
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmacy, Faculty of Medical Paramedical and Allied Health Science, Jagannath University, Jaipur, Rajasthan, 303901, India
Chronic diseases such as diabetes mellitus, chronic obstructive pulmonary disease (COPD), chronic kidney disease, cardiovascular disorders, and asthma are among the leading causes of morbidity and mortality worldwide. Patients suffering from these long-term illnesses are more vulnerable to infections because of reduced immunity, repeated hospital visits, prolonged medication use, and associated com-plications. As a result, antibiotics are frequently prescribed in the management of chronic disease patients for both therapeutic and preventive purposes. Although antibiotics play a major role in control-ling infections and improving patient outcomes, irrational and excessive use of these drugs has become a major public health concern. Inappropriate prescribing practices, unnecessary use of broad-spectrum antibiotics, polypharmacy, and lack of adherence to treatment guidelines contribute significantly to antimicrobial resistance, adverse drug reactions, increased healthcare costs, and poor quality of patient care. Therefore, evaluating the utilization pattern of antibiotics in chronic disease patients has become essential for promoting rational drug therapy and ensuring safe and effective treatment. The present study focuses on the comprehensive evaluation of antibiotic utilization in patients with chronic diseases in a hospital setting. The study aims to analyse prescribing patterns, identify the most commonly used antibiotics, assess the rationality of prescriptions, and evaluate the extent of polypharmacy among patients. The research also emphasizes the importance of World Health Organization (WHO) prescribing indica-tors in assessing the rational use of medicines. Data for the study are collected from patient case records, prescriptions, laboratory reports, and treatment charts over a defined study period. Various parameters such as patient demographics, diagnosis, type of chronic disease, name of antibiotic prescribed, dosage form, route of administration, frequency, duration of therapy, and combination therapy are ana-lysed systematically. Special attention is given to the use of generic prescribing, culture sensitivity testing, and adherence to standard treatment guidelines.
Antibiotics are one of the greatest discoveries in modern medicine and have played a major role in reducing morbidity and mortality caused by infectious diseases. Since the discovery of penicillin by Alexander Fleming in 1928, antibiotics have become an essential part of healthcare systems worldwide. These drugs are used for the prevention and treatment of bacterial infections and have significantly im-proved patient survival and quality of life. Antibiotics are commonly prescribed in hospitals, clinics, and community healthcare settings for various infectious conditions such as respiratory tract infections, urinary tract infections, skin infections, gastrointestinal infections, and postoperative infections. Their proper use has transformed medical practice by making surgeries, organ transplantation, chemotherapy, and intensive care treatments safer and more effective.
Antibiotics are substances that either kill bacteria or inhibit their growth. They act through different mechanisms such as inhibition of bacterial cell wall synthesis, protein synthesis, nucleic acid synthesis, and metabolic pathways. Based on their mechanism of action and spectrum of activity, antibiotics are classified into several groups including penicillins, cephalosporins, macrolides, tetracyclines, amino-glycosides, fluoroquinolones, sulfonamides, and carbapenems. The selection of an appropriate antibi-otic depends on various factors such as type of infection, causative organism, patient condition, severity of disease, and microbial sensitivity pattern.
Chronic diseases are long-term medical conditions that generally progress slowly and require continuous medical care and management. Common chronic diseases include diabetes mellitus, hypertension, cardiovascular diseases, chronic kidney disease, chronic obstructive pulmonary disease (COPD), asthma, arthritis, and cancer. According to the World Health Organization, chronic diseases are among the leading causes of death and disability worldwide. The prevalence of chronic illnesses has increased significantly due to urbanization, aging population, unhealthy lifestyle, physical inactivity, smoking, alcohol consumption, stress, and poor dietary habits. Patients suffering from chronic diseases are more vulnerable to infections because of weakened immunity, impaired organ function, repeated hospitalization, and long-term medication use. For example, diabetic patients are more prone to skin infections, urinary tract infections, and diabetic foot infections, while patients with chronic respiratory diseases such as COPD frequently develop respiratory tract infections. Similarly, chronic kidney disease patients are at increased risk of infections due to reduced immune response and dialysis-related complications. As a result, antibiotics are commonly prescribed in chronic disease patients to manage bacterial infections and prevent complications.
Although antibiotics provide significant therapeutic benefits, their irrational and excessive use has be-come a major global healthcare concern. In many healthcare settings, antibiotics are prescribed unnecessarily or inappropriately without proper diagnosis or confirmation of bacterial infection. Broad-spectrum antibiotics are often used empirically without culture sensitivity testing, which contributes to the development of antimicrobial resistance. Inappropriate dose selection, prolonged duration of therapy, self-medication, incomplete treatment courses, and over-the-counter availability of antibiotics further increase the problem of irrational antibiotic use.
Antimicrobial resistance is one of the most serious public health challenges faced globally today. Anti-biotic resistance occurs when bacteria develop the ability to survive and grow even in the presence of antibiotics that were previously effective against them. Resistant microorganisms make infections difficult to treat and may lead to prolonged illness, treatment failure, increased hospitalization, and higher healthcare costs. The emergence of multidrug-resistant organisms such as methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant enterococci, and multidrug-resistant tuberculosis has created a major burden on healthcare systems worldwide. The misuse and overuse of antibiotics are considered the primary causes of antimicrobial resistance. In developing countries like India, irrational antibiotic use is more common because of lack of awareness, inadequate healthcare facilities, poor infection control practices, and easy availability of medicines without prescription. Many patients discontinue antibiotics once symptoms improve or use leftover antibiotics without medical advice. Such practices reduce the effectiveness of antibiotics and increase resistance among microorganisms. Patients with chronic diseases are particularly vulnerable to the complications associated with irrational antibi-otic use because they often receive multiple medications simultaneously. Polypharmacy increases the risk of drug interactions, adverse drug reactions, and medication errors. Certain antibiotics may interact with antidiabetic drugs, anticoagulants, antihypertensive agents, and nephrotoxic drugs, resulting in harmful effects. Elderly patients with chronic illnesses are at even greater risk due to age-related de-cline in organ function and altered drug metabolism. Adverse drug reactions associated with antibiotics are another important concern in healthcare practice. Antibiotics may cause mild adverse effects such as nausea, vomiting, diarrhea, and skin rashes, or severe reactions including nephrotoxicity, hepatotoxicity, ototoxicity, hypersensitivity reactions, and anaphylaxis. Monitoring antibiotic safety and preventing adverse reactions are essential components of rational drug therapy. Pharmacovigilance programs help identify and evaluate adverse drug reactions and improve patient safety.
Drug utilization studies are important tools for evaluating the prescribing patterns, effectiveness, safety, and rationality of antibiotic use. These studies help identify inappropriate prescribing habits, unnecessary use of broad-spectrum antibiotics, excessive duration of therapy, and non-adherence to treatment guidelines. Drug utilization research also provides information regarding patient compliance, adverse drug reactions, and healthcare costs. Such studies are essential for improving prescribing practices and promoting rational drug use.
The World Health Organization has developed prescribing indicators to assess the quality and rationality of prescribing practices in healthcare settings. These indicators include the average number of drugs prescribed per encounter, percentage of encounters with antibiotics prescribed, use of generic medicines, and adherence to essential medicine lists. Evaluation of these indicators helps healthcare professionals identify irrational prescribing trends and implement corrective measures. Clinical pharmacists play a major role in promoting the rational use of antibiotics and improving patient care. They are in-volved in prescription review, monitoring of adverse drug reactions, identification of drug interactions, dose adjustment, patient counseling, and participation in antimicrobial stewardship programs. The involvement of clinical pharmacists in healthcare teams can significantly reduce medication errors and improve therapeutic outcomes in chronic disease patients.
Antimicrobial stewardship programs are organized efforts designed to optimize antibiotic therapy and reduce antimicrobial resistance. These programs encourage appropriate antibiotic selection, dosing, route of administration, and duration of therapy. Implementation of stewardship programs in hospitals has been shown to reduce irrational antibiotic use, decrease resistance rates, improve patient outcomes, and lower healthcare costs.
Public awareness regarding proper antibiotic use is also essential to control antimicrobial resistance. Patients should be educated about the importance of completing antibiotic courses, avoiding self-medication, and not using antibiotics for viral infections such as common cold and influenza. Healthcare professionals should also follow evidence-based treatment guidelines and prescribe antibiotics only when necessary. The present study focuses on evaluating the utilization pattern of antibiotics in chronic disease patients and assessing the rationality of antibiotic prescribing practices. The study also aims to identify adverse drug reactions, drug interactions, and factors influencing antibiotic use. Under-standing antibiotic prescribing trends and utilization patterns can help healthcare professionals improve rational prescribing practices and reduce the burden of antimicrobial resistance. Therefore, rational use of antibiotics is essential for ensuring effective treatment, minimizing adverse effects, improving pa-tient safety, and preventing the emergence of resistant microorganisms. Continuous monitoring, phar-macovigilance, patient education, and antimicrobial stewardship are necessary to promote safe and ef-fective antibiotic therapy in chronic disease patient.
2. NEED OF THE STUDY
Antibiotics are among the most important discoveries in modern medicine because they have significantly reduced illness and death caused by bacterial infections. They are widely used in hospitals, clinics, and community healthcare settings for the treatment and prevention of infectious diseases. In patients suffering from chronic diseases such as diabetes mellitus, chronic kidney disease, chronic obstructive pulmonary disease (COPD), cardiovascular disorders, and asthma, antibiotics are frequently prescribed because these patients are more vulnerable to infections due to weakened immunity and long-term illness. Although antibiotics are highly beneficial when used properly, their irrational and excessive use has become a major global healthcare concern. In recent years, the misuse and overuse of antibiotics have increased rapidly. Many patients receive antibiotics without proper diagnosis, culture sensitivity testing, or medical indication. In some cases, antibiotics are prescribed unnecessarily for viral infections such as the common cold, influenza, and fever, where they provide no therapeutic benefit. Self-medication, incomplete antibiotic courses, incorrect dose selection, and easy availability of antibiotics without prescription are also major contributors to irrational antibiotic use. These practices not only reduce the effectiveness of antibiotics but also increase the risk of antibiotic resistance, adverse drug reactions, treatment failure, prolonged hospitalization, and increased healthcare costs. Patients with chronic diseases require special attention regarding antibiotic therapy because they often receive multiple medications for the management of their primary illness. The simultaneous use of several drugs increases the possibility of drug interactions and adverse drug reactions. For example, diabetic patients receiving antibiotics may experience altered blood glucose levels, while patients with kidney or liver diseases may develop toxicity due to impaired drug elimination. Elderly patients with chronic diseases are at even higher risk because of reduced organ function and polypharmacy. Therefore, careful monitoring of antibiotic use in such patients is extremely important. Antibiotic resistance has emerged as one of the most serious public health challenges worldwide. Resistance occurs when bacteria change their structure or behavior in response to repeated exposure to antibiotics, making the drugs less effective or completely ineffective. Resistant microorganisms lead to severe infections that are difficult to treat and may require stronger, more expensive, and more toxic antibiotics. According to the World Health Organization, antimicrobial resistance is one of the top global threats to public health. The development of multidrug-resistant organisms has increased morbidity, mortality, and healthcare expenditure across the world. In developing countries like India, irrational antibiotic use is particularly common because of lack of awareness, inadequate healthcare facilities, poor infection control practices, and easy access to medicines without proper prescription.
Drug utilization studies play an important role in evaluating the prescribing patterns, safety, effective-ness, and rationality of antibiotic use. Such studies help in identifying inappropriate prescribing habits, unnecessary use of broad-spectrum antibiotics, excessive duration of therapy, and deviations from standard treatment guidelines. They also provide useful information regarding the frequency of adverse drug reactions, patient compliance, and cost-effectiveness of treatment. By analyzing prescribing trends, healthcare professionals can develop strategies to improve rational antibiotic use and reduce resistance. Clinical pharmacists have an important role in promoting the safe and effective use of antibiotics. They help physicians in selecting appropriate antibiotics, monitoring drug interactions, preventing adverse drug reactions, educating patients, and ensuring adherence to treatment guidelines. The involvement of clinical pharmacists in antibiotic stewardship programs can improve patient outcomes and minimize irrational prescribing practices. Therefore, studying antibiotic utilization patterns can al-so highlight the importance of clinical pharmacy services in healthcare settings.
Another important reason for conducting this study is the increasing burden of chronic diseases world-wide. Lifestyle changes, unhealthy diet, lack of physical activity, smoking, alcohol consumption, stress, and aging population have contributed to a rise in chronic illnesses. Patients suffering from chronic dis-eases are more likely to develop recurrent infections, leading to frequent exposure to antibiotics. Continuous exposure to antibiotics increases the possibility of bacterial resistance and treatment complications. Hence, there is a need to evaluate whether antibiotics are being prescribed rationally and accord-ing to standard guidelines in chronic disease patients. This study is also necessary to create awareness among healthcare professionals and patients regarding the responsible use of antibiotics. Many patients discontinue antibiotics once symptoms improve, while others demand antibiotics even when not re-quired. Lack of awareness regarding proper antibiotic use contributes significantly to resistance development. By understanding the current prescribing patterns and associated problems, effective educational and preventive measures can be implemented.
Furthermore, evaluating antibiotic use patterns helps healthcare institutions formulate antibiotic policies and stewardship programs aimed at optimising therapy and minimising resistance. The findings of this study may assist policymakers, physicians, pharmacists, and healthcare authorities in improving prescribing practices and ensuring patient safety. Therefore, the present study is needed to assess the utilisation pattern of antibiotics in chronic disease patients, identify irrational prescribing practices, evaluate drug interactions and adverse drug reactions, and promote rational antibiotic therapy. The study will contribute to better healthcare management, improved patient outcomes, and control of anti-biotic resistance in the community.
3. OBJECTIVES OF STUDY
The main objective of this study is to evaluate the utilization pattern of antibiotics in patients suffering from chronic diseases and to understand how antibiotics are being prescribed and used in healthcare settings. Chronic diseases such as diabetes mellitus, hypertension, chronic kidney disease, cardiovascular diseases, asthma, and chronic obstructive pulmonary disease (COPD) often weaken the immune system of patients, making them more susceptible to infections. Due to this reason, antibiotics are commonly prescribed in such patients for the prevention and treatment of bacterial infections. However, inappropriate and excessive use of antibiotics has become a major healthcare concern worldwide. Therefore, this study aims to assess whether antibiotics are being prescribed rationally according to standard treatment guidelines and clinical requirements.
Another important objective of the study is to identify the most commonly prescribed antibiotics in chronic disease patients and evaluate their frequency of use. The study also focuses on understanding the factors that influence antibiotic prescribing patterns, including disease condition, severity of infection, physician preference, patient condition, and hospital policies. By studying prescribing trends, the research can help identify irrational prescribing practices such as unnecessary use of broad-spectrum antibiotics, incorrect dose selection, prolonged duration of therapy, and polypharmacy. The study further aims to evaluate the rational and irrational use of antibiotics using standard prescribing indicators recommended by the World Health Organization. These indicators help in assessing the quality of pre-scribing practices and identifying areas where improvement is needed. The study also intends to analyze the average number of drugs prescribed per prescription, percentage of antibiotics prescribed, use of generic medicines, and adherence to essential medicine lists.
Patients with chronic diseases usually receive multiple medications simultaneously for long-term management of their illness. Therefore, another major objective of the study is to identify possible drug interactions associated with antibiotic therapy. Drug interactions may alter the therapeutic effect of medicines and increase the risk of complications. The study also focuses on identifying adverse drug reactions (ADRs) caused by antibiotics, such as allergic reactions, gastrointestinal disturbances, nephrotoxicity, hepatotoxicity, and other side effects. Monitoring adverse drug reactions is important to ensure patient safety and improve therapeutic outcomes. This study also aims to evaluate the role of clinical pharmacists in promoting the rational use of antibiotics. Clinical pharmacists can contribute significantly by reviewing prescriptions, monitoring therapy, identifying drug interactions, counseling patients, and participating in antimicrobial stewardship programs. Their involvement can help reduce medication errors, prevent irrational prescribing, and improve the effectiveness of treatment. Another important objective of the study is to understand the relationship between irrational antibiotic use and the development of antibiotic resistance. Antibiotic resistance is one of the major public health challenges faced globally. Overuse, misuse, self-medication, and incomplete antibiotic courses contribute to the emergence of resistant microorganisms, making infections difficult to treat. Through this study, aware-ness regarding appropriate antibiotic use and antimicrobial resistance can be increased among healthcare professionals and patients.
Finally, the study aims to provide recommendations for improving antibiotic prescribing practices, encouraging rational drug use, minimizing adverse effects, and reducing antibiotic resistance. The findings of this research may help healthcare institutions, physicians, pharmacists, and policymakers develop effective strategies for safe and effective antibiotic therapy in chronic disease patients.
4. CLASSIFICATION AND MECHANISM OF ANTIBIOTICS
Antibiotics are chemical substances used to kill or inhibit the growth of microorganisms, especially bacteria. They play a very important role in the prevention and treatment of infectious diseases.(Fig.1) Antibiotics may be obtained naturally from microorganisms, produced semi-synthetically by modifying natural compounds, or synthesised completely in laboratories. Since the discovery of penicillin by Alexander Fleming, antibiotics have revolutionised medical science and significantly reduced mortality caused by bacterial infections. Antibiotics are widely used in hospitals and community healthcare set-tings for the treatment of respiratory tract infections, urinary tract infections, gastrointestinal infections, skin infections, septicemia, tuberculosis, and many other bacterial diseases.
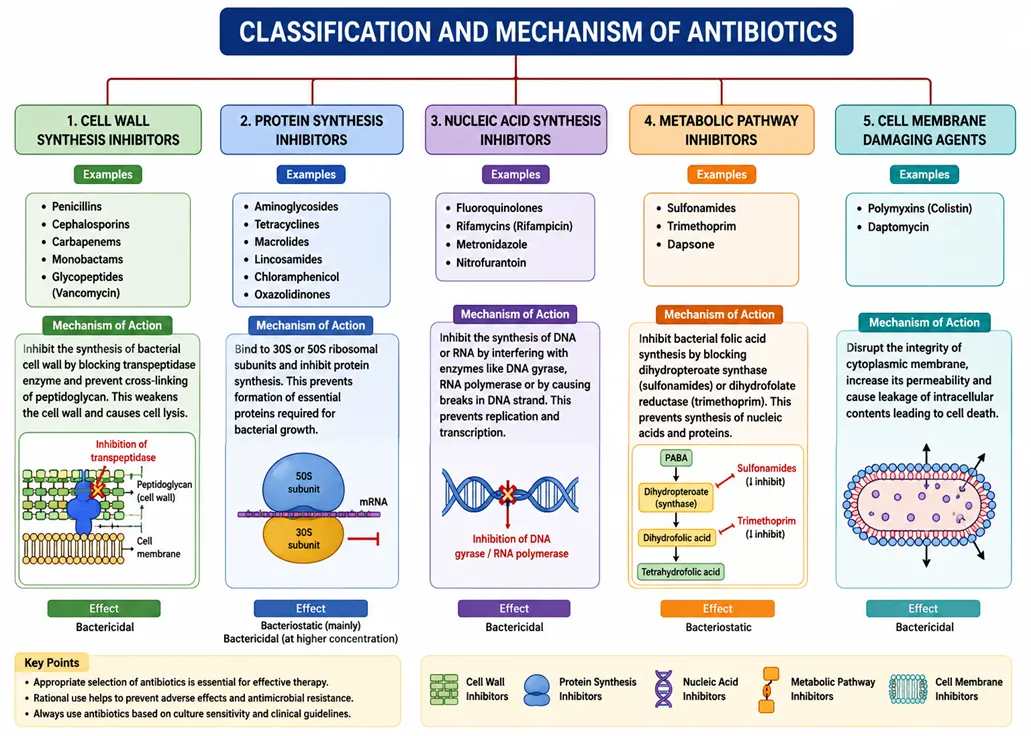
Figure 1: Classification and mechanism of antibiotics
The proper selection and use of antibiotics are essential because irrational use can lead to adverse drug reactions, treatment failure, and antibiotic resistance. Antibiotics are classified on the basis of their chemical structure, mechanism of action, spectrum of activity, and effect on bacteria. Understanding the classification and mechanism of antibiotics is important for rational prescribing and effective patient care. One of the major classifications of antibiotics is based on their mechanism of action. According to this classification, antibiotics are divided into cell wall synthesis inhibitors, protein synthesis inhibitors, nucleic acid synthesis inhibitors, antimetabolites, and cell membrane inhibitors. Cell wall syn-thesis inhibitors are among the most commonly used antibiotics. These antibiotics interfere with the formation of the bacterial cell wall, which is essential for bacterial survival. Because human cells do not have a cell wall, these drugs selectively act on bacteria and are considered relatively safe. The most important group under this category is beta-lactam antibiotics, which include penicillins, cephalosporins, carbapenems, and monobactams. Penicillins such as amoxicillin and penicillin G inhibit the synthesis of peptidoglycan, an important component of the bacterial cell wall. As a result, the bacterial cell becomes weak and undergoes lysis. Cephalosporins are classified into different generations depending on their antimicrobial activity. First-generation cephalosporins are more effective against gram-positive bacteria, while later generations show greater activity against gram-negative organisms. Carbapenems such as imipenem and meropenem are broad-spectrum antibiotics used for severe infections. Another important cell wall inhibitor is vancomycin, which belongs to the glycopeptide class and is effective against resistant gram-positive bacteria such as methicillin-resistant Staphylococcus aureus (MRSA).
Another important class of antibiotics is protein synthesis inhibitors. These antibiotics act by binding to bacterial ribosomes and interfering with protein synthesis, which is essential for bacterial growth and multiplication. Bacterial ribosomes differ structurally from human ribosomes, allowing selective toxicity. Protein synthesis inhibitors are divided into drugs acting on the 30S ribosomal subunit and those acting on the 50S ribosomal subunit. Aminoglycosides such as gentamicin, amikacin, and streptomycin bind to the 30S subunit and cause misreading of messenger RNA, leading to defective protein formation and bacterial death. Tetracyclines such as doxycycline and tetracycline also bind to the 30S subunit and inhibit the attachment of transfer RNA to the ribosome, thereby preventing protein synthesis. Macrolides such as erythromycin and azithromycin act on the 50S ribosomal subunit and inhibit the translocation process during protein synthesis. Chloramphenicol inhibits peptidyl transferase enzyme activity on the 50S subunit, while clindamycin inhibits peptide chain elongation. Linezolid is another important protein synthesis inhibitor used for resistant gram-positive infections.
Antibiotics that inhibit nucleic acid synthesis form another important category. These antibiotics inter-fere with bacterial DNA replication or RNA transcription, ultimately preventing bacterial multiplication. Fluoroquinolones such as ciprofloxacin, levofloxacin, and moxifloxacin inhibit bacterial DNA gyrase and topoisomerase IV enzymes, which are essential for DNA replication and repair. Rifampicin inhibits bacterial RNA polymerase and is widely used in the treatment of tuberculosis. Metronidazole causes DNA strand breakage in anaerobic bacteria and protozoa, leading to cell death. Because of their mechanism, these drugs are highly effective in severe and complicated infections.
Antimetabolite antibiotics act by interfering with bacterial metabolic pathways. Sulfonamides and trimethoprim are important examples of this group. These drugs inhibit the synthesis of folic acid, which is necessary for bacterial growth and DNA synthesis. Sulfonamides compete with para-aminobenzoic acid for the enzyme dihydropteroate synthase, whereas trimethoprim inhibits dihydrofolate reductase. When used together as cotrimoxazole, they produce a synergistic effect and are commonly used in urinary tract infections, respiratory infections, and opportunistic infections. Cell membrane inhibitors are another category of antibiotics. These drugs disrupt the integrity of the bacterial cell membrane, leading to leakage of cellular contents and bacterial death. Polymyxins such as polymyxin B and colistin are mainly active against gram-negative bacteria and are often used as last-resort drugs for multidrug-resistant infections. Daptomycin is another membrane-active antibiotic effective against resistant gram-positive organisms. Antibiotics can also be classified according to their spectrum of activity into broad-spectrum and narrow-spectrum antibiotics. Broad-spectrum antibiotics are effective against a wide variety of gram-positive and gram-negative bacteria. Examples include tetracyclines, chloramphenicol, and carbapenems. These drugs are useful when the causative organism is unknown, but excessive use can disturb normal microbial flora and increase the risk of resistance. Narrow-spectrum antibiotics act against specific groups of bacteria. For example, penicillin G is mainly effective against gram-positive bacteria. Narrow-spectrum antibiotics are preferred whenever possible because they reduce the risk of superinfection and resistance. Another classification is based on the effect of antibiotics on bacteria. Bactericidal antibiotics kill bacteria directly, while bacteriostatic antibiotics inhibit bacterial growth and allow the immune system to eliminate the organisms. Penicillins, cephalosporins, aminoglycosides, fluoroquinolones, and vancomycin are examples of bactericidal antibiotics. Tetracyclines, macrolides, and sulfonamides are generally bacteriostatic antibiotics. The choice between bactericidal and bacterio-static drugs depends on the type and severity of infection, immune status of the patient, and site of infection. Antibiotics are also classified according to their chemical structure. Major classes include beta-lactams, aminoglycosides, tetracyclines, macrolides, glycopeptides, quinolones, sulfonamides, lincosamides, oxazolidinones, and polymyxins. Each class has unique pharmacological properties, spectrum of activity, adverse effects, and clinical uses. Beta-lactam antibiotics contain a beta-lactam ring in their structure and are among the safest and most widely prescribed antibiotics. Aminoglycosides are highly effective against aerobic gram-negative bacteria but may cause nephrotoxicity and ototoxicity. Tetracyclines are broad-spectrum antibiotics commonly used in acne, respiratory infections, and sexually transmitted diseases. Macrolides are frequently used in respiratory tract infections because of their good tissue penetration and safety profile.
The mechanism of antibiotics is closely related to antibiotic resistance. Bacteria develop resistance through various mechanisms such as enzyme production, alteration of target sites, reduced drug permeability, and active efflux pumps. For example, beta-lactamase enzymes produced by bacteria destroy beta-lactam antibiotics and make them ineffective. Methicillin-resistant Staphylococcus aureus develops resistance by altering penicillin-binding proteins. Resistance has become a major global health concern due to irrational prescribing, self-medication, incomplete therapy, and overuse of antibiotics in humans and animals. Therefore, understanding the classification and mechanism of antibiotics is essential for rational drug use and prevention of resistance.
5. EPIDEMIOLOGY OF CHRONIC DISEASE
Chronic diseases are long-lasting health conditions that usually develop slowly and continue for a long period of time, often throughout a person’s life. These diseases require continuous medical care, regular monitoring, lifestyle modifications, and long-term treatment for proper management. Unlike acute dis-eases, which occur suddenly and recover within a short period, chronic diseases progress gradually and may lead to serious complications if not managed properly. Today, chronic diseases have become one of the biggest public health challenges worldwide because they are responsible for a large number of deaths, disabilities, and healthcare expenses.
Common chronic diseases include diabetes mellitus, hypertension, cardiovascular diseases, chronic kidney disease, chronic respiratory diseases such as asthma and chronic obstructive pulmonary disease (COPD), cancer, obesity, arthritis, and stroke. These diseases affect millions of people across the world and significantly reduce the quality of life of patients. Chronic diseases not only affect physical health but also create emotional, social, and economic burdens on individuals, families, and healthcare systems.
According to the World Health Organization, chronic diseases, also known as non-communicable dis-eases (NCDs), are responsible for the majority of deaths globally. Cardiovascular diseases are considered the leading cause of death among chronic illnesses, followed by cancer, respiratory diseases, and diabetes mellitus. The increasing prevalence of chronic diseases has become a serious concern because these conditions are now affecting both developed and developing countries at an alarming rate.
One of the major reasons behind the rapid increase in chronic diseases is modernization and urbanization. In today’s fast-moving lifestyle, people are becoming more dependent on unhealthy dietary habits, processed foods, and sedentary lifestyles. Lack of physical activity, obesity, smoking, alcohol consumption, mental stress, and inadequate sleep have significantly contributed to the development of chronic diseases. Urban populations are especially more affected because of changing work patterns, reduced exercise, and unhealthy food consumption.
In India, the burden of chronic diseases has increased dramatically during the last few decades. Earlier, infectious diseases were considered the major health problem in India, but now non-communicable dis-eases have become equally important. Rapid industrialization, changing lifestyle patterns, environmental pollution, and increasing stress levels have contributed to the rise in chronic illnesses among both urban and rural populations. India is often referred to as the “diabetes capital of the world” because of the large number of diabetic patients present in the country. Diabetes mellitus is highly prevalent due to unhealthy food habits, obesity, physical inactivity, and genetic susceptibility.
Hypertension is another common chronic disease affecting millions of people in India. High blood pressure is considered a silent disease because many patients remain unaware of their condition until com-plications occur. Uncontrolled hypertension increases the risk of heart attack, stroke, kidney failure, and other cardiovascular complications. Similarly, cardiovascular diseases such as coronary artery disease and heart failure have become major causes of death due to unhealthy lifestyle habits, smoking, stress, obesity, and lack of exercise. Chronic respiratory diseases such as asthma and COPD are also highly prevalent, especially in polluted urban environments. Air pollution, smoking, occupational exposure to dust and chemicals, indoor smoke from cooking fuels, and environmental allergens contribute significantly to respiratory illnesses. COPD is more common among smokers and elderly individuals, while asthma can affect people of all age groups.
Cancer is another major chronic disease that continues to increase worldwide. Factors such as tobacco use, alcohol consumption, environmental pollution, unhealthy diet, radiation exposure, and genetic pre-disposition contribute to the development of different types of cancer. Early diagnosis and proper treatment are essential for improving survival rates and reducing complications associated with cancer.
The epidemiology of chronic diseases shows that these conditions are more common among elderly populations because aging is associated with decreased organ function, weakened immunity, and in-creased vulnerability to diseases. However, in recent years, chronic diseases are increasingly being ob-served among younger individuals as well. Poor dietary habits, obesity, stress, lack of physical activity, excessive screen time, and unhealthy lifestyles have made young adults more prone to conditions such as obesity, hypertension, and diabetes mellitus. Socioeconomic status also plays an important role in the epidemiology of chronic diseases. People belonging to lower socioeconomic groups often have limited access to healthcare facilities, nutritious food, health education, and preventive services. Poor living conditions, unemployment, stress, and lack of awareness may further increase the risk of chronic dis-eases. On the other hand, excessive consumption of processed foods and sedentary lifestyles in higher-income groups also contribute to disease development.
Genetic and hereditary factors are equally important in the development of chronic diseases. Individuals with a family history of diabetes, hypertension, heart disease, or cancer are more likely to develop similar conditions. Environmental factors such as pollution, occupational hazards, and unhealthy life-style choices further increase disease risk in genetically susceptible individuals.
Patients suffering from chronic diseases are more vulnerable to infections because their immunity is often weakened due to long-term illness and continuous medication use. Frequent hospitalization and invasive procedures may further increase infection risk. As a result, antibiotics are commonly pre-scribed in chronic disease patients for the treatment and prevention of bacterial infections. For example, diabetic patients are more prone to urinary tract infections, skin infections, and diabetic foot infections, while COPD patients frequently develop respiratory tract infections.
Repeated use of antibiotics in chronic disease patients may increase the risk of antimicrobial resistance, adverse drug reactions, and drug interactions. Many chronic disease patients receive multiple medications simultaneously, leading to polypharmacy and increased chances of medication-related complications. Therefore, rational antibiotic use and proper monitoring are essential for improving patient safety and therapeutic outcomes. The economic burden of chronic diseases is extremely high. Long-term treatment, regular medical check-ups, hospitalization, laboratory investigations, surgeries, and lifelong medication increase healthcare expenses significantly. Chronic diseases also reduce work productivity and may lead to disability, affecting both individuals and society. In many families, long-term treatment costs create financial stress and reduce quality of life. Prevention and early management are important strategies for reducing the burden of chronic diseases. Healthy lifestyle modifications such as balanced diet, regular exercise, smoking cessation, stress management, and routine health check-ups can help prevent many chronic conditions. Early diagnosis and proper treatment can reduce complications and improve quality of life. Public awareness programs and health education also play an important role in disease prevention and control.
Epidemiological studies of chronic diseases are essential for understanding disease distribution, prevalence, incidence, risk factors, and healthcare needs within populations. These studies help healthcare professionals and policymakers develop effective prevention programs, treatment guidelines, and healthcare policies. They also support rational prescribing practices and improve healthcare planning. Clinical pharmacists, physicians, nurses, and other healthcare professionals play a significant role in managing chronic diseases through patient counseling, medication monitoring, adverse drug reaction reporting, and promoting rational drug therapy. Proper healthcare management and patient education are essential to reduce disease burden and improve overall public health outcomes.
6. OVERVIEW OF CHRONIC DISEASE
Chronic Diseases are long-lasting medical conditions that usually develop slowly and continue for months or years. These diseases are among the leading causes of illness, disability, and death world-wide. Unlike acute diseases, which appear suddenly and last for a short period, chronic diseases progress gradually and often require long-term medical care, lifestyle modification, and continuous monitoring. Chronic diseases affect people of all age groups, but they are more common among older adults because the risk increases with age. Rapid urbanization, unhealthy lifestyle habits, poor dietary pat-terns, lack of physical activity, smoking, alcohol consumption, stress, and environmental pollution are some major factors responsible for the increasing prevalence of chronic diseases globally. According to global health reports, chronic diseases contribute significantly to healthcare costs and place a major burden on families, healthcare systems, and national economies. Chronic diseases are generally classified into communicable chronic diseases and non-communicable chronic diseases, although non-communicable diseases are far more common. Major chronic diseases include diabetes mellitus, hyper-tension, cardiovascular diseases, chronic kidney disease, chronic respiratory diseases, arthritis, asthma, chronic obstructive pulmonary disease, cancer, neurological disorders, thyroid disorders, and liver dis-eases. These diseases often coexist in the same patient, a condition known as comorbidity, which further complicates treatment and management. Patients with chronic diseases frequently require multiple medications for long durations, increasing the chances of drug interactions, adverse drug reactions, and poor medication adherence. One of the most common chronic diseases is Diabetes Mellitus, a metabolic disorder characterized by high blood glucose levels due to insufficient insulin production or impaired insulin action. Diabetes can lead to severe complications such as nephropathy, neuropathy, retinopathy, cardiovascular disease, and diabetic foot infections. Patients with diabetes are more susceptible to infections because high blood sugar weakens the immune system. As a result, antibiotics are commonly prescribed for diabetic patients suffering from urinary tract infections, skin infections, respiratory infections, and wound infections. Another important chronic disease is Hypertension, which is characterized by persistently elevated blood pressure. Hypertension is often called a “silent killer” because it may not show symptoms in the early stages but can lead to serious complications such as stroke, heart attack, kidney failure, and heart failure. Long-term uncontrolled hypertension damages blood vessels and organs, especially the heart, brain, and kidneys. Patients with hypertension often require lifelong treatment with antihypertensive drugs along with dietary and lifestyle modifications.
Cardiovascular diseases are another major category of chronic diseases and include coronary artery dis-ease, heart failure, arrhythmias, and stroke. These conditions are mainly caused by atherosclerosis, obesity, smoking, diabetes, hypertension, and sedentary lifestyle. Cardiovascular diseases are among the leading causes of mortality worldwide. Patients suffering from heart diseases may develop secondary infections during hospitalization or invasive procedures, requiring antibiotic therapy. Careful selection of antibiotics is necessary because some antibiotics may interact with cardiovascular drugs or produce cardiac side effects. Chronic Kidney Disease is a progressive and irreversible loss of kidney function over time. CKD may develop due to diabetes, hypertension, glomerulonephritis, or prolonged use of nephrotoxic drugs. As kidney function declines, waste products accumulate in the body, leading to complications such as anemia, electrolyte imbalance, metabolic acidosis, and cardiovascular problems. Patients with chronic kidney disease are more prone to infections because of weakened immunity and frequent hospital exposure. Antibiotic therapy in CKD patients requires dose adjustment because im-paired kidney function affects drug excretion and increases the risk of toxicity.
Chronic respiratory diseases such as asthma and Chronic Obstructive Pulmonary Disease are also common chronic illnesses. Asthma is characterized by airway inflammation and bronchoconstriction, while COPD is associated with chronic airflow limitation caused mainly by smoking and environmental pollutants. Patients with respiratory diseases frequently experience bacterial respiratory infections, which often require antibiotic treatment. However, irrational antibiotic use in respiratory illnesses contributes significantly to antibiotic resistance. Cancer is another serious chronic disease involving uncontrolled growth and spread of abnormal cells. Cancer patients often have weakened immunity due to the disease itself or chemotherapy, making them highly susceptible to infections. Antibiotics are commonly used in cancer patients to prevent and treat bacterial infections. Proper antibiotic selection is essential to avoid complications and improve patient survival. Chronic diseases have several common characteristics. They are usually permanent or long-lasting, progress slowly, and often require continuous treatment and follow-up. Most chronic diseases cannot be completely cured but can be controlled through medication, healthy lifestyle changes, regular exercise, balanced diet, stress management, and avoidance of harmful habits such as smoking and alcohol consumption. Early diagnosis and proper management are important to prevent complications and improve quality of life.
The burden of chronic diseases is increasing rapidly due to population aging and lifestyle changes. Urbanization and modernization have led to reduced physical activity, increased consumption of pro-cessed foods, obesity, and stress, all of which contribute to chronic disease development. In developing countries, lack of healthcare awareness, poor access to medical facilities, and inadequate treatment fur-ther worsen disease outcomes. Chronic diseases not only affect physical health but also create psycho-logical, social, and financial problems for patients and families. In patients with chronic diseases, infections are common because immunity is often weakened. Therefore, antibiotics are frequently prescribed either for treatment or prevention of infections. However, irrational use of antibiotics in chronic disease patients can lead to antibiotic resistance, treatment failure, adverse drug reactions, and increased healthcare costs. Polypharmacy is another major issue in chronic diseases because patients usually take several medications simultaneously. This increases the risk of drug interactions between antibiotics and chronic disease medications. Careful monitoring and rational prescribing are therefore essential. Healthcare professionals, especially clinical pharmacists, play an important role in the management of chronic diseases. They help in medication counseling, monitoring adverse drug reactions, improving patient adherence, and promoting rational use of antibiotics. Public awareness regarding healthy life-style habits, regular health checkups, vaccination, and early treatment can help reduce the burden of chronic diseases.
7. ANTIBIOTICS USE IN CHRONIC DISEASE
Antibiotics are one of the most commonly prescribed medicines in the treatment and management of chronic diseases. Chronic diseases are long-term health conditions that usually progress slowly and re-quire continuous medical care. Common chronic diseases include Diabetes Mellitus, Chronic Kidney Disease, cardiovascular diseases, asthma, Chronic Obstructive Pulmonary Disease, cancer, arthritis, and chronic liver diseases. Patients suffering from these conditions are more likely to develop infections because their immune system becomes weak due to disease progression, aging, poor nutrition, or long-term medication use. For this reason, antibiotics are frequently used to treat bacterial infections and prevent complications in chronic disease patients. (Table 1) Antibiotics are medicines that either kill bacteria or stop their growth. They are very important in preventing serious infections and improving patient survival. In chronic diseases, infections can worsen the patient’s condition and increase the risk of hospitalization, organ damage, and death. Therefore, timely and appropriate antibiotic therapy plays a major role in patient management. However, irrational or unnecessary use of antibiotics can lead to adverse drug reactions and antibiotic resistance, which has become a major global health concern.
In diabetic patients, infections are very common because high blood sugar levels reduce the ability of white blood cells to fight microorganisms. Diabetes also affects blood circulation and delays wound healing, increasing the risk of bacterial infections. Common infections seen in diabetic patients include urinary tract infections, skin infections, diabetic foot ulcers, respiratory tract infections, and gum infections. Diabetic foot infection is one of the most serious complications because it may lead to tissue damage, gangrene, and amputation if not treated properly. Antibiotics are prescribed based on the se-verity of infection and the type of bacteria involved. Mild infections may be treated with oral antibiotics, while severe infections often require intravenous broad-spectrum antibiotics and hospitalization. Proper blood glucose control along with antibiotic therapy is necessary for better healing and prevention of complications.
In Chronic Kidney Disease patients, the risk of infection is very high because kidney dysfunction weakens the immune system. Frequent hospital visits, dialysis procedures, and catheter use further increase the chances of bacterial infections. Common infections in CKD patients include urinary tract infections, respiratory infections, bloodstream infections, and catheter-related infections. Antibiotic therapy in kidney disease patients requires careful monitoring because many antibiotics are eliminated through the kidneys. If renal function is impaired, drugs may accumulate in the body and cause toxicity. Therefore, dose adjustment is necessary for antibiotics such as aminoglycosides, vancomycin, and cephalosporins. Some antibiotics may also worsen kidney damage, so nephrotoxic drugs should be used cautiously. Regular monitoring of kidney function tests is important during treatment. Patients with chronic respiratory diseases such as asthma and Chronic Obstructive Pulmonary Disease often suffer from repeated respiratory infections. In COPD, bacterial infections are a major cause of disease exacerbation, leading to symptoms like cough, breathlessness, chest tightness, and sputum production. Antibiotics such as macrolides, penicillins, tetracyclines, and fluoroquinolones are commonly used to manage respiratory infections. These drugs help reduce inflammation, improve symptoms, and prevent complications. However, antibiotics should only be used when bacterial infection is suspected because unnecessary use in viral infections increases antibiotic resistance.
Cancer patients are another group in which antibiotics play a vital role. Chemotherapy and radiotherapy weaken the immune system and reduce white blood cell count, making patients highly susceptible to infections. Even minor infections can become life-threatening in cancer patients. Broad-spectrum anti-biotics are often started immediately when fever develops because delayed treatment may lead to septicemia and death. Combination antibiotic therapy is commonly used in severe infections involving resistant bacteria. Proper infection control and timely antibiotic use are essential to improve survival in cancer patients. In cardiovascular diseases, antibiotics are sometimes used to prevent infections during surgeries or invasive procedures. Patients undergoing heart valve replacement, angiography, or catheterization may receive prophylactic antibiotics to prevent bacterial infections such as infective endo-carditis. Careful antibiotic selection is necessary because some antibiotics may interact with cardiovascular drugs or produce cardiac side effects such as arrhythmias.
Patients with chronic liver disease are also at increased risk of infections because liver dysfunction affects immunity and protein synthesis. Common infections include spontaneous bacterial peritonitis, urinary tract infections, and respiratory infections. Antibiotics are commonly used to control these infections and reduce complications. However, liver disease affects drug metabolism, so dose adjustment and monitoring are important during therapy.
One important issue in chronic disease management is polypharmacy, which means the use of multiple medicines at the same time. Chronic disease patients often take several drugs daily for long durations. When antibiotics are added to therapy, the risk of drug interactions and adverse effects increases. For example, some antibiotics may increase or decrease the effect of blood thinners, antidiabetic drugs, or antihypertensive medicines. Therefore, careful monitoring by healthcare professionals is essential. Antibiotic resistance is one of the biggest problems associated with antibiotic use in chronic diseases. Resistance develops when bacteria become less sensitive or completely resistant to antibiotics due to re-peated and irrational use. Self-medication, incomplete antibiotic courses, overuse of broad-spectrum antibiotics, and unnecessary prescribing are major causes of resistance. Resistant infections are difficult to treat and may require stronger, more expensive drugs with more side effects. Multidrug-resistant bacteria such as MRSA and resistant gram-negative organisms are increasingly seen in hospitals and chronic disease patients. To reduce resistance, antibiotics should be used only when necessary and according to proper guidelines. Adverse drug reactions are another major concern during antibiotic therapy. Common side effects include nausea, vomiting, diarrhea, allergic reactions, skin rashes, nephrotoxicity, hepatotoxicity, and ototoxicity. Elderly patients and patients with chronic diseases are more vulnerable because of reduced organ function and multiple medication use. Therefore, monitoring patient response and educating patients about side effects are important parts of therapy. The role of healthcare professionals, especially clinical pharmacists, is very important in promoting rational antibiotic use. Clinical pharmacists help in selecting appropriate antibiotics, adjusting doses, checking drug interactions, monitoring adverse effects, and counseling patients regarding medication adherence. They also educate patients about completing the full course of antibiotics and avoiding self-medication. Antibiotic steward-ship programs in hospitals help promote rational prescribing and reduce antibiotic resistance. Lifestyle modifications and preventive measures can also reduce the need for antibiotics in chronic diseases. Good hygiene, vaccination, healthy diet, regular exercise, blood sugar control, smoking cessation, and regular medical checkups help strengthen immunity and reduce infections. Early diagnosis and proper management of chronic diseases are important for preventing complications and improving quality of life.
8. RATIONAL AND IRRATIONAL USE OF ANTIBIOTICS
Antibiotics are among the most important medicines used in modern healthcare for the treatment and prevention of bacterial infections. They have saved millions of lives since their discovery and continue to play a major role in medical practice. However, the effectiveness of antibiotics depends greatly on how they are used. The correct and scientific use of antibiotics is known as rational use, while inappropriate or unnecessary use is called irrational use. Rational antibiotic use is essential for effective treatment, patient safety, and prevention of antibiotic resistance. On the other hand, irrational use of antibiotics has become a serious global health problem and is one of the main causes of increasing antibiotic resistance. Rational use of antibiotics means that patients receive the right antibiotic, at the correct dose, for the appropriate duration, and according to their clinical condition( Fig- 2).
In rational therapy, the antibiotic is selected based on the type of infection, the suspected or identified microorganism, patient age, body weight, organ function, allergy history, and severity of disease. Rational prescribing aims to achieve maximum therapeutic benefit with minimum side effects and mini-mum development of resistance. Proper diagnosis and laboratory investigations such as culture and sensitivity tests are important parts of rational antibiotic use because they help identify the causative bacteria and determine which antibiotic will be most effective. In rational antibiotic therapy, doctors first evaluate whether the infection is bacterial, viral, fungal, or noninfectious. Antibiotics are useful only against bacterial infections and should not be used for viral illnesses such as the common cold, influenza, or most sore throats. When antibiotics are prescribed unnecessarily for viral infections, there is no clinical benefit to the patient, but the risk of resistance and side effects increases. Rational use also in-volves choosing narrow-spectrum antibiotics whenever possible because they target specific bacteria and reduce damage to normal body flora. Broad-spectrum antibiotics should be reserved for severe infections or when the causative organism is unknown. The duration of antibiotic therapy is another important aspect of rational use. Antibiotics should be taken for the full prescribed course even if symptoms improve earlier. Stopping treatment too soon may not eliminate bacteria and can lead to recur-rence of infection and development of resistant organisms. Similarly, overuse of antibiotics for longer durations than necessary should also be avoided because it increases toxicity and resistance. Proper dosing intervals and routes of administration are equally important to maintain effective drug concentration in the body. The World Health Organisation promotes rational antibiotic use through treatment guidelines and antibiotic stewardship programs. These programs encourage evidence-based prescribing, regular monitoring, infection control, and patient education. Rational antibiotic use helps reduce healthcare costs, minimises adverse drug reactions, shortens hospital stays, and improves treatment out-comes. It also preserves the effectiveness of antibiotics for future generations.
In contrast, irrational use of antibiotics refers to inappropriate, excessive, or incorrect use of these medicines. Irrational use occurs when antibiotics are prescribed without proper indication, used in wrong doses, taken for incorrect duration, or selected without considering bacterial sensitivity. Self-medication, over-the-counter availability, unnecessary use of broad-spectrum antibiotics, and misuse in viral infections are common examples of irrational antibiotic use. In many developing countries, anti-biotics are easily available without a prescription, which increases the risk of misuse.
One of the most common forms of irrational use is prescribing antibiotics for viral infections such as cough, cold, fever, and flu. Since antibiotics do not work against viruses, such use provides no benefit but exposes patients to unnecessary risks. Another example is polypharmacy, where multiple antibiotics are prescribed together without a clear indication. Excessive use of injections instead of oral antibiotics is also considered irrational when oral therapy is sufficient. Irrational antibiotic use is especially common in patients with chronic diseases such as Diabetes Mellitus, Chronic Kidney Disease, and Chronic Obstructive Pulmonary Disease because these patients frequently develop infections and require repeat-ed medical treatment. Sometimes antibiotics are prescribed unnecessarily as a preventive measure without evidence of bacterial infection. Repeated exposure to antibiotics in chronic disease patients in-creases the chances of resistant infections and adverse drug reactions. Antibiotic resistance is the most serious consequence of irrational antibiotic use. Resistance occurs when bacteria adapt and become capable of surviving antibiotic treatment. Resistant bacteria are difficult to treat and may require stronger, more expensive, and more toxic medicines. Common resistant organisms include MRSA, multidrug-resistant tuberculosis, and resistant gram-negative bacteria. Antibiotic resistance increases morbidity, mortality, duration of hospitalisation, and healthcare costs worldwide.
It has become a major public health challenge because the development of new antibiotics is much slower than the spread of resistance. Irrational use of antibiotics can also lead to several adverse drug reactions. Common side effects include nausea, vomiting, diarrhoea, allergic reactions, skin rashes, nephrotoxicity, hepatotoxicity, and ototoxicity. Overuse of broad-spectrum antibiotics can disturb normal microbial flora and cause superinfections such as fungal infections and pseudomembranous colitis. Elderly patients and patients with kidney or liver diseases are at greater risk because impaired organ function affects drug metabolism and excretion. Several factors contribute to irrational antibiotic use. Lack of awareness among patients, inadequate knowledge among healthcare providers, pressure from patients demanding antibiotics, self-medication, pharmaceutical promotion, poor infection control practices, and lack of diagnostic facilities are important causes. In some areas, incomplete antibiotic courses due to financial problems or early symptom relief are also common. These practices further increase resistance and treatment failure. Healthcare professionals, especially clinical pharmacists, play a major role in promoting rational antibiotic use. They help in selecting appropriate antibiotics, checking drug interactions, adjusting doses, monitoring adverse effects, and educating patients regarding proper medication use. Patient counselling is very important because many people stop antibiotics once symptoms improve or use leftover medicines without medical advice. Educating patients about completing the full course and avoiding self-medication can significantly reduce misuse.

Figure. 2 Rational and irrational use of antibiotics
9.TYPES OF ANTIBIOTICS
Antibiotic resistance is the ability of microorganisms such as bacteria to survive and grow even in the presence of antibiotics that were previously effective against them. It has become one of the most serious global public health problems because resistant bacteria make infections difficult to treat, increase the risk of complications, prolong hospitalization, and raise healthcare costs. Antibiotic resistance mainly develops due to irrational antibiotic use, overuse of broad-spectrum antibiotics, incomplete treatment courses, self-medication, and poor infection control practices.
Understanding the different types of antibiotic resistance is important for proper treatment and prevention of resistant infections.(Fig. 3)

Figure:3 Mechanisms of Antibiotic Resistance in Bacteria
9.1. Intrinsic Resistance
Intrinsic resistance, also known as natural resistance, is the inherent ability of certain bacteria to resist the action of specific antibiotics due to their structural or functional characteristics. This type of resistance is naturally present in bacteria and is not acquired through mutation or gene transfer. For ex-ample, Gram-negative bacteria are naturally resistant to some antibiotics because their outer membrane prevents drug entry into the bacterial cell. Similarly, some bacteria lack the target site on which certain antibiotics act, making the drug ineffective. Intrinsic resistance is stable and predictable in nature.
9.2. Acquired Resistance
Acquired resistance develops when previously sensitive bacteria become resistant to antibiotics due to genetic changes. This type of resistance may occur through mutation in bacterial DNA or by acquiring resistance genes from other bacteria. Acquired resistance is one of the major causes of treatment failure in infectious diseases. It commonly develops because of irrational antibiotic use, prolonged therapy, and inappropriate dosing. Resistant bacteria can spread rapidly among individuals and healthcare set-tings, creating serious public health challenges.
9.3. Mutation-Mediated Resistance
In this type of resistance, spontaneous mutations occur in bacterial genetic material, altering the target site of the antibiotic or changing bacterial metabolic pathways. These genetic mutations reduce the effectiveness of antibiotics and allow bacteria to survive. Repeated exposure to antibiotics increases the chances of selecting mutated resistant bacteria. Mutation-mediated resistance is commonly observed with antibiotics such as rifampicin and fluoroquinolones.
9.4. Resistance by Gene Transfer
Bacteria can transfer resistance genes from one organism to another through various mechanisms such as conjugation, transformation, and transduction. This transfer allows resistant bacteria to spread resistance traits rapidly among bacterial populations. Plasmids carrying resistance genes are commonly involved in this process. Gene transfer plays a major role in the development of multidrug-resistant organisms in hospitals and communities.
9.5. Cross Resistance
Cross-resistance occurs when resistance to one antibiotic also produces resistance to another antibiotic belonging to the same class or having a similar mechanism of action. For example, bacteria resistant to one macrolide antibiotic may also show resistance to other macrolides. This type of resistance limits therapeutic options and complicates infection management.
9.6. Multidrug Resistance (MDR)
Multidrug resistance refers to the ability of bacteria to resist multiple antibiotics from different classes simultaneously. Multidrug-resistant organisms are difficult to treat and often require stronger, more ex-pensive, and more toxic medications. Common examples include methicillin-resistant Staphylococcus aureus (MRSA) and multidrug-resistant tuberculosis (MDR-TB). MDR has become a major healthcare concern worldwide due to increasing antibiotic misuse.
9.7. Extensive Drug Resistance (XDR)
Extensively drug-resistant bacteria are resistant to almost all available antibiotics except a few limited treatment options. XDR infections are associated with high morbidity and mortality because therapeutic choices become extremely limited. This type of resistance is mainly observed in severe hospital-acquired infections and tuberculosis cases.
9.8. Pan Drug Resistance (PDR)
Pan drug resistance is the most severe form of antibiotic resistance in which bacteria become resistant to all available antimicrobial agents. In such cases, no effective antibiotic treatment remains available, making infections extremely difficult or impossible to cure. PDR poses a major threat to global healthcare systems.
According to the World Health Organization, antibiotic resistance is increasing rapidly due to misuse and overuse of antibiotics. Prevention of resistance requires rational antibiotic prescribing, patient counseling, infection control measures, vaccination, antimicrobial stewardship programs, and public awareness regarding proper antibiotic use. Clinical pharmacists and healthcare professionals play an important role in monitoring antibiotic therapy and promoting safe medication practices.
Therefore, understanding the various types of antibiotic resistance is essential for improving treatment outcomes, preventing the spread of resistant bacteria, and ensuring the effective use of antibiotics in healthcare settings.
10. PUBLIC HEALTH CHALLENGES DUE TO ANTIBIOTICS RESISTANT
Antibiotic resistance has become one of the biggest public health challenges in the modern world. Antibiotics were once considered miracle medicines because they successfully treated many serious bacterial infections and saved millions of lives. However, due to the overuse and misuse of antibiotics, many bacteria have now become resistant to these medicines. This means that antibiotics no longer work effectively against certain infections, making treatment more difficult and dangerous. Antibiotic resistance affects not only individual patients but also the entire healthcare system and society. One of the major public health challenges caused by antibiotic resistance is the difficulty in treating common infections. Diseases such as pneumonia, urinary tract infections, tuberculosis, skin infections, and blood-stream infections are becoming harder to cure because resistant bacteria do not respond to normal anti-biotic therapy. As a result, patients may suffer from prolonged illness, severe complications, and higher risk of death. In some cases, doctors are forced to use stronger and more expensive antibiotics that may cause more side effects.
Antibiotic resistance also increases the spread of infections in hospitals and communities. Resistant bacteria can easily spread from one patient to another through direct contact, contaminated surfaces, poor hygiene, or improper infection control practices. Hospitals are especially at high risk because many patients have weak immunity and require frequent antibiotic treatment. Healthcare-associated infections caused by resistant bacteria have become a serious problem worldwide. Patients suffering from chronic diseases such as Diabetes Mellitus, Chronic Kidney Disease, cancer, and Chronic Obstructive Pulmonary Disease are more vulnerable to resistant infections because their immune systems are often weakened. Elderly people, children, and critically ill patients are also at greater risk. In these patients, resistant infections may lead to repeated hospitalization, treatment failure, and increased mortality. Another important challenge is the economic burden caused by antibiotic resistance. Resistant infections usually require longer hospital stays, repeated laboratory investigations, and expensive medicines. This increases healthcare costs for patients, hospitals, and governments. In developing countries, limited healthcare facilities and lack of awareness make the problem even more serious. Poor sanitation, overcrowding, and easy availability of antibiotics without prescription further contribute to resistance.
Antibiotic resistance also threatens many medical procedures that depend on effective antibiotics. Surgeries, organ transplantation, chemotherapy, dialysis, and intensive care treatments all require antibiotics to prevent and control infections. If antibiotics become ineffective, these medical procedures may become more risky and less successful. One of the major reasons behind antibiotic resistance is irrational antibiotic use. Many people use antibiotics without a doctor’s prescription, stop treatment early, skip doses, or use antibiotics for viral infections such as cold and flu. Inappropriate prescribing, self-medication, and overuse of broad-spectrum antibiotics are common causes of resistance. In some areas, antibiotics are also overused in animals and agriculture, which contributes to the spread of resistant bacteria. Public health systems face difficulties in controlling antibiotic resistance because the development of new antibiotics is very slow. Many pharmaceutical companies are producing fewer new anti-biotics due to high research costs and limited profit. As resistance continues to grow, treatment options become limited. To overcome these challenges, rational use of antibiotics is very important. Antibiotics should only be used when necessary and according to medical advice. Doctors should prescribe antibiotics carefully based on proper diagnosis and culture sensitivity reports whenever possible. Completing the full course of treatment and avoiding self-medication are essential steps in preventing resistance. Healthcare professionals, especially clinical pharmacists, play a major role in promoting responsible antibiotic use. Antibiotic stewardship programs, infection control measures, vaccination, public aware-ness campaigns, and proper hygiene practices are also important strategies to reduce resistance and protect public health.
11. FACTOR AFFECTING ANTIBIOTICS PRESCRIBING PATTERN
Antibiotic prescribing patterns refer to how antibiotics are selected and prescribed by doctors to treat infections. Antibiotics are very important medicines because they help in treating bacterial infections and preventing complications. However, the prescribing of antibiotics is influenced by many different factors related to the patient, doctor, hospital, and healthcare system. Proper antibiotic prescribing is necessary for successful treatment and prevention of antibiotic resistance. Irrational prescribing can lead to treatment failure, side effects, increased healthcare costs, and development of resistant bacteria. One of the main factors affecting antibiotic prescribing patterns is the type and severity of infection. Doctors decide the antibiotic based on the site and seriousness of infection. Mild infections may require simple oral antibiotics, while severe infections such as pneumonia, septicemia, or meningitis may need strong intravenous broad-spectrum antibiotics. In emergency conditions, doctors often start empirical antibiotic therapy before laboratory reports are available to control the infection quickly and prevent complications. The condition and characteristics of the patient also influence antibiotic prescribing. Age is an important factor because children and elderly patients require special attention during antibiotic therapy. Their body functions are different from healthy adults, so dose adjustment may be necessary. Pregnancy and breastfeeding also affect antibiotic selection because some antibiotics may harm the baby. Kidney and liver function are very important because many antibiotics are metabolized or excreted through these organs. Patients with kidney or liver disease may develop toxicity if antibiotics are not prescribed carefully.
Patients suffering from chronic diseases such as Diabetes Mellitus, Chronic Kidney Disease, heart dis-ease, asthma, and Chronic Obstructive Pulmonary Disease are more prone to infections due to weak immunity and long-term illness. These patients often require repeated antibiotic therapy. Doctors must carefully choose antibiotics in such patients because they may already be taking multiple medicines, increasing the risk of drug interactions and adverse effects. In chronic kidney disease patients, dose adjustment is especially important because impaired kidney function reduces drug excretion. Another major factor affecting antibiotic prescribing is laboratory diagnostic facilities. Culture and sensitivity testing helps identify the bacteria responsible for infection and determine which antibiotic will work best. When laboratory facilities are available, doctors can prescribe antibiotics more accurately and rationally. However, in many rural hospitals or primary healthcare centers, laboratory support may be limited or unavailable. In such cases, antibiotics are prescribed based mainly on clinical symptoms and doctor experience, which may sometimes lead to irrational prescribing.
Doctor’s knowledge, experience, and prescribing habits also play an important role. Doctors who are updated with treatment guidelines and antibiotic resistance patterns are more likely to prescribe antibiotics rationally. Experienced physicians may identify infections more accurately and avoid unnecessary antibiotic use. On the other hand, lack of awareness or outdated knowledge may result in excessive use of broad-spectrum antibiotics. Some doctors prefer stronger antibiotics because they want quick recovery or fear treatment failure. Patient expectations and demands also affect antibiotic prescribing pat-terns. Many patients believe antibiotics can cure every type of fever, cough, cold, or sore throat. They often demand antibiotics even when the illness is viral. To satisfy patients or save consultation time, some doctors prescribe antibiotics unnecessarily. Self-medication and use of leftover antibiotics are al-so common problems in many communities. These practices contribute significantly to irrational anti-biotic use and resistance. Hospital policies and healthcare systems have a strong influence on antibiotic prescribing. Hospitals with proper antibiotic stewardship programs and treatment guidelines usually show better prescribing practices. Antibiotic stewardship programs help monitor antibiotic use, encourage culture-based therapy, and reduce unnecessary prescribing. Infection control measures in hospitals also reduce the spread of resistant bacteria and lower antibiotic use. In hospitals without strict guide-lines, irrational prescribing patterns are more common.
The prevalence of antibiotic resistance in a particular area also affects prescribing behavior. In regions where resistant bacteria are common, doctors may use stronger antibiotics or combination therapy more frequently. Local resistance data help doctors choose the most effective antibiotics. However, overuse of broad-spectrum antibiotics can further increase resistance, creating a continuous cycle of antibiotic misuse. Economic factors also influence antibiotic prescribing patterns. The cost and availability of medicines affect treatment decisions, especially in developing countries. Some patients cannot afford expensive antibiotics, so doctors may prescribe cheaper alternatives. In certain situations, financial limitations may lead to incomplete treatment because patients stop taking medicines once symptoms im-prove. Pharmaceutical company promotion and marketing strategies may also influence prescribing behavior by encouraging doctors to prescribe specific branded antibiotics. Workload and time pressure in hospitals and clinics are additional factors affecting prescribing patterns. In busy healthcare settings, doctors may not have enough time for detailed patient examination, counseling, or laboratory investigations. As a result, they may prescribe broad-spectrum antibiotics quickly to reduce the risk of complications. Lack of follow-up facilities also contributes to empirical antibiotic prescribing. The route of ad-ministration is another important factor. Injectable antibiotics are commonly used in hospitalized or critically ill patients because they provide rapid action and better drug delivery. However, unnecessary use of injections increases treatment cost and risk of complications such as infections at the injection site. Oral antibiotics should be preferred whenever possible because they are safer, cheaper, and more convenient for patients. Adverse drug reactions and drug interactions also affect antibiotic selection. Some antibiotics may cause allergic reactions, kidney damage, liver toxicity, hearing loss, or gastrointestinal disturbances. Patients taking multiple medications for chronic diseases are at greater risk of interactions. Doctors must carefully review patient history before prescribing antibiotics. Public health conditions such as poor sanitation, overcrowding, lack of clean water, and poor hygiene can increase the spread of infections and antibiotic use. During outbreaks of infectious diseases, antibiotic prescribing may increase due to fear of secondary bacterial infections. In many developing countries, antibiotics are easily available without prescription, which encourages self-medication and misuse. Healthcare professionals, especially clinical pharmacists, play an important role in improving antibiotic prescribing patterns. They help doctors choose suitable antibiotics, adjust doses, monitor adverse effects, and educate patients about proper medicine use. Clinical pharmacists also support antibiotic stewardship programs and promote rational use of antibiotics.
12. DRUG INTERACTION AND ADVERSE DRUG REACTION
Antibiotics are widely used medicines for the treatment and prevention of bacterial infections. They play an important role in modern healthcare and help in reducing illness and death caused by infectious diseases. Although antibiotics are generally safe and effective when used properly, they can sometimes cause unwanted effects known as adverse drug reactions and may also interact with other medicines. These problems are more common in elderly patients, hospitalized patients, and individuals suffering from chronic diseases because they often take multiple medicines for long periods. Understanding drug interactions and adverse drug reactions of antibiotics is important for safe and effective treatment. Drug interaction occurs when the effect of one medicine is changed by another medicine, food, or chemical substance. Antibiotic drug interactions can increase or decrease the effectiveness of medicines and may also increase the risk of toxicity and side effects. Drug interactions may occur due to changes in absorption, metabolism, distribution, or elimination of medicines in the body. Some interactions are mild, while others may become serious and life-threatening.
One common example of antibiotic interaction is between macrolide antibiotics such as erythromycin and clarithromycin and cardiovascular drugs. These antibiotics inhibit liver enzymes responsible for drug metabolism and may increase the blood levels of drugs such as statins, warfarin, and calcium channel blockers. This can lead to toxicity, muscle damage, bleeding, or heart rhythm disturbances. Fluoroquinolone antibiotics such as ciprofloxacin may interact with antidiabetic medicines and cause abnormal blood sugar levels. They may also interact with antacids containing calcium, magnesium, or aluminum, reducing antibiotic absorption and effectiveness.
Tetracycline antibiotics are known to interact with milk products, iron supplements, and antacids. These substances form complexes with tetracyclines and decrease their absorption from the gastrointestinal tract. Aminoglycoside antibiotics such as gentamicin may interact with diuretics and other nephrotoxic drugs, increasing the risk of kidney damage and hearing loss. Rifampicin is another important antibiotic that interacts with many medicines because it increases liver enzyme activity and reduces the effect of oral contraceptives, anticoagulants, antiretroviral drugs, and antiepileptic medicines. Patients suffering from chronic diseases such as Diabetes Mellitus, Chronic Kidney Disease, hypertension, heart disease, and Chronic Obstructive Pulmonary Disease are at greater risk of drug interactions because they usually take multiple medicines simultaneously. In these patients, careful monitoring and dose adjustment are necessary to avoid complications and improve treatment outcomes. Adverse drug reactions are unwanted and harmful effects that occur after taking medicines at normal therapeutic doses. Antibiotics are among the most common causes of adverse drug reactions in hospitals and community healthcare settings. The severity of reactions may range from mild gastrointestinal discomfort to severe allergic reactions and organ damage.
One of the most common adverse reactions caused by antibiotics is gastrointestinal disturbance. Patients may experience nausea, vomiting, abdominal pain, diarrhea, and loss of appetite. These effects occur because antibiotics disturb the normal bacterial flora present in the intestine. Broad-spectrum antibiotics can also cause superinfections such as fungal infections and pseudomembranous colitis caused by Clostridium difficile. Allergic reactions are another important adverse effect of antibiotics. Penicillins and cephalosporins commonly cause hypersensitivity reactions such as skin rashes, itching, fever, urticaria, and anaphylaxis. Anaphylaxis is a severe life-threatening allergic reaction that requires im-mediate medical treatment. Patients with a history of allergy should be carefully evaluated before pre-scribing antibiotics.
Some antibiotics may cause kidney toxicity, known as nephrotoxicity. Aminoglycosides and vancomycin are commonly associated with kidney damage, especially when used in high doses or for long durations. Patients with chronic kidney disease are at greater risk because their renal function is already im-paired. Regular monitoring of kidney function tests is important during therapy with nephrotoxic anti-biotics. Liver toxicity or hepatotoxicity is another serious adverse effect associated with antibiotics such as rifampicin, tetracyclines, and macrolides. Symptoms may include jaundice, fatigue, abdominal pain, and abnormal liver enzyme levels. Patients with liver disease require careful monitoring and dose adjustment during antibiotic therapy. Certain antibiotics may also affect the nervous system and hear-ing. Aminoglycosides can cause ototoxicity, leading to hearing loss or balance problems. High doses of some antibiotics may produce headache, dizziness, confusion, seizures, or neuropathy, especially in elderly patients and patients with renal impairment. Hematological adverse effects may also occur with antibiotic use. Chloramphenicol can cause bone marrow suppression and aplastic anemia, while sulfonamides may produce hemolytic anemia in susceptible individuals. Long-term use of some antibiotics may reduce white blood cell count and increase infection risk.
Photosensitivity is another adverse effect seen with tetracyclines and fluoroquinolones. Patients taking these medicines may develop skin reactions after exposure to sunlight. Therefore, they are advised to avoid excessive sun exposure during treatment. The risk of adverse drug reactions and interactions in-creases in polypharmacy, where patients take multiple medicines together. Elderly patients are more vulnerable because of reduced organ function and altered drug metabolism. Hospitalized patients, critically ill patients, and immunocompromised individuals also have a higher risk of complications. Proper prescribing practices and patient monitoring are essential to prevent drug interactions and adverse reactions. Doctors should carefully evaluate patient history, allergy status, organ function, and current medications before prescribing antibiotics. Culture and sensitivity testing can help select the most appropriate antibiotic and reduce unnecessary drug exposure.
Healthcare professionals, especially clinical pharmacists, play an important role in identifying potential drug interactions and monitoring adverse drug reactions. They help in dose adjustment, patient counseling, and improving medication safety. Patients should also be educated about taking medicines correctly, reporting unusual symptoms, and avoiding self-medication.
13. WHO PRESCRIBING INDICATORS AND ROLE OF CLINICAL PHARMACIST
World Health Organization prescribing indicators are standard parameters developed to evaluate the prescribing pattern of medicines in healthcare settings. These indicators help in assessing whether med-icines are being used rationally, safely, and effectively. Irrational prescribing of medicines, especially antibiotics, is a major global health problem because it can lead to adverse drug reactions, increased healthcare costs, and antibiotic resistance. WHO prescribing indicators are widely used in hospitals, clinics, and research studies to improve the quality of healthcare services and promote rational drug use. The WHO prescribing indicators mainly focus on five important areas.
The first indicator is the average number of drugs prescribed per encounter. This indicator helps identify polypharmacy, which means prescribing too many medicines to a patient. Polypharmacy increases the risk of drug interactions, adverse effects, and poor patient compliance. Ideally, the number of medicines prescribed should be as low as possible while still providing effective treatment. The second indicator is the percentage of drugs prescribed by generic name. Generic prescribing is encouraged because generic medicines are usually cheaper, easily available, and equally effective as branded medicines. Prescribing medicines by generic name also reduces confusion and promotes rational drug use.
The third indicator is the percentage of encounters with an antibiotic prescribed. Antibiotics are among the most commonly misused medicines worldwide. Excessive and unnecessary use of antibiotics con-tributes to antibiotic resistance. This indicator helps evaluate whether antibiotics are being prescribed rationally and only when necessary.
The fourth indicator is the percentage of encounters with an injection prescribed. Injections are important in certain conditions because they provide rapid action, but unnecessary use increases treatment cost and risk of infections. Oral medicines are preferred whenever possible because they are safer, cheaper, and more convenient.
The fifth indicator is the percentage of drugs prescribed from the essential medicines list. Essential medicines are drugs selected based on safety, effectiveness, and public health importance. Prescribing from the essential medicines list ensures availability of safe and cost-effective treatment.
WHO prescribing indicators are useful for identifying irrational prescribing practices such as polypharmacy, overuse of antibiotics, unnecessary injections, and prescribing expensive branded medicines. These indicators help hospitals and healthcare professionals improve treatment quality and reduce medication-related problems. Clinical pharmacists play a very important role in promoting ration-al drug use and improving prescribing patterns. A clinical pharmacist is a healthcare professional who specializes in medication therapy management and works closely with doctors, nurses, and patients to ensure safe and effective use of medicines. Clinical pharmacists are actively involved in hospitals, clinics, and community healthcare settings. One of the major responsibilities of clinical pharmacists is re-viewing prescriptions and checking whether medicines are prescribed appropriately. They monitor drug doses, duration of therapy, and possible drug interactions. This is especially important in patients with chronic diseases such as Diabetes Mellitus, Chronic Kidney Disease, hypertension, and Chronic Obstructive Pulmonary Disease because these patients usually take multiple medications and are at greater risk of adverse effects and interactions.
Clinical pharmacists also play an important role in antibiotic stewardship programs. They help doctors choose the most appropriate antibiotic, monitor antibiotic use, and reduce unnecessary prescribing. By promoting rational antibiotic use, clinical pharmacists help control antibiotic resistance and improve patient outcomes. Another important role of clinical pharmacists is monitoring adverse drug reactions. They identify and report side effects caused by medicines and help in preventing medication-related complications. Pharmacists also educate patients about correct medicine use, proper dosage, possible side effects, and the importance of completing the full course of antibiotics.
Patient counseling is an important part of clinical pharmacy practice. Many patients do not take medicines properly due to lack of knowledge or misunderstanding. Clinical pharmacists explain how and when medicines should be taken, possible food or drug interactions, and precautions during therapy. Proper counseling improves patient adherence and treatment success. Clinical pharmacists also help in dose adjustment for patients with kidney or liver disease. Since many medicines are metabolized or excreted through these organs, improper dosing can lead to toxicity. Pharmacists ensure safe and effective dosing based on patient condition and laboratory reports. In hospitals, clinical pharmacists participate in ward rounds and discuss treatment plans with doctors and other healthcare professionals. Their involvement helps improve medication safety and reduces prescribing errors. They also contribute to drug information services by providing updated information regarding medicines, interactions, contraindications, and treatment guidelines. Clinical pharmacists play an important role in reducing healthcare costs. By promoting rational drug use, preventing adverse effects, and minimizing unnecessary medicine use, they help reduce hospital stays and treatment expenses. They also encourage generic prescribing and use of essential medicines whenever appropriate. Education and awareness programs conducted by clinical pharmacists are helpful in improving public understanding about medicines and preventing self-medication. They also support healthcare research related to drug utilization studies, prescribing patterns, and medication safety.
14. PHARMACOVIGILANCE OF ANTIBIOTICS
Pharmacovigilance is the science and activity related to the detection, assessment, understanding, and prevention of adverse effects or any other drug-related problems. It plays an important role in ensuring the safe and effective use of medicines in healthcare settings. Antibiotics are among the most frequently prescribed drugs worldwide and are widely used for the treatment and prevention of bacterial infections. Although antibiotics are highly effective medicines, their use is often associated with adverse drug reactions (ADRs), drug interactions, allergic reactions, toxicity, and antimicrobial resistance. Therefore, pharmacovigilance of antibiotics is essential for monitoring drug safety, improving patient care, and promoting rational antibiotic use. Antibiotics can produce a wide range of adverse drug reactions ranging from mild gastrointestinal disturbances to severe life-threatening conditions.( Fig. 4)
Common adverse effects include nausea, vomiting, diarrhea, skin rashes, allergic reactions, nephrotoxicity, hepatotoxicity, ototoxicity, and blood disorders. Some antibiotics may also cause superinfections due to destruction of normal microbial flora. In severe cases, hypersensitivity reactions such as anaphylaxis may occur, particularly with penicillins and cephalosporins. Continuous monitoring of these reactions through pharmacovigilance programs helps healthcare professionals identify the safety profile of antibiotics and prevent serious complications.
Patients suffering from chronic diseases are more vulnerable to antibiotic-related adverse effects be-cause they often receive multiple medications simultaneously. Polypharmacy increases the risk of drug interactions and toxicity. For example, certain antibiotics may interact with antidiabetic drugs, anticoagulants, antihypertensive medicines, or nephrotoxic agents, leading to harmful effects. Elderly patients and patients with liver or kidney impairment are at even greater risk because drug metabolism and elimination are altered. Pharmacovigilance helps detect such interactions early and ensures safer medication practices.
One of the major objectives of antibiotic pharmacovigilance is the identification and prevention of antimicrobial resistance. Irrational use of antibiotics, unnecessary prescriptions, self-medication, pro-longed therapy, and incomplete treatment courses contribute significantly to the development of resistant microorganisms. Resistant bacterial strains make infections difficult to treat and increase morbidity, mortality, and healthcare costs. Monitoring antibiotic use and adverse outcomes through pharmacovigilance systems supports antimicrobial stewardship programs and promotes rational prescribing practices. The process of pharmacovigilance involves collection, reporting, analysis, and evaluation of adverse drug reactions. Healthcare professionals such as physicians, pharmacists, nurses, and other medical staff play an important role in identifying and reporting suspected ADRs. Spontaneous reporting systems are commonly used to collect information regarding adverse effects associated with antibiotics. These reports help regulatory authorities evaluate drug safety and take necessary actions such as updating warnings, restricting use, or withdrawing unsafe medicines from the market.
In India, the Pharmacovigilance Programme of India (PvPI) has been established to monitor the safety of medicines and improve patient safety. The program encourages healthcare professionals and consumers to report adverse drug reactions. The collected data are analyzed to identify safety signals and improve drug monitoring systems. Similarly, the World Health Organization operates an international drug monitoring program that collects global ADR data to ensure medicine safety worldwide. Clinical pharmacists play a vital role in antibiotic pharmacovigilance. They monitor prescriptions, identify drug interactions, counsel patients regarding proper medication use, detect adverse drug reactions, and educate healthcare professionals about rational antibiotic therapy. Their involvement in antimicrobial stewardship programs helps reduce medication errors and improve therapeutic outcomes. Patient education is another important component of pharmacovigilance.
Figure:4 Types of Pharmacovigilance Activities
Patients should be informed about the importance of completing antibiotic courses, avoiding self-medication, following prescribed doses, and reporting any unusual symptoms or side effects immediately. Proper awareness can significantly reduce irrational antibiotic use and improve patient safety. Therefore, pharmacovigilance of antibiotics is essential for ensuring safe, effective, and rational antibiotic therapy. Continuous monitoring of adverse drug reactions, drug interactions, and resistance patterns helps healthcare professionals optimize treatment, reduce complications, and improve overall healthcare quality. Effective pharmacovigilance systems contribute significantly to patient safety and the prevention of antimicrobial resistance.
15. AIM AND OBJECTIVE OF THE STUDY
The present study aims to evaluate the utilization pattern of antibiotics in patients suffering from chronic diseases and to assess the rationality of antibiotic prescribing practices in healthcare settings. The study also aims to identify factors influencing antibiotic use, adverse drug reactions, drug interactions, and the impact of irrational antibiotic use on antimicrobial resistance. Furthermore, the study intends to promote rational antibiotic therapy and improve patient safety through proper monitoring and clinical pharmacy interventions. The primary objective of this study is to analyze the prescribing pattern and utilization of antibiotics among patients with chronic diseases such as diabetes mellitus, hypertension, chronic obstructive pulmonary disease (COPD), chronic kidney disease, cardiovascular diseases, and asthma. The study aims to identify the most commonly prescribed antibiotics and evaluate whether these drugs are being used appropriately according to standard treatment guidelines.
Another important objective of the study is to assess the rational and irrational use of antibiotics using prescribing indicators recommended by the World Health Organization. The study also focuses on identifying unnecessary antibiotic prescriptions, inappropriate dose selection, prolonged therapy, and excessive use of broad-spectrum antibiotics that may contribute to antimicrobial resistance. The study further aims to evaluate adverse drug reactions and possible drug interactions associated with antibiotic therapy in chronic disease patients who are often receiving multiple medications simultaneously. Monitoring the safety and effectiveness of antibiotic therapy is important to reduce complications and improve patient outcomes. In addition, the study intends to analyze factors affecting antibiotic prescribing patterns, including physician prescribing habits, patient expectations, disease severity, hospital policies, and availability of diagnostic facilities. The role of clinical pharmacists in promoting rational antibiotic use, patient counseling, and antimicrobial stewardship programs will also be evaluated.
Another objective of the study is to create awareness regarding appropriate antibiotic use and the dangers of self-medication, incomplete treatment courses, and antibiotic resistance. The findings of the study may help healthcare professionals and policymakers develop effective strategies for improving prescribing practices and reducing antimicrobial resistance. Overall, the study aims to promote safe, effective, and rational use of antibiotics in chronic disease patients in order to improve healthcare quality, minimize adverse effects, and enhance therapeutic outcomes.
16. MATERIAL AND METHODS
The present study was carried out to evaluate the utilization pattern of antibiotics in patients suffering from chronic diseases and to assess the rationality of antibiotic prescribing practices in healthcare set-tings. The study was designed as an observational drug utilization study and was conducted in the med-icine department of a hospital or healthcare institution.

Figure: 5 Mechanism of Action of Fluoroquinolone Antibiotics
The main purpose of the study was to analyze how antibiotics are prescribed and used in patients with chronic illnesses such as diabetes mellitus, hypertension, chronic obstructive pulmonary disease (COPD), chronic kidney disease, cardiovascular diseases, and asthma. Since chronic disease patients are more prone to infections and usually receive multiple medications, monitoring antibiotic use in these patients is important to ensure safe and effective therapy. The study included both male and fe-male patients of different age groups who were diagnosed with chronic diseases and were receiving one or more antibiotics during their treatment. Patients admitted to inpatient departments as well as those attending outpatient departments were included in the study. However, patients who were not receiving antibiotics or had incomplete medical records were excluded from the study. The study was conducted over a specific duration depending on the availability of patients and research requirements.
Data for the study were collected from various hospital sources such as patient case sheets, prescriptions, medication charts, laboratory reports, and hospital records. In some cases, patient interviews and discussions with healthcare professionals were also used to obtain additional information regarding medication history and treatment outcomes. A specially designed data collection form was prepared to record all the required information in a systematic manner. The collected data included patient demo-graphic details such as age, gender, diagnosis, and duration of illness. Information regarding prescribed antibiotics, including name of the drug, dose, dosage form, frequency of administration, route of administration, and duration of therapy, was carefully documented. Details of other medications prescribed along with antibiotics were also recorded because chronic disease patients often receive multiple drugs simultaneously. This helped in identifying possible drug interactions and polypharmacy-related problems. Special attention was given to the evaluation of rational and irrational antibiotic use. Prescriptions were analyzed using prescribing indicators recommended by the World Health Organization. Parameters such as average number of drugs prescribed per prescription, percentage of antibiotics prescribed, use of generic medicines, and adherence to essential medicine lists were assessed to determine the quality of prescribing practices. The study also focused on identifying unnecessary use of antibiotics, inappropriate dose selection, prolonged therapy, and excessive use of broad-spectrum antibiotics.
During the study, possible adverse drug reactions associated with antibiotic therapy were monitored and documented. Common adverse effects such as gastrointestinal disturbances, allergic reactions, nephrotoxicity, hepatotoxicity, and skin reactions were evaluated. Drug interactions between antibiotics and other medications used for chronic diseases were also assessed with the help of standard drug in-formation resources and reference materials. Monitoring these interactions was important because chronic disease patients are at higher risk of medication-related complications. The collected data were organized and analyzed using suitable statistical methods such as percentages, averages, tables, and graphical representations. The results obtained from the study were interpreted to understand prescribing trends, frequency of antibiotic use, common drug interactions, and the rationality of therapy. The findings helped in identifying areas where improvement in antibiotic prescribing practices was needed. Confidentiality of patient information was maintained throughout the study. Necessary permission was obtained from the hospital authorities or institutional ethics committee before conducting the research. Patient identity and personal details were kept strictly confidential and used only for academic and re-search purposes. Clinical pharmacists also played an important role during the study by reviewing prescriptions, monitoring adverse drug reactions, identifying medication-related problems, and counseling patients regarding proper antibiotic use. Their involvement helped in promoting rational drug therapy and improving patient safety. Thus, the materials and methods used in the study provided a systematic approach for evaluating antibiotic utilization patterns in chronic disease patients. The collected information helped in understanding current prescribing practices and contributed toward promoting rational antibiotic use and reducing antimicrobial resistance.
17. LIMITATION AND CHALLENGES
The present study was conducted to evaluate the utilization pattern of antibiotics in patients suffering from chronic diseases and to assess the rationality of antibiotic prescribing practices. Although the study was carried out systematically and carefully, certain limitations and challenges were encountered during the research process. These factors may have influenced the overall findings and interpretation of the study results. One of the major limitations of the study was the small sample size. The study included a limited number of patient prescriptions and case records collected during a specific period of time. Because of this limited sample, the results may not fully represent the antibiotic prescribing pat-terns of the entire population. A larger sample size and multicenter study could provide more reliable and generalized findings.
Another limitation was that the study was conducted in a single hospital or healthcare institution. Anti-biotic prescribing practices may vary among hospitals depending on physician preferences, patient conditions, hospital policies, and availability of medicines. Therefore, the findings obtained from one healthcare setting may not be applicable to all hospitals or regions. The limited duration of the study was also a challenge. Since the study was conducted for a short period, long-term prescribing trends, seasonal variations in infections, and changes in antimicrobial resistance patterns could not be fully evaluated. Longer study durations are generally more effective for understanding the overall impact of antibiotic utilization and resistance development. Incomplete patient records and insufficient documentation created additional difficulties during data collection. In some cases, information regarding diagnosis, laboratory investigations, culture sensitivity reports, previous medication history, and adverse drug reactions was missing or inadequately documented. This affected the detailed analysis of antibiotic prescribing patterns and rationality of therapy.
Another major challenge was the lack of microbiological culture and sensitivity testing in many patients. Antibiotics were often prescribed empirically without confirmation of the causative organism. Due to this, it was difficult to determine whether the selected antibiotic was fully appropriate according to bacterial sensitivity patterns. Empirical prescribing practices also limited the assessment of rational antibiotic use. Patient-related factors also affected the study. Some patients were unable to provide ac-curate medication history or information regarding previous antibiotic use. Poor patient awareness, self-medication practices, incomplete treatment courses, and non-adherence to therapy further complicated the evaluation process. In chronic disease patients, polypharmacy was common, making it difficult to identify the exact cause of adverse drug reactions or drug interactions. The identification and reporting of adverse drug reactions posed another challenge during the study. Mild or unnoticed adverse reactions may not have been reported by patients or documented in medical records. Therefore, the actual incidence of antibiotic-related adverse effects may have been underestimated. Time constraints and limited resources were additional challenges faced during the research. Limited access to advanced diagnostic tools, updated drug information resources, and electronic medical record systems restricted the depth of analysis. In some cases, heavy workload in hospital settings also made data collection more difficult.
Another limitation was that the study mainly focused on prescribing patterns and utilization of antibiotics. Economic evaluation, pharmacoeconomic analysis, and long-term clinical outcomes of antibiotic therapy were not studied in detail. Similarly, the impact of patient counseling and antimicrobial stewardship interventions could not be assessed completely during the study period. Despite these limitations and challenges, the study provided useful information regarding antibiotic prescribing practices, ration-al and irrational use of antibiotics, adverse drug reactions, and antimicrobial resistance in chronic disease patients. The findings of the study may help healthcare professionals improve rational antibiotic prescribing and encourage further research in this field. Future studies involving larger populations, multiple healthcare centers, and longer durations can provide more comprehensive and accurate results regarding antibiotic utilization and patient safety.
18.FUTURE PERSPECTIVES
The increasing use of antibiotics in chronic disease patients has created serious concerns regarding antimicrobial resistance, adverse drug reactions, and irrational prescribing practices. Therefore, future efforts should focus on promoting rational antibiotic use, improving patient safety, and strengthening healthcare systems to control the growing burden of resistant infections. Proper monitoring, research, education, and implementation of antibiotic stewardship programs are essential for improving the quality of healthcare and ensuring effective antibiotic therapy in the future. One of the most important future perspectives is the development and implementation of strong antimicrobial stewardship programs in hospitals and healthcare institutions. These programs can help ensure the appropriate selection, dose, duration, and route of antibiotic therapy. Regular monitoring of prescriptions, adherence to treatment guidelines, and restriction of unnecessary broad-spectrum antibiotic use can significantly reduce irrational prescribing practices and prevent antimicrobial resistance. Another important area for future improvement is increasing awareness among healthcare professionals and patients regarding rational anti-biotic use. Educational programs, workshops, and awareness campaigns should be conducted to educate physicians, pharmacists, nurses, and the general public about the dangers of self-medication, incomplete antibiotic courses, and overuse of antibiotics. Patient counseling regarding proper medication adherence and infection prevention can also improve therapeutic outcomes and reduce resistance development. The role of clinical pharmacists is expected to become more significant in the future management of antibiotic therapy. Clinical pharmacists can actively participate in prescription review, monitoring of adverse drug reactions, identification of drug interactions, dose adjustments, and patient counseling. Their involvement in multidisciplinary healthcare teams can help improve rational drug use and minimize medication-related complications in chronic disease patients. Future studies should focus on larger populations and multicenter research to obtain more comprehensive information regarding anti-biotic prescribing patterns and antimicrobial resistance trends. Long-term studies involving different healthcare settings can provide better understanding of regional prescribing behaviors, resistance pat-terns, and effectiveness of intervention strategies. Advanced pharmacovigilance and drug utilization studies can further improve the safety and effectiveness of antibiotic therapy. Another important future perspective is the use of advanced diagnostic techniques and microbiological investigations for accurate identification of infectious organisms. Culture sensitivity testing and rapid diagnostic methods can help physicians select the most appropriate antibiotic and reduce unnecessary empirical therapy. This approach can improve treatment outcomes and decrease the emergence of resistant microorganisms. Research and development of new antibiotics and alternative therapies are also essential to combat the growing problem of antimicrobial resistance. Since many bacteria have developed resistance to current-ly available antibiotics, pharmaceutical research organizations and healthcare authorities need to focus on discovering new antimicrobial agents, vaccines, and innovative treatment approaches. Alternative therapies such as bacteriophage therapy, immunotherapy, probiotics, and herbal medicines may also provide supportive treatment options in the future. The use of electronic prescribing systems and digital healthcare technologies can further improve antibiotic prescribing practices. Computerized prescription monitoring systems can help identify medication errors, drug interactions, duplicate therapies, and in-appropriate antibiotic use. Electronic medical records can also support better patient monitoring and data analysis for future research.
According to the World Health Organization, global collaboration among healthcare professionals, governments, regulatory authorities, and research organizations is necessary to control antimicrobial resistance. Strict regulations regarding over-the-counter sale of antibiotics and implementation of national antibiotic policies can help reduce misuse and improve public health outcomes. In developing countries like India, strengthening healthcare infrastructure, improving diagnostic facilities, and in-creasing access to quality healthcare services are important future goals.
CONCLUSION
The present study concluded that antibiotics are commonly prescribed in patients suffering from chronic diseases because these patients are more susceptible to infections due to weakened immunity and long-term health complications. The study observed that broad-spectrum antibiotics were frequently used in both inpatient and outpatient settings for the management of respiratory tract infections, urinary tract infections, skin infections, and other bacterial infections associated with chronic diseases such as Diabetes Mellitus, Chronic Kidney Disease, cardiovascular diseases, and Chronic Obstructive Pulmonary Disease. The findings of the study showed that although antibiotics play an important role in infection control and improving patient outcomes, irrational prescribing practices are still common in healthcare settings. Empirical prescribing, polypharmacy, unnecessary use of broad-spectrum antibiotics, and lack of culture sensitivity testing were observed in many cases. These practices increase the risk of adverse drug reactions, drug interactions, treatment failure, and antibiotic resistance. The study also highlighted that antibiotic resistance has become a major public health concern due to the misuse and overuse of antibiotics. Incomplete treatment courses, self-medication, and inappropriate prescribing further contribute to the development of resistant bacterial strains. Therefore, rational antibiotic use is very important to preserve the effectiveness of antibiotics and improve patient safety. The role of the World Health Organisation prescribing indicators was found useful in evaluating prescribing patterns and identifying irrational drug use. The involvement of clinical pharmacists was also beneficial in promoting rational antibiotic use, monitoring adverse drug reactions, preventing drug interactions, and educating patients regarding proper medication use.
REFERENCES

Pankaj Kumar, Parveen Kumar, Comprehensive Study of Drug Utilization Study of Antibiotics in Chronic Disease, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 2178-2214. https://doi.org/10.5281/zenodo.20608124
 10.5281/zenodo.20608124
10.5281/zenodo.20608124