
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Genesis institute of pharmacy, Radhanagari.
Metoprolol serves as a commonly used medication which functions as a cardioselective ??-adrenergic receptor blocker to treat hypertension and ischemic heart disease and arrhythmias and chronic heart failure. The medication metoprolol shows a safe profile for use; however, increasing evidence from adverse drug reaction (ADR) studies and case reports and post-marketing pharmacovigilance surveillance shows that metoprolol can cause rare but serious immune-related and skin and nerve and heart problems.Objective:The review investigates metoprolol adverse drug reactions through pharmacovigilance methods which assess immune-mediated skin toxicity and cardiovascular failure and central nervous system symptoms and overdose effects and all significant drug interactions.Methods:The research team conducted a narrative pharmacovigilance review which used published case reports and observational studies and overdose case series and spontaneous ADR reporting data as research sources. The analysis of reported adverse reactions used a standardized safety framework which included principles for causality assessment and classification according to the Medical Dictionary for Regulatory Activities (MedDRA) system organ classes and preferred terms when applicable.Results:The research shows that metoprolol causes delayed immunological skin reactions which include lichenoid drug eruption and pemphigus foliaceus together with acute heart failure deterioration and myocarditis and central nervous system disturbances and immediate hypersensitivity reactions and life-threatening overdose toxicity which happens mostly with extended-release formulations and calcium channel blocker co-ingestion. The research shows that many reactions show delayed onset which makes them difficult to recognize and leads to their misidentification. The primary factors which lead to positive results in treatment involve early drug discontinuation and supportive care.Conclusion:Metoprolol serves as a vital treatment for cardiovascular conditions. The medication can cause uncommon yet life-threatening negative effects. The detection and prevention of metoprolol-related adversed drug reactions in present-day medical settings requires improved clinician knowledge and personalized patient evaluation and standardized MedDRA reporting procedures which enable effective monitoring of ADRs.
The second-generation β-adrenergic receptor blocker metoprolol was developed to improve β₁-receptor selectivity which protects patients from the bronchospastic and metabolic side effects that result from non-selective β-blocker use. The pharmacological characteristics of metoprolol together with its safety profile make it the most frequently prescribed cardiovascular medication throughout the world[1].
Metoprolol serves as a medical treatment for patients with hypertension, angina pectoris, acute myocardial infarction, chronic heart failure with reduced ejection fraction (HFrEF), and various supraventricular and ventricular arrhythmias[2]. The medical field uses both immediate-release (tartrate) and extended-release (succinate) forms of the medication to provide doctors with flexible dosing options for patients who experience acute and chronic cardiovascular conditions[3].
The selective β-blockers of metoprolol demonstrate β₁-adrenergic receptor inhibition which decreases at higher doses[4]. The drug does not possess any active sympathomimetic effects together with α-adrenergic blocking abilities which exist in modern vasodilating β-blockers, thus these attributes determine both its medical effectiveness and its side effect profile[5].
The safety profile of metoprolol shows high reliability after its long-term use yet research data from ADR investigations and post-marketing monitoring and pharmacovigilance records show the drug can cause uncommon delayed allergic reactions together with severe heart problems that occur during high-risk medical situations. Many of these events are underreported or misattributed, particularly when they occur weeks after the initial incident.
This review serves as an ADR-centric pharmacovigilance study, integrating evidence from reports of cases, data collected through observation, and impulsive reporting systems. Reported adverse reactions are analyzed using an established pharmacovigilance framework, which includes classification based on the Medical Dictionary for Therapeutic Actions (MedDRA) system of organ classes and chose terms, when relevant. This review seeks to enhance the detection, reporting, and risk evaluation of metoprolol-related adverse drug reactions (ADRs) in modern clinical practice by synthesizing existing clinical evidence.
Table 1: Classification of Metoprolol-Associated ADRs (MedDRA-Based)
|
System Organ Class (SOC) |
Preferred Term (PT) |
Onset |
Severity |
|
Skin & SC Tissue |
Lichenoid dermatitis |
Delayed |
Moderate |
|
Immune System |
Pemphigus foliaceus |
Delayed |
Severe |
|
Cardiac Disorders |
Bradycardia |
Early |
Moderate |
|
Nervous System |
Fatigue, depression |
Variable |
Mild |
|
Immune System |
Anaphylaxis |
Immediate |
Severe |
PHARMACOLOGICAL BASIS FOR ADVERSE REACTIONS
Metoprolol's main pharmacological effect is to block β₁-adrenergic receptors, which lowers the heart rate, contractility of the myocardium, and cardiac output[6]. These effects are responsible for its therapeutic efficacy in heart disease; however, they also constitute the mechanistic foundation for various heart adverse drug reactions (ADRs), especially cardiac arrest, low blood pressure, and acute cardiac decompensation. in susceptible or unstable patients.
Metoprolol undergoes significant first-pass hepatic metabolism, primarily through the cytochrome P450 enzyme called CYP2D6[7]. Genetic variations in CYP2D6 genes lead to considerable variation between individuals in drug exposure, where poor metabolizers demonstrate elevated levels in the blood and an augmented risk of dose-related adverse drug reactions (ADRs)[8]. Utilizing CYP2D6 inhibitors at the same time makes this risk even higher, which shows how important it is to give each person their own dose and keep an eye on them[9].
In addition to its heart effects, the drug metoprolol along with other β-blockers may affect immune function[10]. Suggested immunopathological mechanisms encompass modified cytokine signaling, the induction of toxic CD8⁺ T cell lymphocytes, and drug-induced immune activation[11]. These immunomodulatory effects offer a credible mechanistic rationale for infrequent immune-mediated adverse drug reactions, including lichenoid drug explosions and autoimmune severe disorders documented in pharmacovigilance studies.
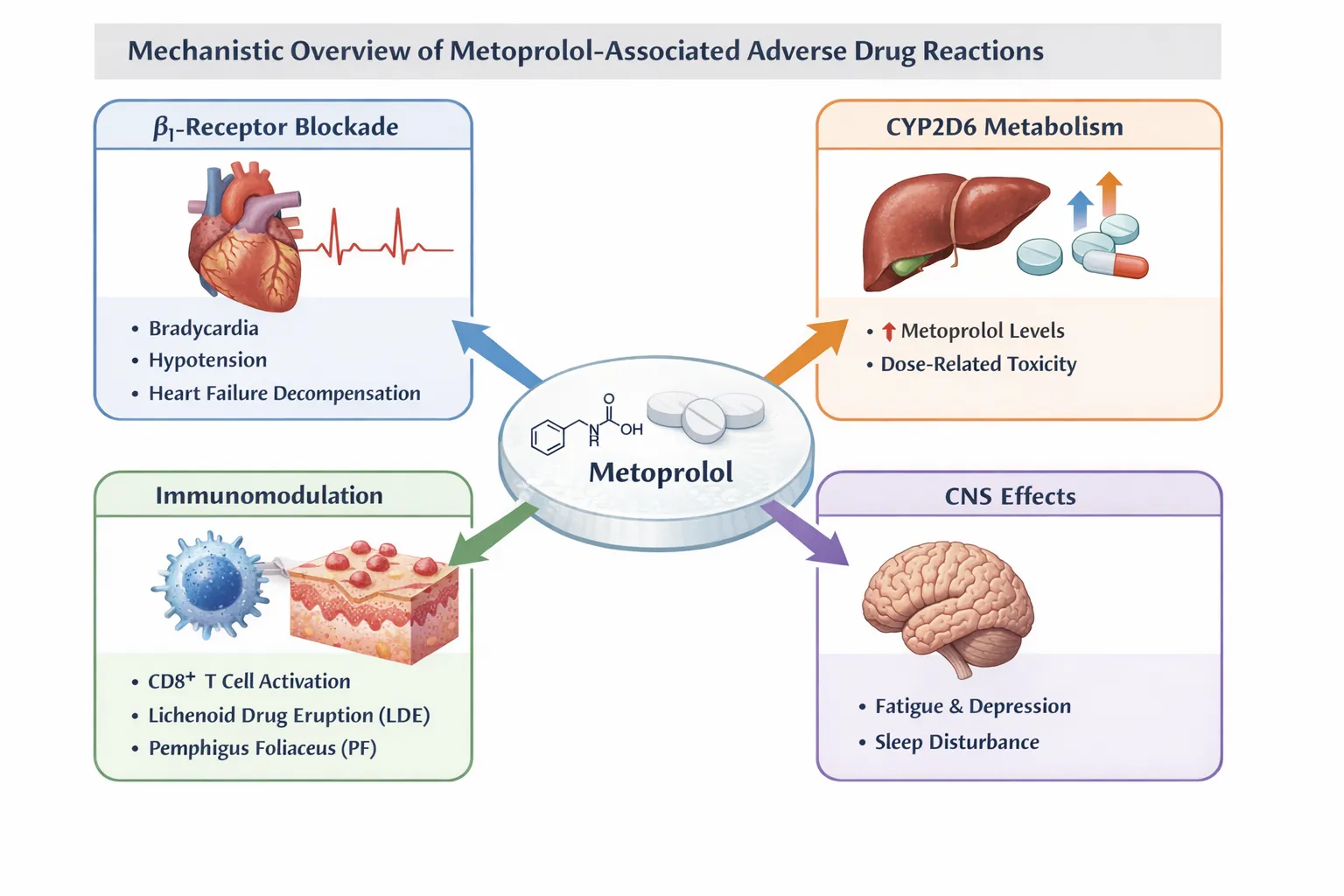
Figure 1: Mechanistic Overview of Metoprolol-Associated ADRs
DERMATOLOGICAL ADVERSE DRUG REACTIONS
Lichenoid Drug Eruption (LDE)
Metoprolol-related allergic drug manifestation is an infrequent yet acknowledged immune-mediated cutaneous unwanted drug reaction, progressively documented via reports of cases and post-marketing surveillance data. The reaction usually happens a few weeks to a few months after therapy starts, which is in line with a delayed-type sensitivity mechanism. Clinically, patients exhibit intensely pruritic, violet-colored to pigmented lichenoid pustules and plaques, predominantly affecting the sides as well as trunk, with mucosal involvement typically absent. Histopathological examination is essential for diagnosis and typically demonstrates a classic skin interface dermatitis, marked by normal keratinocyte destruction, an extensive band-like lymphocyte infiltrate at the epidermal junction, and an abundance of eosinophils, indicating a drug-induced etiology instead of idiopathic lichen planus. In an ADR study, the timing of metoprolol exposure, the resolution after stopping the drug, and the positive dechallenge are all important factors for figuring out if the drug caused the problem. These factors are usually considered "probable" by standard pharmacovigilance algorithms. Symptoms generally ameliorate following the cessation of metoprolol, in topical corticosteroids employed for symptomatic relief. In pharmacovigilance databases, such reactions are frequently encoded with MedDRA preferred terms pertaining to lichenoid dermatitis, highlighting the necessity of precise reporting to enhance signal detection for infrequent β-blocker–associated cutaneous adverse drug reactions [13].
Pemphigus Foliaceus (PF)
In rare cases, metoprolol has been linked to drug-induced pemphigus foliaceus, a serious autoimmune blistering disorder that is one of the most serious skin reactions to β-blocker therapy[14]. Pemphigus foliaceus is marked by superficial, delicate blisters that readily rupture, resulting in extensive erosions and crusted wounds, primarily impacting the top of the head, face, and body, while preserving mucous membranes[15]. Drug-induced autoantibody production against desmoglein-1, a crucial adhesion molecule in the basal epidermis, is the underlying pathophysiology that leads to keratinocyte cohesion loss. Metoprolol-induced pemphigus foliaceus may have a more severe and protracted clinical history than lichenoid drug eruptions, and it frequently does not go away with stopping the medication alone. To establish disease management, systemic immunosuppressive therapy—which includes corticosteroids and steroid-sparing agents—is often necessary. From a pharmacovigilance perspective, identifying metoprolol as a possible trigger is essential since early detection and timely discontinuation of the offending medication may lessen the severity of the illness and improve results. In order to identify uncommon but significant autoimmune dermatological reactions linked to frequently prescribed cardiovascular drugs, these instances emphasize the significance of diligent ADR reporting, MedDRA-based categorization, and ongoing post-marketing surveillance.
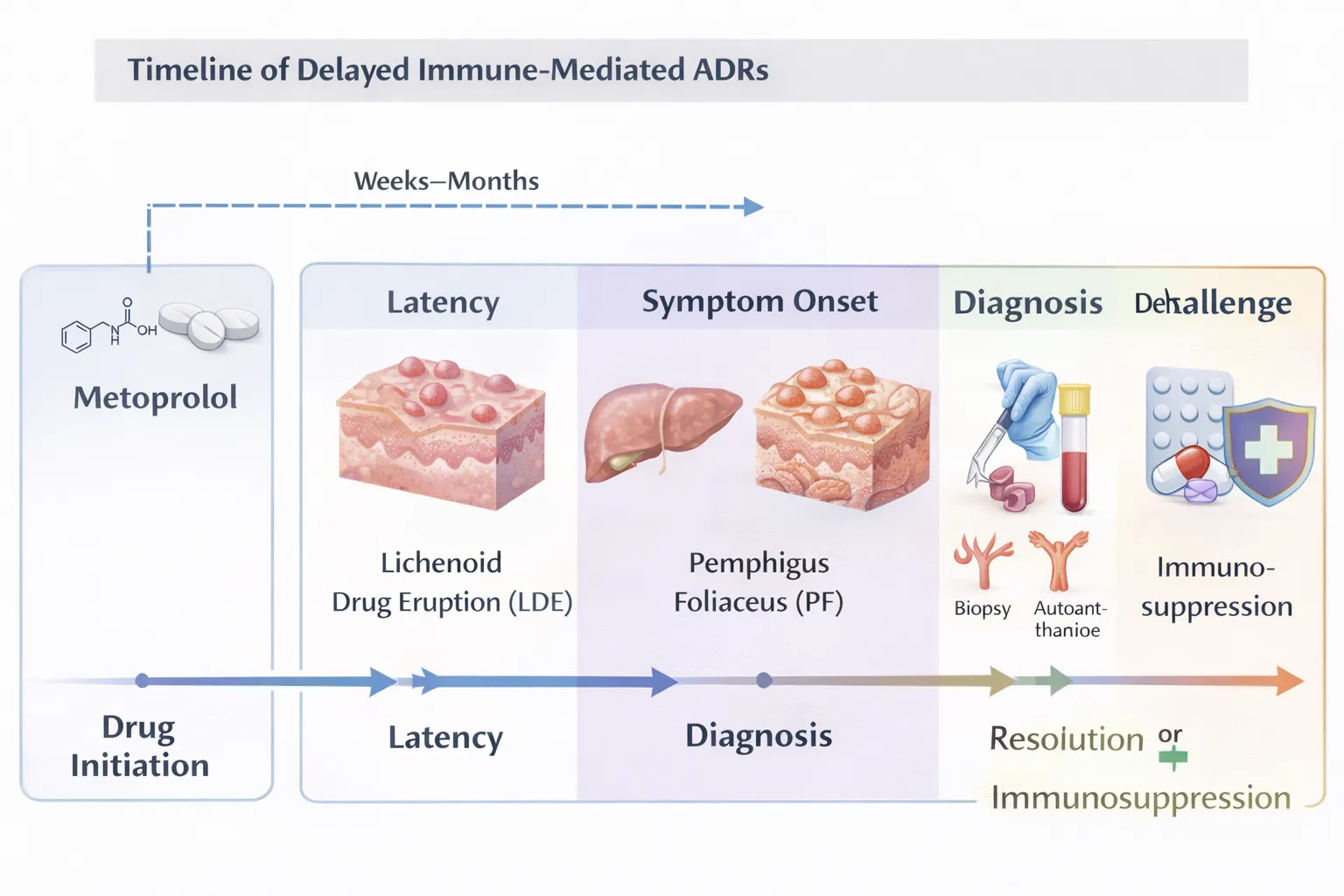
Figure 2: Timeline of Delayed Immune-Mediated ADRs
CARDIOVASCULAR TOXICITY AND HEMODYNAMIC COMPLICATIONS
Acute Decompensated Heart Failure
Metoprolol is a key treatment for long-lasting, stable heart failure with decreased ejection fraction (HFrEF), but starting or continuing it during acutely decompensated heart failure episodes carries a known risk of severe adverse pharmacological responses related to the cardiovascular system. Metoprolol lowers heart rate and myocardial contractility by β₂-adrenergic inhibition, which may seriously compromise cardiac output in patients with hemodynamic instability. These pharmacodynamic characteristics can hasten the development of overt cardiogenic shock, worsen hypotension, and cause further hemodynamic degradation in the context of volume overload, low blood pressure, or cardiogenic shock. From the standpoint of pharmacovigilance, these occurrences are frequently underreported since they might be ascribed to the advancement of the illness rather than drug-related etiology. However, metoprolol's contribution to these acute cardiovascular adverse medication reactions is well supported by temporal correlation, dose beginning or escalation, and clinical improvement after drug discontinuation [16].
Metoprolol in COVID-19–Associated Myocarditis
The possible risks of early β-blocker use in individuals suffering from acute viral myocarditis have been brought to light by emerging data from case-specific pharmacovigilance studies during the COVID-19 pandemic. Following early metoprolol commencement, a documented instance of COVID-19-associated myocarditis with significant biventricular dysfunction of the s showed clinical progression, as evidenced by increasing hypertension and low-output heart function. In this case, the decrease in cardiac output in an underlying inflamed and defective myocardium was probably exacerbated by β₂-receptor blockage, which led to hemodynamic instability. This instance highlights the significance of distinguishing between acute inflammatory myocardial damage and stable heart failure, even though β-blockers are helpful in chronic cardiomyopathy.From the perspective of an ADR research, these examples highlight the possibility that metoprolol-associated cardiovascular toxicity is situational rather than dose-dependent and highlight the necessity of using careful clinical judgment. According to pharmacovigilance data, β-blockers should not be started until hemodynamic recovery is attained and should be avoided during the acute, unstable phase of myocarditis or shock [17].
Severe Metoprolol Toxicity and Refractory Shock Following Overdose
Metoprolol is usually tolerated well at therapeutic levels, but a large overdose, especially with extended-release formulations, can cause severe and potentially fatal cardiovascular damage [18]. Refractory low blood pressure, cardiovascular shock, and multi-organ failure have been reported in pharmacovigilance reports of purposeful overdose, particularly when metoprolol is taken with calcium channel blockers like amlodipine [19]. A 15-year-old girl who showed up around 14 hours after purposefully consuming a significant amount of extended-release metoprolol with amlodipine was one particularly illuminating case. The patient experienced chronic hypotension that did not improve with high-dose catecholamines such as dopamine, norepinephrine, and dobutamine, even after early gastric lavage. Notably, transthoracic echocardiogram showed maintained left ventricular systolic function and early electrocardiography indicated normal sinus rhythm, underscoring a crucial pharmacovigilance insight: serious β-blocker toxicity can happen despite apparently normal cardiac imaging findings.
The combined toxicology mechanisms involved significant β₁-receptor blockade resulting in diminished contraction of the myocardium, peripheral vasodilation with compromised vascular tone, and suppression of calcium-mediated myocardial excitation due to simultaneous blocked calcium channels toxicity. This combination caused shock that wouldn't go away with regular drugs. Management necessitated a vigorous multimodal intervention, encompassing continuous a calcium gluconate infusion, increasing vascular support, and ultimately venous oxygenated extracorporeal (VA-ECMO) in conjunction with prone ventilation. Extracorporeal life support acted as an interface to recovery by keeping the body's blood flow and oxygen levels stable while giving the body time to break down and get rid of drugs. From a pharmacovigilance and adverse drug reaction study standpoint, this case highlights the enduring toxicity risk linked to extended-release metoprolol, the inadequacies of early diagnostic markers in ruling out severe poisoning, and the essential function of prompt escalated situations to ventilatory support in refractory shock. It also emphasizes the necessity for increased monitoring of β-blocker overdose among young people and individuals with preexisting psychiatric comorbidities, underscoring the imperative for preventive measures and focused risk evaluation[20].
Table 2: Summary of Key Published ADR Case Reports
|
ADR Type |
Patient Profile |
Dose/Formulation |
Outcome |
|
LDE |
Adult |
IR |
Resolved after withdrawal |
|
PF |
Elderly |
Chronic |
Required immunosuppression |
|
Myocarditis |
COVID-19 |
Early use |
Hemodynamic worsening |
|
Overdose |
Adolescent |
ER + CCB |
VA-ECMO required |
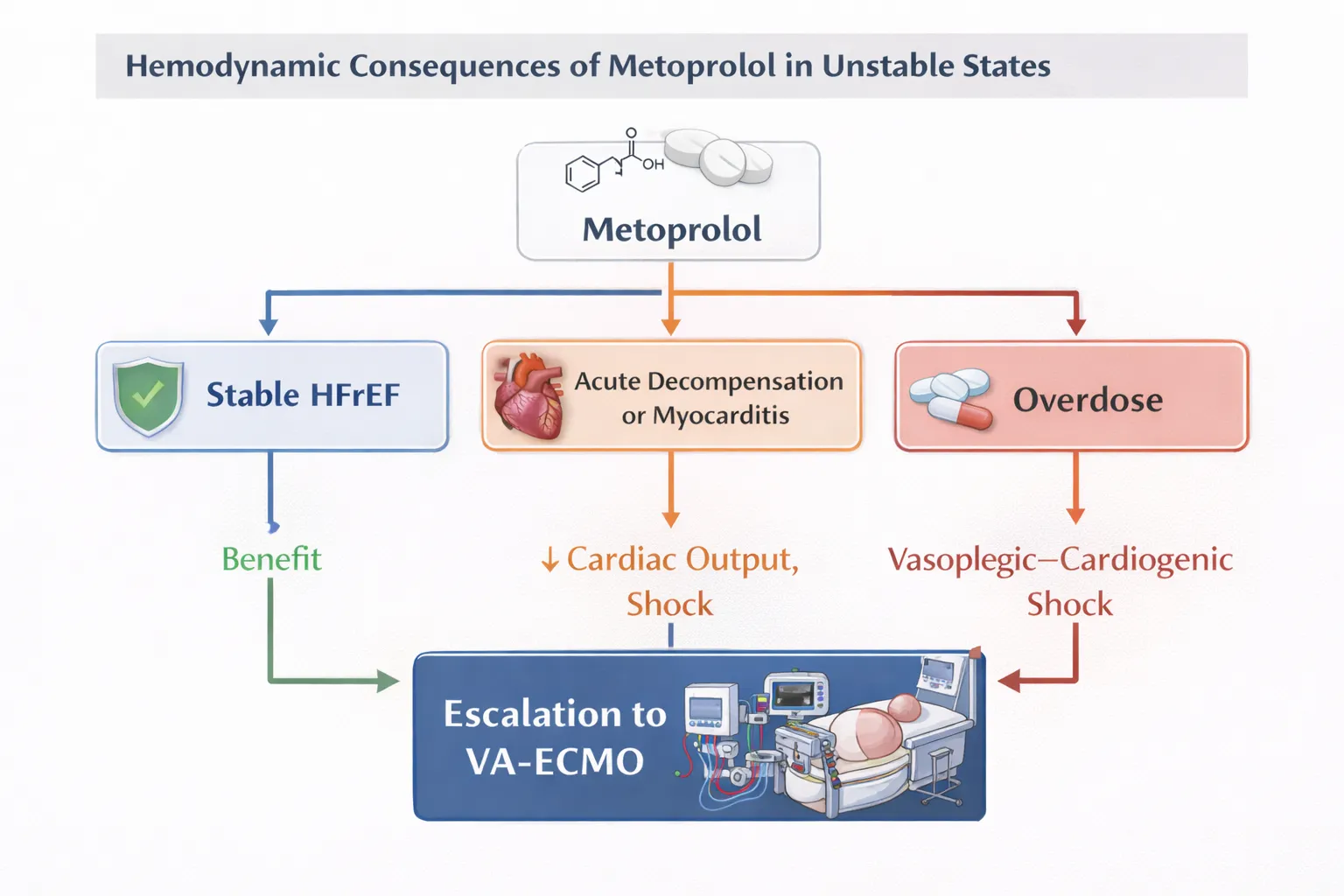
Figure 3: Hemodynamic Consequences of Metoprolol in Unstable States
IMMUNOLOGICAL AND AUTOIMMUNE COMPLICATIONS
Metoprolol has been linked to various immune-related side effects that, while infrequent, are of clinical importance and frequently overlooked[21]. Pharmacovigilance information and case-based adverse drug reaction (ADR) reports suggest that metoprolol may induce drug-related autoantibody generation and delayed hypersensitivity responses, indicating an immune controlled mechanism instead of direct dose-dependent toxicity[22]. Proposed mechanisms encompass modifications of immune tolerance, heightened stimulation of lymphocytes that are cytotoxic, and drug-hapten-mediated immune responses, potentially resulting in autoimmune dermatological conditions such as lichenoid drug explosions and pemphigus foliaceus[23]. These reactions frequently manifest with delayed onset, emerging weeks to months post-initiation, thereby complicating the assessment of causality and contributing to underreporting in spontaneous reporting systems.
Cross-reactivity among -blockers in immune-related reactions seems to be erratic and does not consistently align with β₁ specificity or lipophilicity. Reports of recurrence after switching to different β-blockers show how important it is to be careful when giving affected patients another chance. From a pharmacovigilance point of view, believed immune-mediated ADRs should lead to the permanent stopping of metoprolol and a careful look at the situation before switching to a different class of drugs. To enhance the identification of signals and risk assessment for these rare but serious side effects, it is important to keep accurate records and reports using standard MedDRA language.
IMMEDIATE HYPERSENSITIVITY REACTIONS
Immediate hypersensitivity responses to metoprolol are uncommon but may be life-threatening, serving as a significant safety indicator in post-marketing pharmacovigilance monitoring. Reported reactions encompass urticaria, angioedema, bronchospasm, and, in severe instances, an allergic reaction occurring shortly after drug exposure. These occurrences indicate either IgE-mediated or non-IgE-mediated mast cell stimulation and may transpire in patients with no previous record of drug allergies[24]. Because these reactions happen quickly, they are easier to spot. However, when more than one medication is given at the same time, it may still be missed that metoprolol is to blame.
Management of immediate hypersensitivity reactions necessitates the swift cessation of metoprolol and the initiation of conventional emergency medical protocols, including breathing support, antihistamines, corticosteroids, and intramuscular epinephrine if indicated. Avoid giving metoprolol again at all costs, and think about other non-β-blocker treatments. From the point of view of an ADR study, it is very important to report these reactions in a systematic way using the correct MedDRA preferred terms. This is necessary to get an accurate estimate of how often they happen, find out what makes patients more likely to have them, and help doctors make decisions about the safety of β-blockers.
NEUROLOGICAL AND CENTRAL NERVOUS SYSTEM EFFECTS
Metoprolol has been linked to a variety of cerebral and central nervous system (CNS) adverse drug reactions that are predominantly mild to moderate in severity yet serious in nature, especially in elderly individuals and those with pre-existing neuropsychiatric disorders[25]. Commonly documented central nervous system adverse drug reactions in pharmacovigilance databases encompass fatigue, depressive symptoms, sleep disturbances, vivid dreams, and diminished concentration. Extrapyramidal symptoms and delirium have been infrequently reported, particularly at elevated doses or among susceptible populations. Metoprolol's moderate lipophilicity allows it to cross the blood-brain barrier more easily than hydrophilic β-blockers, which means it has more exposure in the CNS. These effects are usually reversible when the dose is lowered or the drug is stopped. From an ADR reporting standpoint, CNS reactions could be underreported owing to their nonspecific characteristics and common misattribution to age-related changes, comorbid conditions, or psychological stress, highlighting the necessity of systematic evaluation and MedDRA-driven coding in pharmacovigilance research.
DRUG–DRUG INTERACTIONS
Pharmacokinetic Interactions
Metoprolol has clinically significant drug-drug interactions because it is broken down by the liver using the CYP2D6 enzyme. Taking CYP2D6 inhibitors at the same time as metoprolol can greatly raise the levels of metoprolol in the blood, which can lead to bradycardia, hypotension, and CNS toxicity. Pharmacodynamic interactions are frequent, especially with calcium channel blockers, leading to cumulative negative chronotropic and inotropic effects that can cause severe bradyarrhythmias or heart block. Taking other antihypertensive drugs at the same time increases the possibility of symptomatic hypotension even more, especially when starting or increasing the dose. These interactions are a common cause of avoidable ADRs found in pharmacovigilance studies.
Clinical Risk Mitigation
To lower metoprolol-associated ADRs and interaction-driven toxicity, it is important to have strategies for minimizing risk. Safe prescribing means slowly increasing the dose, keeping a close eye on heart rate and blood pressure, and not using drug combinations that are known to be dangerous. Taking into account pharmacogenomic variability, especially CYP2D6 poor metabolizing status, may help tailor therapy to each patient and avoid adverse drug reactions. From a pharmacovigilance perspective, the proactive detection of interaction-related adverse drug reactions (ADRs) and the standardized reporting utilizing MedDRA terminology are essential for enhancing drug safety monitoring and guiding evidence-based prescribing practices.
Table 3: Drug–Drug Interactions and Clinical Consequences
|
Interacting Drug |
Mechanism |
Clinical Risk |
|
CYP2D6 inhibitors |
↑ Metoprolol levels |
Bradycardia |
|
Calcium channel blockers |
Additive negative inotropy |
Shock |
|
Other antihypertensives |
Synergistic BP reduction |
Hypotension |
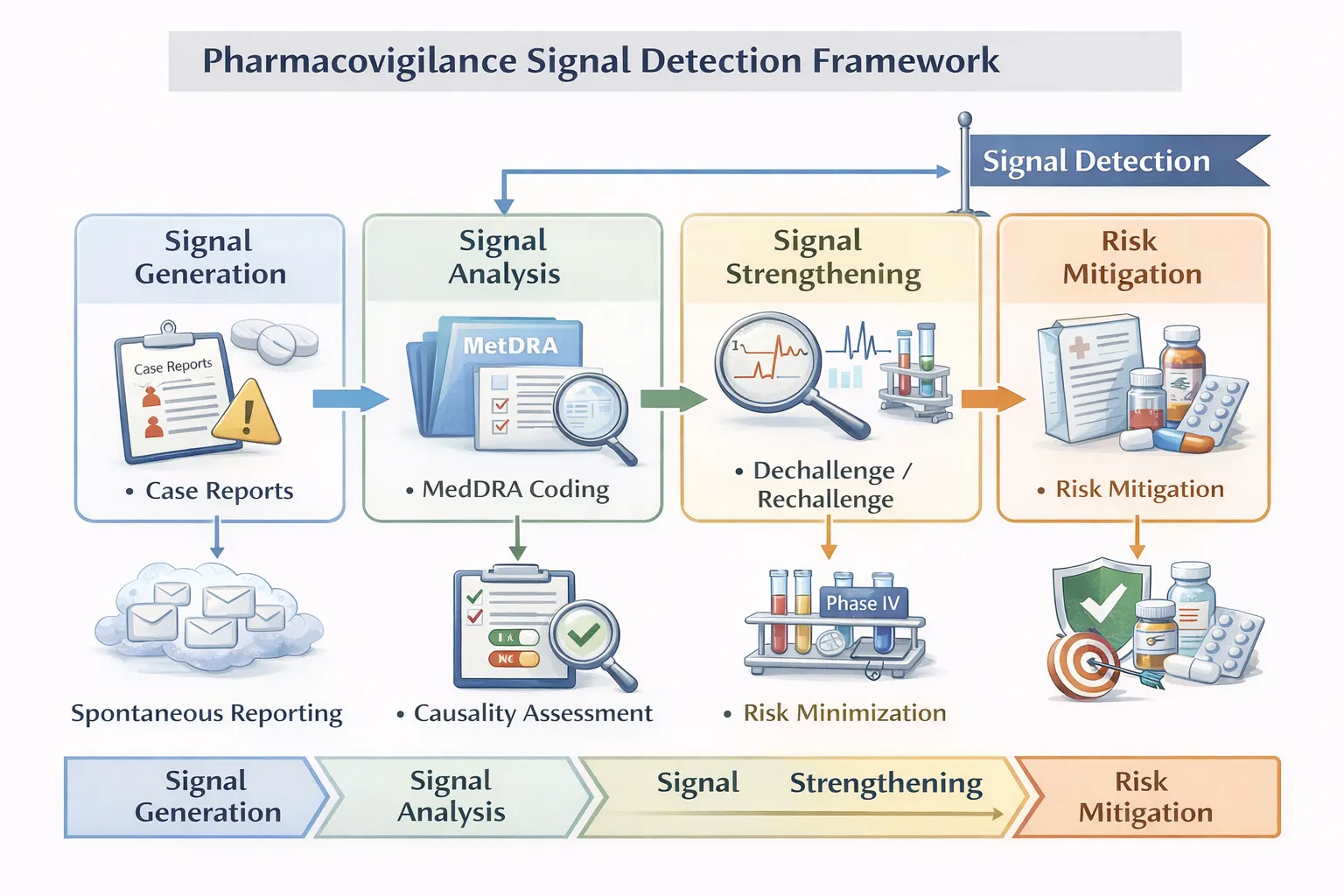
Figure 4 : Pharmacovigilance Signal Detection Framework
DISCUSSION
This review has demonstrated that so called long established drugs such as metoprolol will continue to reveal a confounding variety of adverse drug reactions (ADRs) affecting an increasing range of organs and organ systems. Some of these reactions are relatively common; however many tend to be delayed in onset, infrequent and immune mediated. This combination of factors underpins present day challenges in identifying and subsequently reporting these types of ADRs in clinical practice as well as in spontaneous reporting programs.The integration of various data sources in this present review indicates the utility of common pharmacovigilance approaches to generate meaningful signals to improve the safe use of common drugs such as metoprolol.
One of the main immune-mediated toxicities linked to metoprolol is dermatological adverse events, specifically lichenoid drug eruption and pemphigus foliaceus. These responses are noteworthy for their reliance on clinicopathological association for identification and for their delayed presentation, which frequently happens weeks to months after medication initiation. From the perspective of an ADR study, causality classification is strengthened by positive temporal correlation, dechallenge response, and rejection of alternate etiologies. Metoprolol may function as a trigger rather than a direct toxicant due to the autoimmune character of pemphigus foliaceus, underscoring the significance of early detection and long-term drug cessation.
Metoprolol-related cardiovascular damage is largely context-dependent. Pharmacovigilance studies show that starting β-blockade during acutely decompensated heart failure myocarditis, or shock might cause severe hemodynamic worsening, even while it reduces mortality in stable chronic heart failure. ADRs may result from improper clinical timing rather than improper dosage, as the COVID-19-associated myocarditis example demonstrates. Similarly, overdose-related toxicity highlights the importance of extracorporeal life support in refractory shock and exposes the shortcomings of traditional diagnostic indicators, particularly when prolonged-release formulations and co-ingestion with calcium channel blockers are involved.
Metoprolol's safety profile is further expanded by adverse drug reactions (ADRs) related to neurological, hypersensitivity, and drug-drug interactions. While rapid hypersensitivity reactions are uncommon but have a significant risk of morbidity, CNS effects are often vague and prone to misattribution. Pharmacogenomic knowledge and cautious medication reconciliation are important because drug-drug interactions, especially those mediated by CYP2D6 suppression, are an avoidable source of adverse drug reactions.
All of these results support the idea that metoprolol-related adverse drug reactions (ADRs) should be evaluated within an organized pharmacovigilance framework that includes proactive reporting, consistent causality evaluation, and MedDRA-based classification. To improve risk characterisation, guide better prescription practices, and stop preventable patient damage, such a strategy is crucial.
CONCLUSION
Acute cardiovascular decompensation, severe immune-mediated dermatological disease, mild neurological symptoms, and potentially fatal overdose toxicity are all included in the wide clinical spectrum of metoprolol-associated adverse medication events. Despite the rarity of these occurrences, increased clinical attention is required due to their potential severity and delayed presentation. This ADR-focused pharmacovigilance review shows that rather than being solely dose-dependent, many significant events are situational, immune-mediated, or interaction-driven.
Positive results depend on early detection, timely drug discontinuation, and appropriate supportive or immunosuppressive medication When giving metoprolol to patients who are hemodynamically unstable, have an autoimmune tendency, are taking interfering drugs, or are at danger of overdosing, clinicians should be more cautious. To enhance signal detection and improve the benefit-risk profile of metoprolol, robust ADR reporting using standardized MedDRA language and ongoing post-marketing surveillance are crucial.
In the end, using pharmacovigilance principles in everyday clinical decision-making will make patients safer while keeping the big therapeutic benefits of metoprolol in cardiovascular medicine.
REFERENCES









Suraj Ambale, Sujit Karande, Ayush Shendage, Pratiksha Kamble, Shweta Patil, Dr. Shobhraj Malavi, Dr. Pratik Maske, Umesh Kolap, Sandip Biradar, Adverse Drug Reactions Associated with Metoprolol: An Adr Study and Pharmacovigilance Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 3852-3863, https://doi.org/10.5281/zenodo.20715352
 10.5281/zenodo.20715352
10.5281/zenodo.20715352