyperglycemic agents. There are different classes of anti-diabetic drugs, and their selection depends on the nature of the diabetes, age and situation of the person, among other factors[40].
Type 1 Diabetes mellitus is a disease caused by the lack of insulin. Insulin must be used in Type 1 must be injected or inhaled. Type 2 Diabetes mellitus is a disorder of insulin resistance in cells. Treatments include medications that increase the quantity of insulin secreted by the pancreas, drugs that increase the sensitivity of target organs to insulin, and agents that slow the rate of glucose absorption from the gastrointestinal tract[40].
Insulin is commonly administered subcutaneously, either through injections or an insulin pump. Research is underway of other routes of administration. In acute care conditions, insulin may be administered intravenously. There are several types of insulin, distinguished by the rate with which the body metabolizes them. Insulin is required for treating type 1 diabetes. For many years, it was considered that regulating plasma glucose would prevent diabetic complications. The diabetes management and complications trial (American Diabetes Association, 1993) demonstrated that this faith was well founded: Type 1 diabetes patients were randomly assigned to intensive or conventional care[40].
Oral hypoglycemic agents including insulin are used in the treatment of type 2 DM and those agents includes Sulfonylureas, Alpha glucosidase inhibitors, Biguanides and Thiazolidinediones.
The main goal is to treat metabolic disorders such as insulin resistance and inadequate insulin secretion.
Sulfonylureas were the first commonly used oral hypoglycemic drugs. They are insulin secretagogues, which cause insulin release by directly acting on the KATP channel of pancreatic beta cells. Examples include Glimepiride, Glibenclamide, Chlorpropamide, Glipizide, Glyburide etc.
Meglitinides, also known as "short-acting secretagogues," aid in the production of insulin by the pancreas. Their mode of action is original, affecting channels. By shutting the potassium channels of pancreatic beta cells, they open the calcium channels, thus increasing insulin release. Examples include Repaglinide, Nateglinide, Nateglinide.
Biguanides decrease hepatic glucose production while increasing glucose absorption by the periphery, which includes skeletal muscle. Although it must be used with caution in patients with impaired liver or kidney function, motorman has become the most commonly used agent for type 2 diabetes in children and teenagers. Examples include Metformin, Phenformin, Buformin.
Thiazolidinediones (TZD) or glitazones , belong to the medications of type II diabetes. Their chemical structure includes the thiazolidine group, which is responsible for the major action of these active substances. Their mode of action involves the activation of peroxisome proliferator-activated receptor (PPAR gamma), a nuclear receptor. This activity alters the transcription of numerous genes that contribute to glucose and lipid metabolism, as well as energy balance. The main TZD derivatives are pioglitazone, rosiglitazone, and lobeglitazone.
Alpha-glucosidase inhibitors, also known as "diabetes pills", are not considered hypoglycemic medicines because they do not directly affect insulin secretion or sensitivity. They are primarily administered to patients orally in order to reduce blood glucose levels. Alpha-Glucosidase Inhibitors inhibit alpha-glucosidase enzymes that convert polysaccharide carbohydrates into monosaccharides in the upper gastrointestinal system. These medications reduce the absorption of glucose. Acarbose was the first medicine approved by the FDA in 1995, with miglitol following in 1996. Their application is limited because they must be administered in numerous daily dosages, and some gastrointestinal (GI) side effects have been reported.
Incretins consist a group of hormones (the two main are GLP-1 and glucose dependent insulinotropic peptide) produced by GI that increase insulin secretion in a glucose-dependent manner. Both GLP-1 and GIP are quickly deactivated by the enzyme dipeptidyl peptidase-4 (DPP-4).
GLP agonists bind to membrane GLP receptors. This leads to increased insulin release from pancreatic beta cells. Endogenous GLP has a half-life of only a few minutes; consequently, an analogue of GLP is not practicable. Examples include Exenatide, Liraglutide.
Dipeptidyl peptidase-4 (DPP-4) inhibitors are new class of oral diabetic agents that help in weight loss as well as blood sugar control. They act by an enzyme which destroys a group of gastrointestinal hormones known as incretins. DPP-4 inhibitors are prescribed for type 2 diabetic patients who do not respond well to metformin and sulphonylureas[49].
These are injectables used to treat both type 1 and type 2 diabetes and are administered before meals. They inhibit the release of glucagon while eating, which slows the food emptying from the stomach. Pramlintide acetate (SYMLIN) is the class of drug available in US which is administered by subcutaneous injections. In the UK, it is not approved by National Institute for Health and Care Excellence (NICE) because it can significantly raise the risk of severe hypoglycemia[49].
B] Non-Drug Treatment
Low-calorie, low-sugar, high-protein, high-fiber, and moderately fat-rich foods should be provided, as well as a sufficient quantity of vitamins (mostly vitamins C and E) in the diet. Minerals such as zinc should be prescribed in this scenario[50].
Adequate caloric value and dietary management should be taken properly by the both diabetic and non-diabetic patient such as:
Exercise's Impact on Physical, Mental, and Social Health. Exercise helps to reduce blood glucose levels. Regular exercise also helps to maintain healthy body weight and control high blood pressure and high blood cholesterol levels[52]. This, in turn, helps to minimize the risk of associated health disorders such as cardiovascular disease. Sitting still (i.e. being sedentary) for long periods is a risk factor for T2DM. You should strive to get up periodically and move around for a few minutes[51].
Lifestyle modification is defined as a way of living that has been transformed in a variety of ways. Lifestyle has seven elements of excellent diabetes care, including: knowing more about diabetes, obtaining regular diabetes care, learning how to control your diabetes, preventing long-term diabetes problems, getting examined for long-term problems and treating them, and so on[40].
HERBAL TREATMENT
Plant-based medications that are eco-friendly, bio-friendly, cost-effective, and reasonably safe have moved from the fringe to the mainstream in recent decades as traditional medicine research has improved[53]. The WHO has recognized 21,000 plants that are utilized for therapeutic purposes worldwide. India is the largest producer of medicinal herbs and is known as the world's botanical garden[54].
According to ancient literature, around 800 plants are reported to have anti-diabetic qualities[55]. Ethnopharmacological surveys show that over 1200 herbs are utilized in traditional medicine for their putative hypoglycemic properties[56]. Since time immemorial, medicinal plants have been employed as a source of medicine in almost all cultures[40]. Plants-based products have been popular all across the world for the centuries. Some herbal alternatives in diabetes have been shown to provide symptomatic relief and assist in the prevention of secondary problems of the condition. Some herbs have also been shown to help regenerate ß-cells and overcome resistance. In addition to maintaining normal blood sugar levels, several herbs are said to have antioxidant and cholesterol-lowering properties. Type 2 diabetes mellitus (NIDDM) can be managed using medications that lower blood sugar levels while also restoring liver glycogen levels. In modern system of medicine, there is no drug, which is reported to possess both of these properties. However, the hypoglycemic impact of various herbal extracts has been established in human and animal models of type 2 diabetes, and conventional medications have been developed using the active components of these medicinal plants. Metformin, a less toxic biguanide and strong oral glucose-lowering drug derived from Galega officianalis, is used to treat diabetes[57]. Out of dozens of oral drugs for diabetes, only one medication (metformin) is licensed for use in children, and it was developed from herbs[58].
PREVENTION
T1DM is unavoidable due to an immune system issue. Most diabetes prevention or treatment techniques include making easy modifications to your diet and exercise routine. Some factors of T2DM, such your genes or age, are beyond your control. However, many additional diabetes mellitus risk factors are controllable. These are not the only approaches to avoid diabetes mellitus. Diabetes Mellitus is a chronic condition with no known cure[59]. Here's what you can do to delay or avoid T2DM,
It may be possible to manage by eating healthy foods, exercising, and maintaining healthy body weight. DOC1
CONCLUSION
Diabetes mellitus is a serious complication in today life. The lifestyle and day today circumstances are play major role in occurring this type of serious complications. In this review we get some idea regarding diabetes mellitus. The above review has given information about Diabetes Mellitus, Types, Signs & Symptoms, Causes, Diagnosis, and Treatment. Diabetes Mellitus become a common disease among children and more severe if no initiative is taken to control it. Diabetes Mellitus is a Non-Curable (Incurable) Disease, but it can handle or Prevent by Insulin Therapy & Anti-Diabetic medicines for a while. Proper diet and exercise for diabetic’s patients is a must. 80-90% of Diabetic Patients suffer from T2DM in India & US. If not appropriately treated, the disease will affect 90– 95% of the World’s population & it will generally appear in people of all age’s in the future.
REFERENCE


Jagruti G. Musale, Dikshita D. Wagh, Rishikesh S. Bachhav, Smita S. Aher, A Review on Diabetes Mellitus, Int. J. of Pharm. Sci., 2024, Vol 2, Issue 7, 107-118. https://doi.org/10.5281/zenodo.12606390
 10.5281/zenodo.12606390
10.5281/zenodo.12606390