
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmaceutical Quality Assurance, Samarth Institute of Pharmacy Belhe. Maharashtra¹,²,³
Department of Pharmaceutical Quality Assurance, Samarth Institute of Pharmacy Belhe. Maharashtra?,?,?
Avacopan is a novel, orally administered selective complement 5a receptor (C5aR) antagonist that has emerged as an important therapeutic option for the treatment of antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV). AAV is a group of rare autoimmune diseases characterized by inflammation and destruction of small blood vessels, particularly affecting organs such as the kidneys and lungs. Conventional treatment strategies primarily rely on high-dose glucocorticoids combined with immunosuppressive agents; however, prolonged steroid use is associated with significant adverse effects, including osteoporosis, diabetes, hypertension, and increased risk of infections. In this context, avacopan represents a targeted and steroid-sparing therapeutic alternative that acts on a specific component of the complement system.
INTRODUCTION
Analytical method development plays a crucial role in pharmaceutical quality control to ensure the safety, efficacy, and stability of drug products. Reverse Phase High Performance Liquid Chromatography (RP-HPLC) is one of the most widely used analytical techniques for quantitative drug estimation due to its precision, accuracy, and reproducibility.
Avacopan is a selective complement 5a receptor (C5aR) antagonist used in the treatment of anti-neutrophil cytoplasmic antibody (ANCA)–associated vasculitis. It was approved by the U.S. Food and Drug Administration in 2021 and marketed under the brand name Tavneos.
Avacopan is chemically known as a complement 5a receptor inhibitor with immunomodulatory action. As a relatively new drug molecule, limited literature is available regarding simple, cost-effective, and stability-indicating RP-HPLC methods for routine quality control analysis.
Therefore, the present research aims to develop and validate a simple, accurate, precise, and stability-indicating RP-HPLC method for the quantitative estimation of Avacopan in bulk and pharmaceutical dosage forms in accordance with International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use guidelines.
Drug Profile- Avacopan:
Anti-neutrophil cytoplasmic (auto)antibody (ANCA)-associated vasculitis (AAV) is a rare (estimated incidence of 3 cases per 100,000 per year) form of "pauci-immune" systemic small-vessel vasculitis typified by the presence of ANCAs in the serum. The full spectrum of AAV includes granulomatosis with polyangiitis (GPA), microscopic polyangiitis (MPA), eosinophilic granulomatosis with polyangiitis (EGPA), and drug-induced AAV. AAV may be associated with necrotizing and crescentic glomerulonephritis (NCGN). Despite complex pathophysiology, studies over the past ~2 decades have identified a key role for the alternative complement pathway and, in particular, the interaction between the anaphylatoxin fragment C5a and its cognate C5aR receptor in AAV. Avacopan (formerly CCX168) is an allosteric C5aR antagonist indicated for use in AAV.
Avacopan was granted FDA approval on October 8, 2021, and is currently marketed under the name TAVNEOS by ChemoCentryx, On January 19, 2022, the European Commission approved avacopan for the treatment of adult patients with severe, active granulomatosis polyangiitis (GPA) or microscopic polyangiitis (MPA) - the two main forms of ANCA-associated vasculitis - in combination with rituximab or cyclophosphamide.10 Avacopan was approved by Health Canada on April 20, 2022.
Structure of Avacopan:
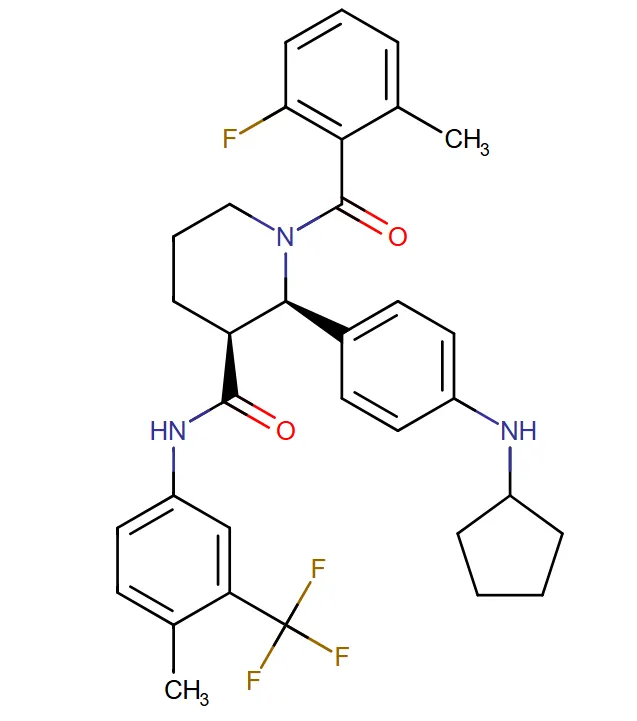
Chemical Formula: C33H35F4N3O2
Indication: Avacopan is indicated for the adjunctive treatment of adult patients with severe active anti-neutrophil cytoplasmic autoantibody (ANCA)-associated vasculitis (granulomatosis with polyangiitis and microscopic polyangiitis; GPA/MPA) in combination with standard therapy including glucocorticoids. Avacopan does not eliminate the need for glucocorticoids.
Pharmacodynamics: Avacopan is a complement 5a receptor (C5aR) antagonist that blocks C5a-induced upregulation of C11b (integrin alpha M) on neutrophils and inhibits C5a-mediated neutrophil activation and migration. Avacopan has been associated with hypersensitivity reactions, including angioedema, and hepatotoxicity, as evidenced by elevated liver transaminases. Likely due to its effect on the complement pathway, avacopan has also been associated with hepatitis B virus reactivation and serious infections, which should be monitored for as appropriate.
Absorption:
Avacopan exhibits favorable pharmacokinetic properties following oral administration. It is rapidly absorbed, with peak plasma concentrations typically reached within 1 to 2 hours. The extent of absorption is enhanced when the drug is taken with food, particularly high-fat meals, which increase systemic exposure. Once absorbed, avacopan undergoes extensive hepatic metabolism, primarily mediated by cytochrome P450 enzymes, especially CYP3A4. It is converted into several metabolites, among which the M1 metabolite is pharmacologically active and contributes significantly to the overall therapeutic effect. Due to its dependence on CYP3A4, avacopan is susceptible to drug interactions, with enzyme inhibitors increasing its plasma concentration and enzyme inducers reducing its efficacy
Metabolism: Avacopan is metabolized primarily by CYP3A4. The major circulating M1 metabolite, a mono-hydroxylated form of avacopan, represents ~12% of drug plasma levels and acts as a C5aR antagonist with similar efficacy to avacopan itself.
Route of Elimination: The elimination of avacopan occurs predominantly via the fecal route, accounting for approximately 77% of the administered dose, while urinary excretion plays a minor role, contributing less than 10%.
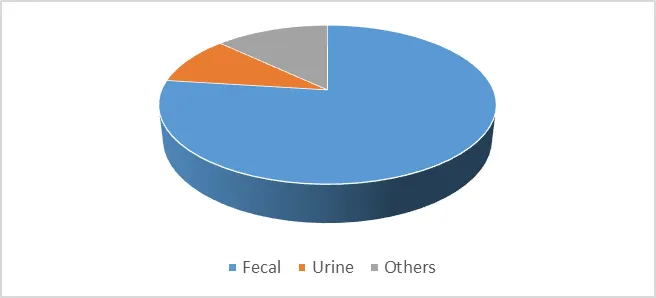
Fig. 1: Distribution of elimination pathways of avacopan
This indicates that biliary excretion is the primary pathway for drug elimination. The drug has an elimination half-life ranging from 10 to 20 hours, which supports a twice-daily dosing regimen and ensures sustained inhibition of the complement 5a receptor over a 24-hour period. Clearance of avacopan is moderate and mainly depends on hepatic metabolism, and therefore may be affected in patients with impaired liver function or in the presence of drugs that alter CYP3A4 activity.
Half-Life: A single 30 mg dose of avacopan given with food to healthy subjects resulted in mean elimination half-lives of 97.6 and 55.6 hours for avacopan and its M1 metabolite, respectively.
t1/2= 0.693k
Clearance: Avacopan exhibits moderate systemic clearance, which is primarily dependent on hepatic metabolism rather than renal excretion. The drug is extensively metabolized in the liver via cytochrome P450 enzymes, especially CYP3A4, and this metabolic process plays a major role in determining its clearance from the body. Since renal elimination is minimal, kidney function has little impact on the overall clearance of avacopan. However, hepatic function is a critical factor; any impairment in liver activity can reduce drug clearance and lead to increased systemic exposure. Additionally, co-administration of drugs that inhibit or induce CYP3A4 can significantly alter the clearance rate, either slowing it down and increasing the risk of toxicity or accelerating it and reducing therapeutic efficacy. Thus, avacopan clearance is largely governed by liver metabolism and is sensitive to both physiological and drug-related factors.
Toxicity:
Avacopan is generally well tolerated, with a safety profile that is favorable compared to conventional glucocorticoid therapy. Common adverse effects include nausea, headache, fatigue, and upper respiratory tract infections. Some patients may experience elevations in liver enzymes, indicating potential hepatotoxicity, which necessitates periodic monitoring of liver function during treatment. Additionally, there is a risk of infections due to its immunomodulatory mechanism, although severe adverse events are relatively uncommon. Importantly, avacopan significantly reduces the risk of long-term steroid-related toxicities such as osteoporosis, diabetes, hypertension, and weight gain, making it a safer alternative for long-term management of ANCA-associated vasculitis.
Mechanism of Action
Avacopan selectively inhibits the complement 5a receptor (C5aR), blocking the interaction between C5a and its receptor.
It Inhibits neutrophil activation and migration Reduces inflammation and vascular damage
Prevents release of proteolytic enzymes and free radicals C5a is a potent pro-inflammatory mediator responsible for neutrophil chemotaxis and activation. By blocking this pathway, avacopan reduces tissue injury without affecting the membrane attack complex.
Pharmacokinetics
Pharmacokinetically, avacopan demonstrates favorable properties suitable for oral administration. It is rapidly absorbed following ingestion, with peak plasma concentrations typically achieved within one to two hours. Ct=C0e-kt
The drug exhibits a half-life of approximately 10 to 20 hours, allowing for twice-daily dosing. Avacopan undergoes hepatic metabolism primarily via cytochrome P450 enzymes and is predominantly eliminated through the fecal route. These characteristics contribute to sustained receptor inhibition over a 24-hour period, ensuring consistent therapeutic effects.
Fig. 1: Distribution of elimination pathways of avacopan
Clinical efficacy & Safety
The clinical efficacy of avacopan has been well established through pivotal clinical trials, particularly the Phase III ADVOCATE study.
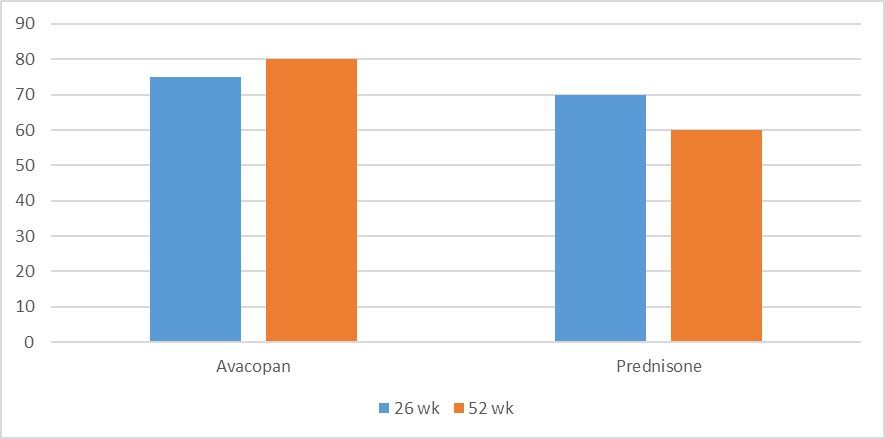
Fig. 3: Comparison of remission rates between avacopan and prednisone at 26 and 52 weeks
This randomized, controlled trial compared avacopan with standard glucocorticoid therapy in patients with granulomatosis with polyangiitis (GPA) and microscopic polyangiitis (MPA). The results demonstrated that avacopan was non-inferior to prednisone in achieving remission at 26 weeks and superior in maintaining sustained remission at 52 weeks. Additionally, patients receiving avacopan experienced significantly lower glucocorticoid-related toxicity and showed improved renal outcomes, including better estimated glomerular filtration rate (eGFR). These findings highlight the potential of avacopan to transform the current treatment paradigm for AAV.
In terms of safety, avacopan is generally well tolerated, with a safety profile comparable to conventional therapy. Common adverse effects include nausea, headache, fatigue, and upper respiratory tract infections. Some patients may experience elevated liver enzymes, necessitating periodic monitoring of hepatic function during treatment. Although there is a potential risk of infections due to immune modulation, no major safety concerns have been identified in clinical trials, making avacopan a relatively safer alternative to long-term glucocorticoid therapy.
Pharmaceutical quality assurance perspective
The development and validation of avacopan formulations require strict adherence to regulatory guidelines. Critical Quality Attributes (CQAs) for avacopan include assay accuracy, purity, dissolution characteristics, and stability under various environmental conditions. Analytical methods such as reverse-phase high-performance liquid chromatography (RP-HPLC) are commonly employed for quantitative estimation and impurity profiling. Method validation is conducted in accordance with International Council for Harmonisation (ICH) guidelines, particularly ICH Q2(R1), covering parameters such as accuracy, precision, linearity, specificity, and robustness. y = mx + c ?
These measures ensure the reliability, reproducibility, and consistency of analytical results.
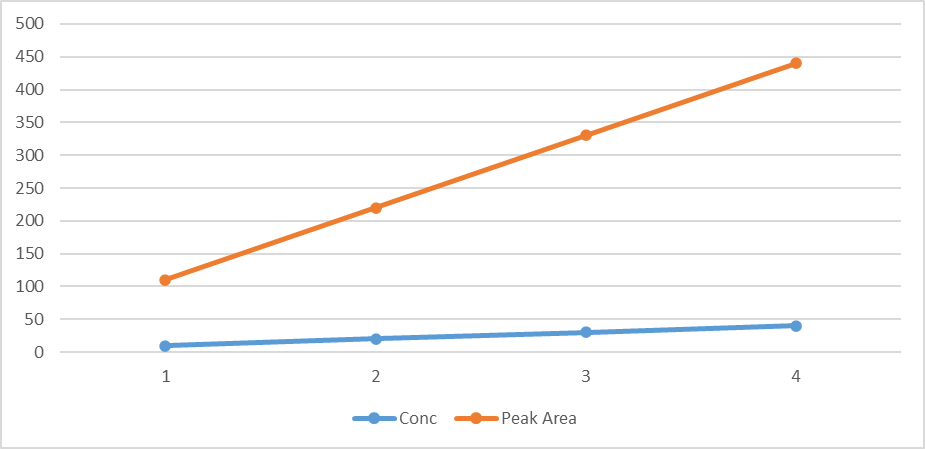
Fig. 4: Calibration curve showing linear relationship between concentration and peak area of avacopan
CONCLUSION
Avacopan represents a significant advancement in the management of ANCA-associated vasculitis by introducing a targeted therapeutic approach that inhibits the complement 5a receptor pathway. Unlike conventional glucocorticoid-based therapies, avacopan provides effective disease control while minimizing the risk of steroid-related adverse effects. Its favorable pharmacokinetic profile, including good oral absorption, hepatic metabolism via CYP3A4, and predominant fecal elimination, supports its clinical utility and convenient dosing regimen. Clinical evidence, particularly from the ADVOCATE trial, has demonstrated its non-inferiority in inducing remission and superiority in maintaining sustained remission, along with improved renal outcomes and reduced toxicity.
From a pharmaceutical quality assurance perspective, the development of avacopan requires stringent adherence to regulatory guidelines and validated analytical methods to ensure product quality, safety, and efficacy. Validation parameters such as accuracy, precision, linearity, specificity, robustness, LOD, and LOQ are well justified through previously reported research studies, confirming the reliability of analytical techniques like RP-HPLC and LC-MS/MS for its estimation. Stability studies and forced degradation analyses further support the development of stability-indicating methods, which are essential for lifecycle management of the drug.
Overall, avacopan offers a promising steroid-sparing alternative with improved safety and efficacy profiles. However, continued research, long-term clinical data, and post-marketing surveillance are necessary to fully establish its role in broader clinical applications and ensure sustained therapeutic benefits.
REFERENCES

Omkar Gosavi, Sachin Bhalekar, Ganesh Lamkhade, Rahul Lokhande, Komal Aher, Kuldeep Ramteke, Avacopan in ANCA-Associated Vasculitis: Pharmacology, Clinical Profile, and Analytical Method Validation Perspectives, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 5, 7313-7321. https://doi.org/10.5281/zenodo.20410659
 10.5281/zenodo.20410659
10.5281/zenodo.20410659