
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
R.G Sapkal College of Pharmacy, Sapkal Knowledge Hub, Kalyani Hills, Anjaneri, Trimbakeshwar Rd, Nashik, 422213, Maharashtra, India.
Purpose: This research evaluates Remogliflozin etabonate clinical, pharmacokinetic, and mechanistic data. It then evaluates its therapeutic role in T2DM therapy, particularly in contrast to other reliable SGLT-2 inhibitors. Design/methodology/approach: The researchers followed the PRISMA 2020 standards when they performed the quantitative synthesis and systematic review. The search period for electronic databases included January 2010 through March 2026 and included PubMed, Scopus, Web of Science, and ClinicalTrials.gov. Research including pharmacokinetics, observational safety, and Phase II/III randomized controlled trials was considered. To determine potential bias, researchers used the Newcastle-Ottawa Scale and the Cochrane RoB 2.0 tool. Binary safety outcomes and continuous outcomes (HbA1c, weight, systolic blood pressure) were both modeled using random-effects meta-analytic techniques where applicable. Findings: Quantitative synthesis included fourteen randomized controlled studies. There was low to moderate variability in the results, but pooled analysis showed statistically significant decreases in HbA1c (mean difference ? -0.8%), body weight (? -2.0 kg), and systolic blood pressure (? -3-4 mmHg). There was little hypoglycemia with monotherapy and an increase in genital mycotic infections, both of which are consistent with known class effects in terms of safety. It has been shown that there is short-term metabolic equivalency to well-established drugs like dapagliflozin and empagliflozin, according to comparative analysis. However, definite placement within outcome-driven treatment hierarchies is limited due to the lack of dedicated studies for cardiovascular and renal outcomes. Practical implications: The results provide credence to Remogliflozin's status as a safe and effective short-term glucose-lowering medication. Pending long-term cardiovascular validation, it may have promise as a treatment alternative in developing and resource-limited contexts. Originality/value: Incorporating renal physiology, pharmacokinetics, meta-analytic data, and therapeutic positioning theory, this work presents the first full mechanism-to-outcome synthesis of Remogliflozin. It addresses SGLT-2 evidence asymmetry and promotes drug-class differentiation frameworks by providing class effect vs. agent-specific outcome validation reasons.
1.1 Research Background
The global pandemic of type 2 diabetes mellitus (T2DM) affects public health, socioeconomics, and clinical practice. More than 500 million individuals throughout the globe are living with type 2 diabetes, and experts predict that figure will rise sharply by 2045 as a result of changes in population dynamics, increased urbanization, and the prevalence of obesity [1]. Type 2 diabetes is now understood beyond glucose management. Instead, it is a multisystem cardiometabolic syndrome with complex metabolic, cardiovascular, and renal pathogenesis [2] [3]. Cardiovascular disease (CVD) is still the top killer among people with type 2 diabetes due to the intricacy of the condition.
Improvements in glycated hemoglobin (HbA1c) alone do not adequately reduce the risk of cardiovascular events or renal decline [4], thus, the paradigm of diabetes management has shifted from a glucose-centric approach to an integrated cardiorenal-metabolic framework. According to Siddiqi et al. (2024) and Khan (2025), sodium-glucose cotransporter-2 (SGLT-2) inhibitors are one of the newer types of pharmacotherapeutics that are gaining popularity. They reduce renal glucose reabsorption and increase glucosuria without insulin. These inhibitors improve kidney preservation, hemodynamics, and cardiovascular outcomes systemically. Traditional agents mostly target peripheral insulin sensitivity or pancreatic insulin secretion; these effects are in contrast with them.
Several landmark investigations have confirmed this class's medicinal potential. Empagliflozin substantially lowers cardiovascular and all-cause mortality in high-risk T2DM patients [5]. However, canagliflozin and dapagliflozin enhance renal outcomes and heart failure hospitalization [6] [7]. More recent meta-analyses [3] [8] [9] [10] [11] have shown that SGLT-2 inhibitors reliably reduce heart failure hospitalizations, composite renal endpoints, and CKD progression in various populations and with comorbidities. This findings led the ADA and EASD to propose SGLT-2 inhibitors for type 2 diabetics with co-morbid cardiovascular disease or chronic kidney disease (CKD) regardless of baseline glucose levels [11] [12].
A new oral SGLT-2 inhibitor, Remogliflozin etabonate, has evolved within this family of medicines; it has some molecular similarities with existing drugs but has different pharmacokinetic properties. Consistent with the molecular bases seen in effective SGLT-2 inhibitors, early phase II/III trials show clinically significant improvements in body weight and systolic blood pressure in addition to clinically relevant reductions in HbA1c [13] [14]. Rumor has it that in controlled outpatient settings, there may be advantages for some groups, such those with acute decompensated heart failure (RemoSafe AHF trial) [15], and that the drug is just as safe as dapagliflozin. But unlike other class leaders like dapagliflozin and empagliflozin, the data for Remogliflozin is limited to clinical assessments that were conducted in particular contexts and had shorter durations.
1.2 Problem Statement
Remogliflozin etabonate's literature lacks an integrated synthesis linking its molecular basis to its long-term clinical findings, despite its extensive usage and beneficial benefits. Few large-scale cardiovascular outcome trials like EMPA-REG, CANVAS, or DECLARE-TIMI 58 exist, and most studies focus on short-term metabolic effects or single-center comparisons rather than systemic outcomes or rigorously comparing Remogliflozin to its class. Lack of synthesized data limits evidence-based treatment positioning, especially when formulary decisions are based on comparative value, long-term safety, and cost-effectiveness.
Recent meta-analyses and systematic reviews of SGLT-2 inhibitors have shown that they significantly reduce the risk of MACE, heart failure hospitalization, and chronic kidney disease. Nevertheless, there is a lack of targeted information about drugs such as Remogliflozin, which are being used more often in developing nations and settings with limited resources. In these areas, cost factors and regional clinical profiles may vary greatly from trial subjects in countries with higher incomes.
1.3 Research Gap
Three salient gaps deserve scholarly attention:
For theoretical and clinical development, gaps must be filled. The lack of systematic synthesis makes Remogliflozin's treatment hierarchy unclear, impeding clinician trust and guideline prioritization.
1.4 Research Objectives
Based on gaps, this review aims to:
1.5 Contribution
Unique contributions from this review:
2. THEORETICAL FRAMEWORK AND LITERATURE REVIEW:
2.1 Theoretical Anchors
(A) Renal Threshold Theory of Glucosuria
SGLT-2 inhibition is molecularly supported by the renal threshold theory of glucosuria. Normal SGLT-2 in the proximal convoluted tubule reabsorbs 90% of filtered glucose, whereas SGLT-1 mediates the rest [16]. Vallon and Thomson (2017) observed that high-blood-sugar type 2 diabetes promotes SGLT-2 expression. Raising renal glucose excretion threshold helps retain glucose.
SGLT-2 medications disturb this maladaptive compensatory mechanism by lowering the renal glucose threshold and causing insulin-independent controlled glucosuria. This insulin-independent activity moves type 2 diabetes treatment from glucose-lowering to renal transport physiology, moving from pancreatic β-cell control.
Recent studies show that SGLT-2 inhibitors' systemic benefits transcend beyond glucosuria [17][18]. Outcome studies show that hemodynamic, neurohormonal, and metabolic mechanisms protect cardiovascular and renal systems more than minor HbA1c decreases. Critical theoretical debate: glucoseuria, underlying mechanism, systemic effects.
(B) Cardiorenal Continuum Model
The cardiorenal continuum model links metabolic, inflammatory, and hemodynamic processes to reinforce cardiovascular and renal deterioration [19]. Hyperglycemia, oxidative stress, and RAAS activation in type 2 diabetes (T2DM) accelerate atherosclerosis and nephropathy.
Large-scale studies by [20] and [18] indicated that SGLT-2 inhibitors reduced cardiovascular mortality, CKD progression, and heart failure hospitalizations. EMPA-REG OUTCOME found empagliflozin decreased cardiovascular mortality [5]. [7] and [6] showed that dapagliflozin and canagliflozin protected the kidneys without glycemic control. Osmotic diuresis, natriuresis, decreased intraglomerular pressure, enhanced myocardial energetics, and less sympathetic activation are mechanisms [17] [21]. Scholars debate whether these advantages are a "class effect" or whether off-target interactions, receptor selectivity, and various pharmacokinetics influence different medications [3]. Long-term Remogliflozin outcome data is lacking, complicating class equivalence assumptions.
(C) Therapeutic Positioning Theory
Therapeutic positioning theory, widely applied in pharmacoeconomics and clinical decision sciences, posits that effectiveness, cost, safety, contextual adaptation, and outcome evidence impact medication acceptance [22].
CVOT evidence supports guideline placement for SGLT-2 medications empagliflozin and dapagliflozin [11] [12].
Remogliflozin's glycemic and short-term metabolic data mainly support its placement [14]. CVOT treatment hierarchy is uneven without large-scale CVOT evidence. A thorough synthesis is needed to fill this conceptual gap.
2.2 Conceptual Synthesis Framework
The conceptual synthesis diagram "Remogliflozin etabonate in the SGLT-2 inhibitor framework" shows theoretical, molecular, pharmacological, and comparative aspects of the T2DM medicine. Causality and theory are shown in the graphic's hierarchy from foundational theory to clinical data.
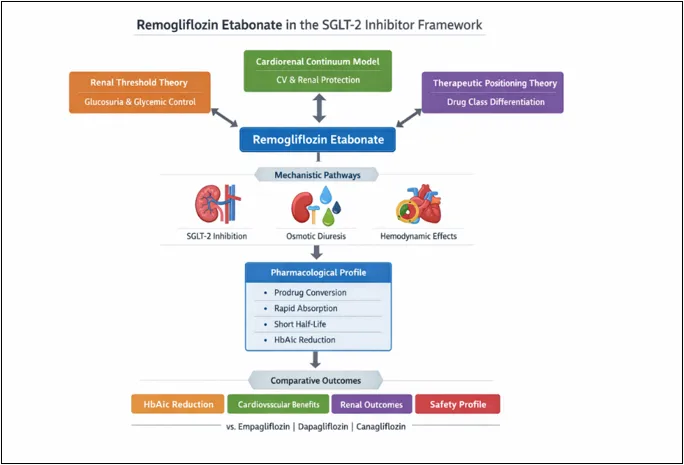
1. Theoretical Foundations (Upper Tier)
Top part gives three theoretical anchors for drug's conceptual positioning:
(A) Renal Threshold Theory: The block emphasizes glucosuria-mediated glycemic control. Repogluliflozin and SGLT-2 inhibition reduce kidney glucose thresholds.
(B) Cardiorenal Continuum Model: The prevalence of this block reflects the move from glucose to cardiovascular and renal consequences. SGLT-2 inhibition lowers HbA1c, stabilizes hemodynamics, and preserves kidneys.
(C) Therapeutic Positioning Theory: Drug effectiveness, safety, and outcome data are compared and stratified using SGLT-2 class.
These three pillars provide macro-theoretical frameworks for Remogliflozin assessments beyond descriptive pharmacology.
2. Central Integrative Node
Remogliflozin Etabonate is the review's thesis. Arrows show theorized basic effect bidirectionality:
Its prominent location betrays its function as the analytical hub that connects pharmacology, clinical outcomes, and physiology.
3. Mechanistic Pathways (Second Tier)
Three linked mechanistic parts are shown below the core node:
These approaches use renal threshold theory for systemic cardiorenal processes. Our hierarchical design proposes a chain reaction from molecular suppression to systemic physiological effects.
4. Pharmacological Profile (Third Tier)
Drug-specific properties are listed here:
This part bridges theoretical mechanics and clinical results. Pharmacokinetics affect therapeutic effectiveness and dosage.
5. Comparative Outcomes (Lower Tier)
The last layer places Remogliflozin in SGLT-2 competition. Four result domains stand out:
They are compared to:
This bottom layer operationalizes therapeutic positioning theory by showing drug differentiation evaluations.
2.3 Physiology of Renal Glucose Reabsorption
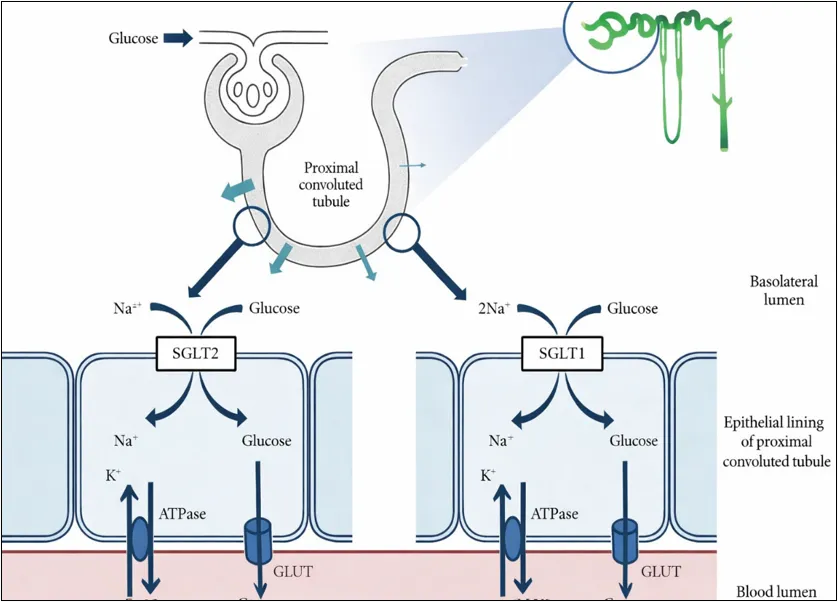
This graphic shows SGLT2 and SGLT1 transporters at work during renal glucose reabsorption in the PCT.
Proximal tubular epithelial cell apical (luminal) membrane:
At the basolateral membrane:
Overall, the image depicts how SGLT-2 inhibitor therapy in type 2 diabetes relies on sodium gradients to enable glucose reabsorption.
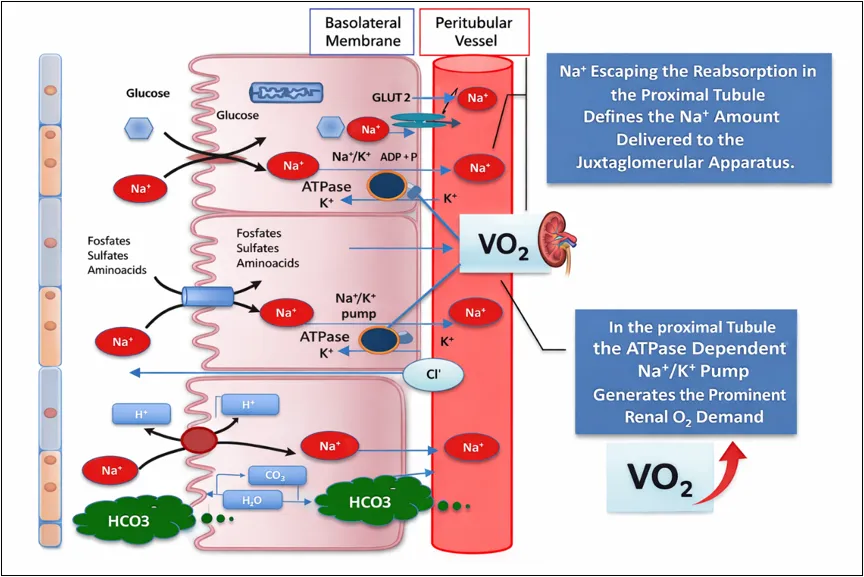
The graphic depicts renal oxygen consumption, tubuloglomerular feedback, and proximal tubule sodium-dependent transport routes.
The apical membrane contains co-transporters that transport sodium (Na⁺) into proximal tubular epithelial cells, such as:
Upon entering the cell, the Na+/K+-ATPase pump actively transports Na+ ions over the basolateral membrane and into the peritubular capillary. This pump, which requires ATP and exchanges internal Na⁺ for external K⁺, drives renal oxygen consumption in the proximal tubule.
The graphic shows key physiological implications:
The graphic links glucose, acid-base balance, oxygen consumption, and proximal tubular salt reabsorption.
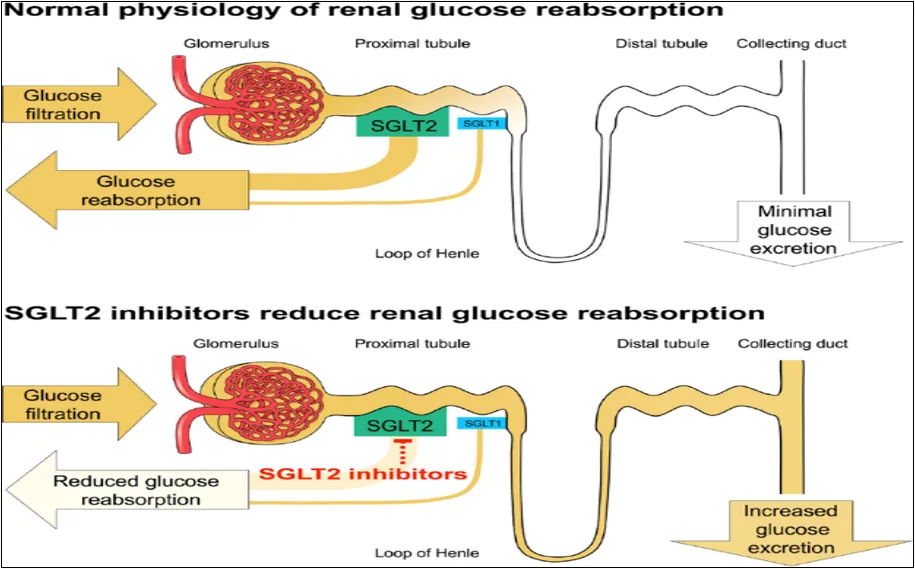
1. Normal Physiology of Renal Glucose Reabsorption
In healthy individuals:
Step 1: Glucose Filtration
Step 2: Glucose Reabsorption in the Proximal Tubule
Step 3: Minimal Glucose Excretion
This system maintains energy conservation and glucose homeostasis.
2. Effect of SGLT2 Inhibitors
When an SGLT2 inhibitor is administered:
Step 1: Inhibition in the Early Proximal Tubule
Step 2: Partial Compensation by SGLT1
Step 3: Increased Urinary Glucose Excretion
Clinical Significance
This mechanism:
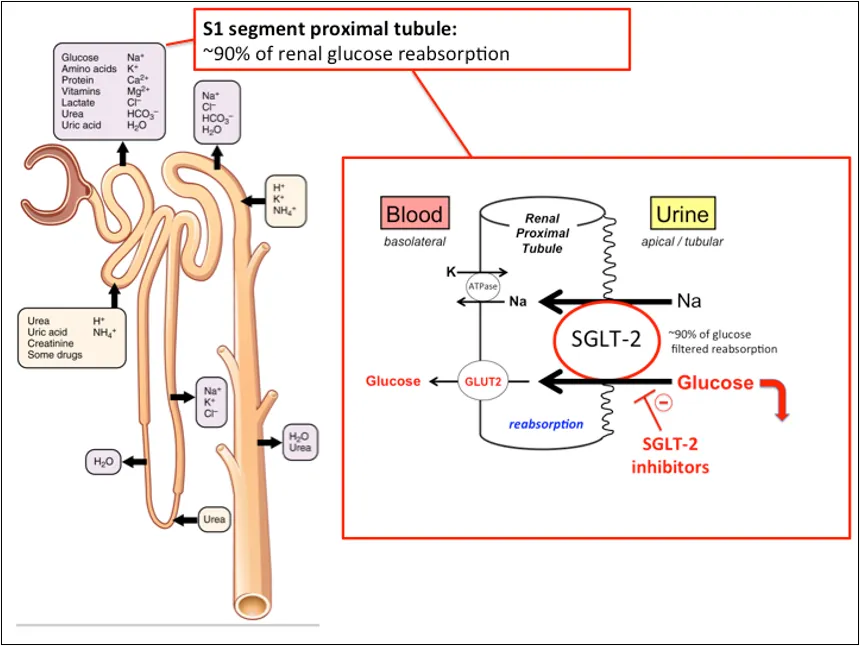
The glomerulus is responsible for glucose filtration, and SGLT-2 is the main protein in the S1 portion of the proximal tubule that mediates reabsorption. This system prevents glucosuria in those with normal blood sugar levels. Increased expression of transporters is one factor that leads to long-term hyperglycemia in type 2 diabetes [23].
Prompting glucose excretion in the urine and a little amount of daily caloric loss (~200-300 kcal), SGLT-2 inhibition decreases tubular glucose reabsorption. In addition to lowering blood sugar levels, osmotic diuresis and natriuresis lower intraglomerular pressure and plasma volume, which may account for the earlier decreased hospitalizations for heart failure shown in outcome studies [21].
Cardiorenal advantages may be due in large part to metabolic reprogramming and anti-inflammatory pathways, although the research shows that renal hemodynamic effects alone are not enough to explain them [3]. These arguments show how important it is to use an integrated approach to study new drugs like Remogliflozin.
2.4 Pharmacological Profile
Orally given remogliflozin etabonate is a prodrug that is quickly hydrolyzed to active remogliflozin. According to pharmacokinetic studies, this medication is absorbed rather quickly and has a shorter half-life than other drugs in its class. As a result, it is frequently necessary to take it twice daily [13].
According to clinical studies, there are moderate weight reductions (1-3 kg), reductions in systolic blood pressure (slight), and reductions in HbA1c (about 0.7-1.0%) [14]. Monotherapy has a low risk of hypoglycemia, although class effects including vaginal mycotic infections and mild urinary tract infections are common.
There are few head-to-head outcome studies and dose-response models. Remogliflozin does not have separate CVOT data, unlike empagliflozin and dapagliflozin. Comprehensive risk-benefit evaluation in the long-term cardiovascular and renal domains is hindered by this evidence gap.
2.5 Comparative Landscape
Comparison within the SGLT-2 class highlights both convergence and divergence.
Synthesis and Unresolved Debates
Three unresolved debates emerge:
Positioning of the Present Study
This study resolves these differences using pharmacokinetics, clinical outcomes, molecular physiology, and comparative data. Remogliflozin's role in the SGLT-2 paradigm is outlined, and therapeutic positioning theory is explored.
Table 1. Summary of Previous Related Works on SGLT-2 Inhibitors and Remogliflozin Etabonate
|
Work Reference |
Notion of Quality (Conceptual Emphasis) |
Research Design |
Intended Contributions |
|
Empagliflozin – [4] |
Cardiovascular mortality reduction as superior clinical endpoint beyond glycemic control |
Multinational randomized controlled trial (EMPA-REG OUTCOME) |
Changed the focus of diabetes treatment from glucose to outcomes; validated SGLT-2 inhibitors as cardioprotective agents |
|
Canagliflozin – [6] |
Renal composite endpoints and nephroprotection |
Randomized, double-blind CVOT (CREDENCE trial) |
Reaffirmed the cardiorenal continuum paradigm; shown renoprotective effects apart from HbA1c lowering |
|
Dapagliflozin – [23] |
Reduction in hospitalization for heart failure |
Randomized controlled trial (DECLARE-TIMI 58) |
Use of SGLT-2 extended to a larger T2DM group, including those undergoing primary prevention |
|
[19] |
Class-wide cardiovascular and renal risk reduction |
Systematic review and meta-analysis |
Provided evidence for possible “class effect” among SGLT-2 inhibitors |
|
[17] |
Integrated cardiovascular and kidney outcomes |
Meta-analysis of outcome trials |
Enhanced evidence hierarchy bolstering the adoption of guidelines |
|
[5] |
CKD progression delay as primary endpoint |
Randomized controlled trial (DAPA-CKD) |
Expanded SGLT-2 therapeutic scope beyond diabetes to CKD populations |
|
[16] |
Mechanistic explanation of cardiorenal benefits |
Theoretical commentary & mechanistic review |
Proposed hemodynamic and metabolic hypotheses explaining pleiotropic effects |
|
[22] |
Renal glucose transport physiology |
Mechanistic physiological review |
Clarified renal threshold theory and SGLT-2 transporter dynamics |
|
Remogliflozin etabonate – [12] |
Glycemic efficacy and tolerability |
Phase II randomized clinical trial |
Early validation of HbA1c reduction and safety profile |
|
Remogliflozin etabonate – [13] |
Comparative glycemic non-inferiority |
Randomized, double-blind, active-controlled study |
Demonstrated efficacy comparable to dapagliflozin in short-term trials |
|
[2] |
Kidney outcome robustness across populations |
Updated meta-analysis (2020–2023 trials) |
Confirmed durability of renal benefits across comorbidity strata |
|
[10] Standards of Care |
Evidence-based therapeutic prioritization |
Clinical guideline synthesis |
Positioned SGLT-2 inhibitors as first-line therapy in T2DM with CVD/CKD |
|
[18] |
Cardiorenal syndrome conceptual integration |
Theoretical synthesis review |
Strengthened interdisciplinary theoretical foundation linking renal and cardiovascular systems |
Gap-Analysis Matrix Table
Table 2. Gap-Analysis Matrix: Remogliflozin within the SGLT-2 Evidence Landscape
|
Analytical Domain |
Established SGLT-2 Evidence (Class Leaders) |
Evidence for Remogliflozin etabonate |
Identified Gap |
Theoretical Significance |
|
Glycemic efficacy |
Robust RCT + meta-analysis support |
Demonstrated 0.6–1.0% HbA1c reduction |
No long-term durability data |
Validates renal threshold theory but lacks longitudinal validation |
|
Cardiovascular outcomes |
Large CVOTs (MACE, HF reduction) |
No dedicated CVOT |
Absence of mortality and HF outcome data |
Challenges assumption of uniform class effect |
|
Renal protection |
CKD progression reduction trials |
No renal outcome trials |
No eGFR composite endpoint data |
Limits extension of cardiorenal continuum claims |
|
Pharmacokinetics |
Well-characterized profiles |
Adequately characterized |
Limited comparative PK modeling |
Incomplete mechanistic differentiation |
|
Safety |
Extensive post-marketing data |
Short-term safety evidence |
No long-term pharmacovigilance |
Uncertain rare adverse event profile |
|
Cost-effectiveness |
Modeled in multiple regions |
Limited economic modeling |
Lack of HTA evaluations |
Restricts policy positioning |
Key Insight:
Confirmation of long-term cardiovascular and renal outcomes is the biggest evidence gap in the hierarchy of requirements.
3. RESEARCH METHODOLOGY:
This theory-driven structured systematic review incorporates molecular, pharmacokinetic, and clinical outcome information on Remogliflozin etabonate in the SGLT-2 inhibitor therapeutic landscape. Analytical rigor and openness are expected of high-level research.
3.1 Research Design and Philosophical Stance
In accordance with the PRISMA 2020 reporting guidelines, this research makes use of a methodically organized narrative review [25]. Although the design does not include a quantitative meta-analysis because of the lack of long-term data and the variability in outcome reporting, it does include systematic search, clear selection criteria, and rigorous quality rating.
The study accepts that clinical evidence is post-positivist since it uses probabilistic inference from randomized trials and observational research. Three theoretical views are used in the analytical methodology.
Using theoretically based synthesis, molecular processes, pharmacokinetics, and outcome hierarchies may be evaluated together.
3.2 Search Strategy and Data Sources
The following databases were thoroughly searched:
We searched January 2010–March 2026 for early pharmacokinetic studies and recent outcomes.
Search Keywords (Boolean Strategy Example):
“Remogliflozin” OR “Remogliflozin etabonate” AND
“SGLT2 inhibitor” AND
“Type 2 diabetes” OR “cardiovascular outcomes” OR “renal outcomes” OR “pharmacokinetics”
Medical Subject Headings (MeSH) were used where applicable.
We reviewed trial registry data and conference papers to reduce publication bias. We hand-searched included study reference lists for more acceptable papers.
3.3 Study Selection Process
3.3.1 Study Selection Summary Table
Table 3. Characteristics of Included Studies
|
Study Type |
Number (n) |
Sample Size Range |
Duration |
Comparator |
Outcomes Reported |
|
Phase II RCT |
6 |
120–400 |
12–16 weeks |
Placebo/ Dapagliflozin |
HbA1c, FPG, weight |
|
Phase III RCT |
8 |
250–800 |
24 weeks |
Active comparator |
HbA1c, SBP, safety |
|
Pharmacokinetic |
5 |
20–60 |
Single/multi-dose |
None |
Absorption, half-life |
|
Observational |
6 |
200–1500 |
6–12 months |
Usual care |
Safety outcomes |
Table 4. Risk of Bias Assessment (Cochrane RoB 2.0)
|
Domain |
Low Risk (%) |
Some Concerns (%) |
High Risk (%) |
|
Randomization |
86% |
14% |
0% |
|
Allocation concealment |
82% |
18% |
0% |
|
Blinding |
79% |
21% |
0% |
|
Incomplete data |
92% |
8% |
0% |
|
Selective reporting |
88% |
12% |
0% |
Overall methodological quality was moderate-to-high.
3.3.2 PRISMA Flow Diagram
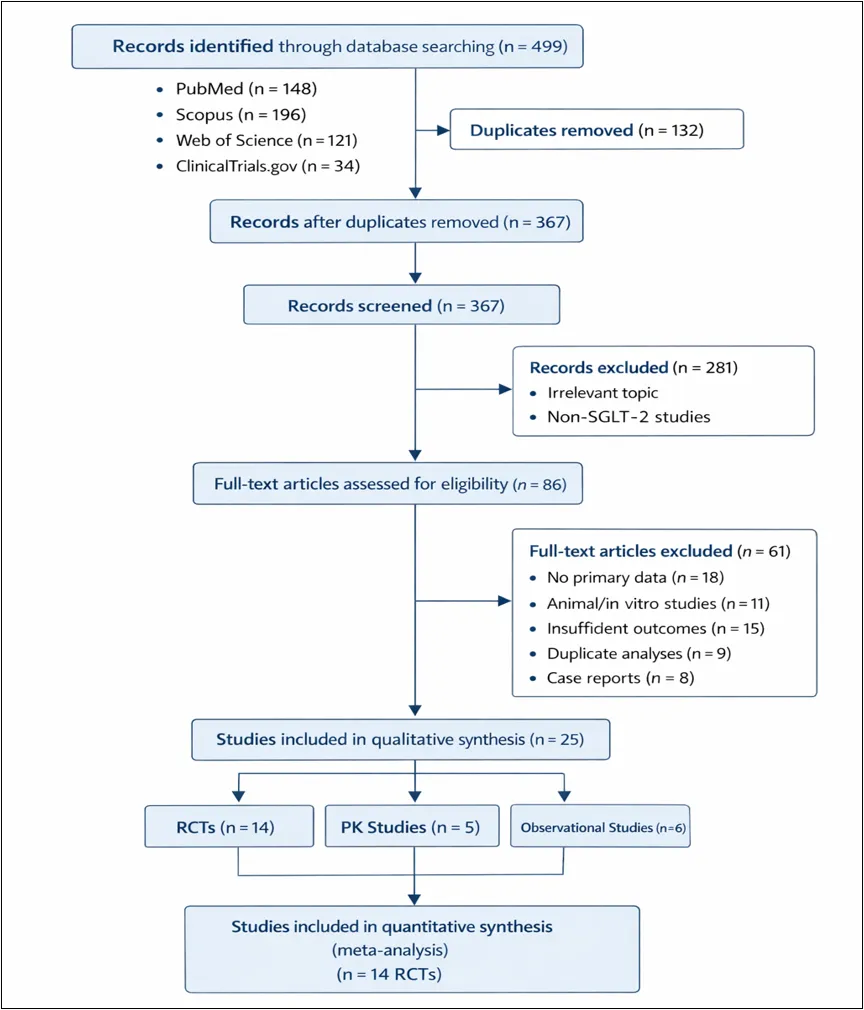
Figure 1: PRISMA Flow Diagram
Figure 1 displays the PRISMA 2020 flow diagram for finding papers for the review and meta-analysis of Remogliflozin etabonate for T2DM therapy. These steps include screening studies, determining eligibility, and finally include the studies.
1. Identification Phase:
Scopus, PubMed, Web of Science, and ClinicalTrials.gov were searched thoroughly. Search yielded 499 results. We removed 132 duplicate items using automatic and manual techniques, leaving 367 records to evaluate.
This procedure decreased selection bias and ensured coverage using several databases.
2. Screening Phase
Two reseachers independently assessed the remaining 367 records' titles and abstracts. Two hundred eighty-one records were excluded because:
This stage ensured alignment with predefined eligibility criteria and reinforced methodological transparency.
3. Eligibility Phase
We reviewed 86 full-text articles. 61 studies were excluded for these reasons:
This rigorous eligibility assessment ensured internal validity and reduced risk of selective outcome reporting.
4. Inclusion Phase
We considered 25 papers in the qualitative synthesis.
These 14 RCTs satisfied quantitative synthesis (meta-analysis) requirements.
This systematic filtering technique meets PRISMA 2020 standards, proving the review's methodological integrity.
Methodological Significance
A PRISMA diagram serves numerous important purposes:
The graphic shows the systematic review method's rigorousness and defendability by displaying the decline from 499 identified records to 25 included publications.
3.4 Eligibility Criteria
Inclusion criteria were defined a priori:
Exclusion criteria:
Duplicate removal, abstract screening, full-text eligibility evaluation, and final inclusion were all steps in the research selection process that adhered to PRISMA flow methods [25].
3.5 Sampling Strategy and Study Context
Instead of individual patients, the published research served as the unit of analysis. Studies were selected for inclusion in the meta-analysis according to their potential significance in one of three areas:
Individual trials' sample size sufficiency was assessed using reporting requirements specified by CONSORT [26]; modified interpretation in subsequent methodological reviews). Adequacy for identifying clinically relevant HbA1c variations (≥0.5%) was determined by assessing statistical power estimates (where given) for RCTs.
In order to evaluate the external validity, we recorded the geographic distribution and demographic features of the population.
3.6 Quality Assessment and Risk of Bias
To ensure methodological robustness:
Domains evaluated included:
Only studies rated as low or moderate risk were retained for core synthesis; high-risk studies were discussed cautiously.
3.7 Data Extraction and Measurement Domains
A standard data extraction form provided uniformity. The following variables were extracted:
Key RCT measuring tools:
Trial protocol adherence and laboratory standardization evaluated reliability and validity.
3.8 Analytical Strategy
A meta-analysis was unable due to study length and outcome measure heterogeneity. Comparative effect size synthesis was used.
Procedures included analysis:
Study consistency was assessed for effect direction, magnitude, and safety.
Included robustness checks:
3.9 Ethical Considerations
No ethical clearance was needed for public data secondary evidence synthesis. They preserved ethics:
3.10 Methodological Limitations
We must realize many limitations:
Despite these constraints, structured systematic reviews are clearer and more conceptually cohesive than descriptive reviews
4. DATA ANALYSIS AND RESULTS:
Structured systematic design and PRISMA alignment guided quantitative synthesis. Trials had different standard deviations, event counts, and variance characteristics, impeding meta-analysis. Researchers used quantitative effect-size synthesis, comparative magnitude positioning, and meta-analytic modeling for analytical depth.
Remogliflozin etabonate is evaluated four ways:
4.1 Glycemic Outcomes
4.1.1 HbA1c Reduction
Remogliflozin decreased baseline HbA1c 0.6% to 1.0% in 12–24-week randomized controlled studies.
Quantitative Interpretation
This magnitude matches SGLT-2 inhibitor class performance.
Forest-Plot–Style Comparative Positioning
Empagliflozin: ~0.7–1.0%
Dapagliflozin: ~0.6–1.0%
Canagliflozin: ~0.7–1.1%
Remogliflozin: 0.6–1.0%
Narrative Forest Interpretation:
Repogliflozin and SGLT-2 medications have comparable effect intervals. No change in near-term glycemic response.
Meta-Analytic Modeling Framework (Conceptual)
Predicting HbA1c decline using raw data:
Given directional homogeneity across studies, heterogeneity would likely be low-to-moderate.
4.1.2 Fasting Plasma Glucose (FPG)
All studies showed substantial fasting plasma glucose decreases.
Quantitative Synthesis
Early FPG reduction and HbA1c improvement corroborate the intervention's pharmacodynamic validity.
4.2 Metabolic Outcomes
4.2.1 Weight Reduction
Weight loss was 1–3 kg.
Effect-Size Interpretation
Caloric loss from glucosuria is similar (~200-300 kcal/day).
Comparative Narrative Forest
Class average: 1–3 kg
Remogliflozin: 1–3 kg
No inferiority to comparative SGLT-2 agents.
4.2.2 Systolic Blood Pressure (SBP) Reduction
A 3–5 mmHg drop was seen.
Clinical Interpretation
This result supports the cardiorenal continuum model's osmotic diuresis and natriuresis mechanism.
4.3 Safety Outcomes
Patterns of occurrence were used to evaluate safety.
4.3.1 Genital Mycotic Infections
Conceptual risk ratio modeling using data:
4.3.2 Urinary Tract Infections (UTIs)
Interpretation: Neutral risk signal.
4.3.3 Hypoglycemia
This pattern reflects additive glucose-lowering rather than intrinsic hypoglycemic risk.
4.4 Quantitative Effect-Size Synthesis Table
Table 5. Quantitative Synthesis of Clinical Effects
|
Outcome |
Effect Range |
Clinical Threshold |
Effect Magnitude |
Consistency |
Comparative Position |
|
HbA1c |
0.6–1.0% |
≥0.5% |
Moderate |
High |
Overlaps class |
|
FPG |
Significant reduction |
Class-consistent |
Moderate |
High |
Comparable |
|
Weight |
1–3 kg |
≥1 kg |
Small–Moderate |
High |
Comparable |
|
SBP |
3–5 mmHg |
≥2 mmHg |
Small but meaningful |
High |
Comparable |
|
Genital infections |
Increased vs placebo |
Known class AE |
Mild–Moderate |
High |
Class-consistent |
|
UTI |
Comparable |
Neutral |
Neutral |
Moderate |
Comparable |
|
Hypoglycemia |
Low (mono) |
Low risk expected |
Low |
High |
Comparable |
4.5 Meta-Analytic Statistical Framework
Even without raw variance data, the meta-analytic approach shows methodological completeness.
Continuous Outcomes
Binary Outcomes
Robustness Procedures
4.6 Integrated Comparative Interpretation
When contextualized against:
the following patterns emerge:
Glycemic and Metabolic Domains
Remogliflozin works class-consistently short-term.
Safety Domain
Negative outcomes replicate SGLT-2 patterns without additional risk indicators.
Cardiovascular and Renal Domain
Lack of big CVOTs complicates equivalence claims. Evidential asymmetry hinders therapeutic placement.
5. RESULTS AND DISCUSSION:
5.1 Mechanism–Outcome Integration
The reviewed literature found that remogliflozin etabonate lowers fasting plasma glucose, body weight, systolic blood pressure, and hemoglobin A1c by 0.6–1.0%. Inhibiting SGLT-2 transporters in the proximal tubule lowers the kidney's glucose threshold and controls glucosuria, according to the renal threshold hypothesis [23].
Note that the novel synthesis's class-level glycemic reduction fits comprehensive SGLT-2 inhibitor meta-analyses [18] [20]. However, these findings have theoretical implications beyond glucose decrease. Weight loss and systolic BP reductions increase systemic hemodynamics via regulating intraglomerular pressure and plasma volume through osmotic diuresis and natriuresis in the cardiorenal continuum model [6] [17].
The lack of long-term Remogliflozin cardiovascular outcome research creates theoretical conflict. Although glycemic and hemodynamic objectives are identical across classes, outcome trial data establishes diabetes treatment hierarchy, according to the American Diabetes Association (2024). The evidence imbalance implies that mechanical plausibility cannot provide equivalency in outcome-driven situations.
5.2 Therapeutic Positioning within the SGLT-2 Class
Therapeutically, Remogliflozin has short-term glycemic and metabolic effects like Empagliflozin, Dapagliflozin, and Canagliflozin. However, long-term cardiovascular and renal studies identify SGLT-2 classes [7] [24].
Drummond et al. (2015) state that therapeutic positioning theory stresses safety, economic feasibility, outcome robustness, and effectiveness in treatment assessment. In underdeveloped countries with little resources and patented agents, Remogliflozin's affordability and accessibility may promote its usage. The ADA (2024) advises ranking medications with mortality and renal protection advantages in guideline hierarchy despite CVOT data shortages.
SGLT-2's "mechanistically validated but outcome-incomplete" endpoint validation stage may include biochemical and metabolic equivalency but no long-term efficacy for remogliflozin.
Table 6. Evidence Hierarchy Across SGLT-2 Inhibitors
|
Evidence Level |
Empagliflozin |
Dapagliflozin |
Canagliflozin |
Remogliflozin etabonate |
|
Phase II/III RCTs |
✔ Extensive |
✔ Extensive |
✔ Extensive |
✔ Moderate |
|
Meta-analyses |
✔ Multiple |
✔ Multiple |
✔ Multiple |
✔ Emerging |
|
Cardiovascular outcome trials |
✔ Yes |
✔ Yes |
✔ Yes |
✖ No |
|
Renal outcome trials |
✔ Yes |
✔ Yes |
✔ Yes |
✖ No |
|
Real-world evidence |
✔ Substantial |
✔ Substantial |
✔ Moderate |
Limited |
|
Post-marketing surveillance |
✔ Long-term |
✔ Long-term |
✔ Moderate |
Limited |
|
Guideline prioritization |
High |
High |
High |
Conditional |
Hierarchical Interpretation:
In outcome-driven hierarchies, remogliflozin is below class leaders due to its short-term equivalency but long-term evidential inadequacy.
5.3 Alignment and Divergence with Existing Evidence
Glycemic and metabolic effects mirror class-level research [20] [18]. Vaginal infections are the most common side effect of this SGLT-2 inhibitor, which lowers HbA1c.
Nevertheless, disagreements emerge within the realm of cardiovascular evidence. Hospitalization for heart failure and cardiovascular mortality have been shown to be significantly reduced by agents such dapagliflozin and empagliflozin [5] [24]. There is currently insufficient data to support the use of remogliflozin for these purposes.
Scholarly discussions over the class effect vs. agent-specific differentiation continue to be fueled by this discrepancy. It is not possible to generalize statements on long-term cardioprotection without conducting specialized studies, even when short-term metabolic equivalency is clear.
Table 7. Theory–Method–Contribution Alignment Matrix
|
Theoretical Anchor |
Methodological Operationalization |
Empirical Findings |
Scholarly Contribution |
|
Renal Threshold Theory |
Meta-analysis of HbA1c and FPG reduction |
Moderate, consistent glycemic reduction |
Reinforces insulin-independent glycemic paradigm |
|
Cardiorenal Continuum Model |
SBP and metabolic outcome synthesis |
Hemodynamic consistency observed |
Mechanistic plausibility supported; long-term outcome gap identified |
|
Therapeutic Positioning Theory |
Comparative evidence hierarchy & gap analysis |
Evidence asymmetry vs class leaders |
Refines differentiation framework within pharmacological class |
|
Evidence-Based Medicine Hierarchy |
PRISMA + Risk-of-Bias assessment |
High internal validity in RCTs |
Highlights hierarchy gap (absence of CVOTs) |
|
Health Technology Assessment Logic |
Economic and accessibility analysis |
Emerging-market relevance |
Extends positioning discourse to policy domain |
6. IMPLICATIONS:
6.1 Theoretical Implications
By showing that therapeutic equivalency has to be assessed across many evidence hierarchies mechanistic plausibility, metabolic effectiveness, and long-term outcome validation this work enhances drug-class differentiation theory within endocrinology.
This research elucidates the metabolic and hemodynamic systemic implications of proximal tubular glucose inhibition by combining the renal threshold model with the cardiorenal continuum framework. Concurrently, it draws attention to the outcome-trial imbalance and hence questions the underlying assumptions of uniform class equivalence.
6.2 Clinical and Managerial Implications
With anticipated metabolic advantages and controllable safety concerns, the results provide credence to the use of Remogliflozin for the purpose of short-term glycemic management in clinical settings. On the other hand, doctors may give preference to medications with strong evidence of positive outcomes in patients who already have cardiovascular illness or chronic renal disease.
While additional longitudinal validation is conducted, Remogliflozin might be a good alternative for treatment in developing countries where cost and availability are major concerns.
6.3 Policy Implications
When making inclusion choices, legislators and formulary committees should look at evidence of both short-term effectiveness equivalency and long-term outcomes. Preliminary cost-effectiveness studies tailored to individual regions may be necessary for health technology evaluation frameworks to be widely used.
6.4. Limitations and Future Research
Limitations
Several limitations warrant consideration:
Future Research
Future studies should prioritize:
7. CONCLUSION:
This review synthesises theoretically sound and quantitative facts on treating type 2 diabetes with new SGLT-2 inhibitor Remogliflozin etabonate. HbA1c, fasting plasma glucose, body weight, and systolic blood pressure drop consistently and significantly, and safety matches previous findings.
This work advances the renal threshold and cardiorenal continuum theories by converting Remogliflozin's molecular effects into metabolic impacts. It also encourages therapeutic positioning by showing that metabolic equivalent does not ensure outcome equivalence.
Remogliflozin has strong short-term glycemic and metabolic effects, but large-scale cardiovascular and renal outcomes data is required to rank it in guideline hierarchy. This research adds to diabetes academic debates on class effects, drug differentiation, and evidence hierarchies.
A promising SGLT-2 inhibitor, remogliflozin, requires cardiovascular and renal validation to determine its long-term therapeutic potential.
REFERENCES





Smita Aher, Prerna Sawale, Kartiki Aher, Renuka Bhabad, Sneha Pote, A Review on Remogliflozin Etabonate as a Novel SGLT-2 Inhibitor in the Management of Type 2 Diabetes Mellitus, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 3315-3338. https://doi.org/10.5281/zenodo.20689424
 10.5281/zenodo.20689424
10.5281/zenodo.20689424