
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Bharat School of Pharmacy, Mangalpally, Ibrahimpatnam, 501510
Breast cancer is one of the most common malignancies worldwide, characterised by the uncontrolled proliferation of breast tissue cells and significant health burden among women. This review outlines the aetiology, risk factors, pathophysiology, clinical features, diagnosis, staging, and treatment approaches of breast cancer. Special focus is given to chemotherapy - induced neutropenia (CIN), a major dose - limiting toxicity associated with cytotoxic chemotherapy that increases susceptibility to infections and affects treatment continuity. Paclitaxel, a widely used antineoplastic agent, plays a key role in breast cancer management due to its ability to inhibit microtubule depolymerisation and induce cell cycle arrest. However, its use is commonly associated with haematological toxicities, particularly neutropenia. This study includes five clinical case reports to evaluate the incidence and severity of neutropenia in patients undergoing weekly and three - weekly paclitaxel chemotherapy regimens. The findings suggest that neutropenia occurs in both treatment schedules, with increased severity observed in patients receiving 3- weekly regimens compared to weekly dosing. Regular monitoring of absolute neutrophil count is essential for early detection and effective management of CIN, thereby improving patient safety and therapeutic outcomes.
The unchecked proliferation of aberrant cells in the breast's milk-producing glands or in the ducts that carry milk to the nipples is the hallmark of breast cancer, a relatively prevalent form of cancer in women. It is a malignant tumour that begins in both male and female breast tissue. The male has breast tissue, which is made up of fat, fibrous fibers, fine channels, and glandular elements or lobules, just like the female. Most breast cancers start in the ducts (ductal carcinoma). A tiny percentage (lobular cancers) begin in the sacs or lobules. There are various subtypes of breast cancer within these two categories. While some grow quickly, others grow very slowly. Breast cancer can spread to the liver, bones, lymph nodes, and other areas of the body. Usually, breast cancer is found either during a screening test, prior to the onset of symptoms, or after a woman feels a lump (1).
Symptoms:
There are some of the main symptoms that may be seen during
breast cancer are-
Risk Factors :
Breast cancer is one of the many and common malignant tumors that harm women. Numerous internal and external variables contribute to the development and occurrence of breast cancer.
Table 1 lists the risk factors.
|
Risk Factors of Breast Cancer |
|
|
Hormonal and reproductive |
|
|
Related to physiological factors and health status |
|
|
Nutritional |
|
|
Other lifestyle-related |
|
Epidemiology:
The very young (younger than 35) and the very old (more than 75) have the highest mortality rates.4 The very young seem to have more aggressive illness, while the very old may not receive aggressive treatment or may have concomitant conditions that raise the death rate from breast cancer (3).
Breast cancer is the most commonly diagnosed cancer worldwide, with 2.3 million new cases and 685,000 deaths reported in 2020. Its incidence is increasing due to aging populations and improved screening. Male breast cancer is rare, accounting for about 1% of cases (4).
Stages :
The TNM classification system, which takes into account tumor size, regional lymph node involvement, and the existence of distant metastases, provides the foundation for breast cancer staging (3).
The stages of breast cancer ranges from 0-IV.
1) Stage 0: This breast cancer means that breast cancer cells have developed, but they
cannot spread to any other surrounding tissues, or to the lymph nodes or other organs.
2) Stage I: The first stage of breast cancer means that tumor size is less than 2 cm. The I
stage is divided into two Stage IA & Stage IB.
3) Stage II: Stage II is divided into subcategories known as IIA and IIB.
4) Stage III: Stage III is divided into subcategories known as IIIA, IIIB, and IIIC.
5) Stage IV: It is described as invasive breast cancer that has spread beyond the breast and nearby lymph nodes to other organs of the body, such as the lungs, distant lymph nodes, skin, bones, liver, or brain (1).
Diagnosis :
A combination of clinical evaluation, imaging, and histological confirmation are used to diagnose breast cancer. Tumor type, histologic grade, lymphovascular invasion, and examination of estrogen receptor, progesterone receptor, and HER2/neu status are all part of pathologic evaluation, which has consequences for both diagnosis and treatment (3).
In addition to guiding biopsies of radiologic lesions, mammography uses low-dose x-rays to assess potential abnormalities discovered during a clinical examination or screening.
In addition to guiding biopsies and differentiating solid from cystic breast tumors, ultrasound can be utilized for staging, such as evaluating potential liver metastases in advanced disease..
The majority of procedures are performed as outpatient procedures; imaging guidance (ultrasound or mammography) aids in the localization of non-palpable lesions; biopsies remove cells or tissue for pathological investigation, determining the existence and type of cancer.
Compared to FNA, core needle biopsy allows for more precise histologic and receptor assessment by using a hollow needle, often with vacuum help, to remove bigger tissue cores from problematic locations.
The number of nodes implicated is crucial for staging and prognosis, and lymph node biopsy assesses dissemination throughout the lymphatic system, particularly to axillary nodes.
Fine needle aspiration, which is minimally invasive and helpful for differentiating cysts from solid tumors and screening for cancer, uses a thin needle to extract cells or fluid from a lump. However, it cannot accurately distinguish in situ from invasive disease, so additional core or surgical biopsy may be necessary (2).
Treatment :
Breast cancer treatment is multidisciplinary and customized according to patient characteristics, tumor biology, and stage. In order to achieve locoregional control and lower the risk of distant recurrence, therapy usually entails a combination of systemic and local medicines. Early-stage and advanced-stage malignancies, as well as noninvasive and invasive diseases, have quite different treatment approaches (3).
1. HR+/ERBB2− subtype
The primary systemic treatment for hormone-receptor-positive breast cancer is endocrine therapy. Aromatase inhibitors reduce the risk of long-term recurrence slightly more than tamoxifen, and taking tamoxifen for five years can cut the possibility of the cancer returning in half.
2. Chemotherapy in ERBB2− subtypes
Chemotherapy reduces 10-year breast cacner mortality, especially in high-risk tumors. Common regimens include AC, docetaxel/cyclophosphamide, CMF, and anthracycline-taxane combinations.
3. Triple‑negative subtype
Chemotherapy is the standard treatment for most triple-negative tumors. Carboplatin improves pathologic complete response rates, while adjuvant capecitabine benefits patients with residual disease after neoadjuvant therapy..
4. ERBB2+ subtype
Trastuzumab with chemotherapy significantly improves survival in ERBB2+ breast cancer. Additional agents like pertuzumab or neratinib provide small benefits in selected high-risk patients.
B. Local Therapy for Nonmetastatic Breast Cancer
1. Surgery
2. Radiation therapy
C. Systemic Therapy for Metastatic Breast Cancer
Metastatic Breast cancer causes most breast cancer deaths. HR+/ERBB2- disease is treated mainly with endocrine therapy plus CDK4/6 inhibitors. ERBB2+ disease uses trastuzumab-based targeted therapy, while triple-negative disease is treated with chemotherapy, PARP inhibitors for BRCA mutations and immunotherapy for PD-L1-Positive cases (5). Discussed a detail note in table 2.
Table 2. Systemic Therapy for Metastatic Breast Cancer
|
|
Hormone Receptor (HR) +/ERBB2− |
ERBB2+ (HR+ or HR−) |
Triple-Negative |
|
Typical systemic therapies for nonmetastatic disease (agents, route, And duration) |
• Endocrine therapy (all patients):
• Chemotherapy (some patients):
|
• Chemotherapy plus ERBB2-targeted therapy (all patients):
• Docetaxel/ carboplatin/ trastuzumab ±pertuzumab (TCH±P) • Intravenous therapy • 12-20 wk of chemotherapy; 1y of ERBB2-targeted therapy • Endocrine therapy (if also Hormone receptor positive) • Tamoxifen, letrozole, anastrozole, orexemestane • Oral therapy • 5-10y |
• Chemotherapy (all patients):
|
CHEMOTHERAPY INDUCED NEUTROPENIA (CIN) :
An abnormally low neutrophil count, a vital type of white blood cell that is essential in the fight against infections, is the hallmark of neutropenia. Because their body's defenses against bacteria and other pathogens are compromised, people with neutropenia are therefore more vulnerable to infections.
Cytotoxic chemotherapy weakens the body's defenses by impairing the bone marrow's capacity to make blood cells. This results in chemotherapy-induced neutropenia (CIN), a disease that makes patients extremely vulnerable to potentially fatal infections and fever (6).
An absolute neutrophil count (ANC) of less than 2000 cells/mm³ in peripheral blood is commonly used to diagnose chemotherapy-induced neutropenia (CIN).
This grading system classifies neutropenia into four levels based on absolute neutrophil count (ANC):
- Grade 1: ANC between 1500-2000 cells/mm³
- Grade 2: ANC between 1000-1500 cells/mm³
- Grade 3: ANC between 500-1000 cells/mm³
- Grade 4: ANC below 500 cells/mm³ (7).
DIAGNOSIS
A conventional complete blood count (CBC) is used to diagnose most cases of neutropenia; the corresponding differential count shows a decline in the total number of neutrophils.An absolute neutrophil count (ANC) of less than 1,500 cells/mm3 is considered mild neutropenia.Less than 1,000 cells/mm3 is regarded as a low count.Less than 500 cells/mm3 is considered severe neutropenia.
Patients may or may not show symptoms of low ANC or neutropenia. Clinical signs including bruises and decreased stamina are more likely when neutropenia is combined with thrombocytopenia and anemia, and the ANC anomaly is an unintentional discovery. Individuals who have solitary neutropenia might not have any noticeable signs. A fever may be the first indication (8).
The absolute neutrophil count is calculated by using -
ANC = (WBC count) x (% segmented neutrophils + % bands) / 100
Drugs in Study
PACLITAXEL
CATEGORY : Anti neoplastic agent, Mitotic inhibitor
Paclitaxel is a crystalline powder that is white to off-white in color. Its empirical formula is C47H51NO14, and its molecular weight is 853.9 units. Because of its high lipophilicity, it is very insoluble in water. At 216 and 217°C, itmelts (9).
STRUCTURE :
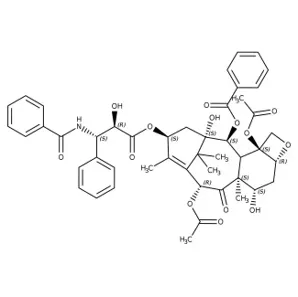
MECHANISM OF ACTION :
By attaching itself to the β-tubulin subunit of microtubules and encouraging and sustaining their polymerization, paclitaxel prevents microtubule depolymerization. This hyperstabilization prevents the normal dynamic remodeling of the microtubule network required for the formation of mitotic spindles during cell division, leading to apoptosis and arrest during the G2/M phase (10).
Indications :
Pharmacokinetics :
Adverse Effects :
Dose :
CASE DISCUSSION :
A patient of 71 years old female, has admitted in the oncology department on 10/12/2025 with the chief complaints of weight loss, change in shape of breast and redness on breast skin since 2 weeks.
Upon biopsy and clinical breast examination, it is diagnosed as Breast cancer stage IIA. Now came for treatment. All the laboratory investigations are correlated clinically and planed for weekly chemotherapy. Upon examination the patient is conscious and coherent, pulse rate - 92bpm, BP - 130/70mmHg, Temp - 97.4F, SpO2 - 98%ra, RR- 18/min.
On 10/12/2025 :
Week 1 Chemotherapy - on Paclitaxel : 70 mg / IV in 1 unit NS over 1 hr
IHC results shows invasive breast carcinoma, right breast with ER - 90%, PR - 10% & HER 2 neu-1+ .
HPE shows
Based on examination the patient was diagnosed with breast cancer stage IIA, cycle 1 was started with premedications of Inj. Palnox 0.25 mg + Inj. Dexa 8mg in 100ml NS over 15 min & Inj.Avil 1 amp + Inj. Rantac 50mg in 100ml NS over 15 min. Following which chemotherapy was started started with Inj. Paclitaxel 70 mg in 1 unit NS for 2 hrs.
Patient and their attenders are advised for the laboratory investigations of CBP including WBC, Neutrophils results must be bought every week.
On 17/12/2025 : Week 2 Chemotherapy on Paclitaxel - 70mg / IV
On 23/12/2025 : Week 3 Chemotherapy on Paclitaxel - 70mg / IV
Laboratory investigations found in the normal range for all the above cycles.
On 31/12/2025 : Week 4 Chemotherapy on Paclitaxel - 70mg / IV
The investigations found abnormal parameters like WBC - 1.2 cells/cumm, Neutrophils - 76.7%, ANC - 0.958 Thousand / mm3. These were the abnormal parameters identified in this patient. The neutropenia stage was found to be Moderate.
A patient of 55 years old female, has admitted in the oncology department on 02/01/2026 with the chief complaints of painless lump in the breast and under arms, unusual nipple discharge since 3 weeks.
Upon biopsy, mammography and clinical breast examination, it is diagnosed as Breast cancer stage III. Now came for treatment. All the laboratory investigations are correlated clinically and planed for weekly chemotherapy. Upon examination the patient is conscious and coherent, pulse rate - 96bpm, BP - 130/90mmHg, Temp - 96.8F, SpO2 - 98%ra, RR- 22/min.
On 02/01/2025 :
Week 1 Chemotherapy - on Paclitaxel : 90 mg / IV in 1 unit NS over 1 hr
IHC results shows invasive breast carcinoma, right breast with ER - 90%, PR - 50% & HER 2 neu- negative .
Based on examination the patient was diagnosed with breast cancer stage III, cycle 1 was started with premedications of Inj. Palnox 0.25 mg + Inj. Dexa 8mg + Inj.Pan 40 mg and Inj. Avil 1 AMP was given. Following which chemotherapy was started started with Inj. Paclitaxel 90 mg in 1 unit NS for 2 hrs.
Patient and their attenders are advised for the laboratory investigations of CBP including WBC, Neutrophils results must be bought every week.
On 09/01/2025 : Week 2 Chemotherapy on Paclitaxel - 90mg / IV
Laboratory investigations found in the normal range for all the above cycles.
On 16/01/2025 : Week 3 Chemotherapy on Paclitaxel - 90mg / IV
The investigations found abnormal parameters like WBC - 0.05 cells/cumm, Neutrophils - 49.7%, ANC - 0.024 Thousand / mm3. These were the abnormal parameters identified in this patient. The neutropenia stage was found to be Severe.
A patient of 52 years old female, has admitted in the oncology department on 14/02/2026 with the chief complaints of localised breast pain,Lump in left breast unusual nipple discharge since 2 years.
Upon biopsy, ultrasound and clinical breast examination, it is diagnosed as Breast cancer stage IIIc. Now came for treatment. All the laboratory investigations are correlated clinically and planed for 3- weekly chemotherapy. Upon examination the patient is conscious and coherent, pulse rate - 112bpm, BP - 100/60mmHg, Temp - 98.4F, SpO2 - 98%ra.
On 14/02/2026 :
Cycle 1 Chemotherapy AC regimen - on Paclitaxel : 260 mg / IV in 500 ml NS over 3 hrs.
IHC results shows invasive breast carcinoma, right breast with ER - 90%, PR - 90% & HER 2 neu- negative (+1) .
Ultra sound scan of both breast shows bilateral bilateral fibroadnomas.
Based on examination the patient was diagnosed with breast cancer stage III, cycle 1 was started with premedications of Inj. Dexa 12mg + Inj.Rantac 50 mg and Inj. Avil 1 AMP was given. Following which chemotherapy was started started with Inj. Paclitaxel 260 mg in 500 ml NS for 3 hrs.
Patient and their attenders are advised for the laboratory investigations of CBP including WBC, Neutrophils results must be bought every week.
Laboratory investigations found in the normal range in the above cycle.
On 07/03/2026 : Cycle 2 Chemotherapy AC regimen on Paclitaxel - 260mg / IV
The investigations found abnormal parameters like WBC - 0.31 cells/cumm, Neutrophils - 72.3%, ANC - 0.234 Thousand / mm3. These were the abnormal parameters identified in this patient. The neutropenia stage was found to be Severe.
A patient of 41 years old female, has admitted in the oncology department on 10/11/2025 with the chief complaints of weight loss, change in nipple, lump on right breast and redness on breast skin since 6 weeks.
Upon biopsy, ultra sound, mammography and clinical breast examination, it is diagnosed as Invasive right Breast cancer. Now came for treatment. All the laboratory investigations are correlated clinically and planed for 3-weekly 4 cycles of Adjuvant chemotherapy. Upon examination the patient is conscious and coherent, pulse rate - 98 bpm, BP - 130/70mmHg, Temp - 97.4F, SpO2 - 98%ra, RR- 18/min.
On 10/11/2025 :
Cycle 1 Chemotherapy AC- on Paclitaxel : 260 mg / IV in 1 unit NS over 3 hrs
Digital mammography shows defined soft tissue mass lesion noted in right breast lateral quadrant with peripheral spiculations. BIRADS IV C
Ultrasound breast shows malignant lesion in right breast with suspicious right axillary nodal metastasis.
IHC results shows invasive breast carcinoma, right breast with ER - Negative, PR - 80% & HER 2 neu-0 .
HPE shows features suggestive of invasive breast carcinoma , NST, NMBR grade II with nodal metastasis.
Based on examination the patient was diagnosed with invasive right breast cancer, cycle 1 was started with premedications of Inj. Palnox 0.25 mg + Inj. Dexa 8mg in 100ml NS over 15 min & Inj.Avil 1 amp + Inj. Rantac 50mg in 100ml NS over 15 min. Following which chemotherapy was started started with Inj. Paclitaxel 260 mg in 1 unit NS for 3 hrs.
Patient and their attenders are advised for the laboratory investigations of CBP including WBC, Neutrophils results must be bought every week.
On 01/12/2025 : Week 2 Chemotherapy on Paclitaxel - 260mg / IV
On 22/12/2025 : Week 3 Chemotherapy on Paclitaxel - 260mg / IV
Laboratory investigations found in the normal range for all the above cycles.
On 12/01/2026 : Week 4 Chemotherapy on Paclitaxel - 260mg / IV
The investigations found abnormal parameters like WBC - 0.62 cells/cumm, Neutrophils - 40.1%, ANC - 0.25 Thousand / mm3. These were the abnormal parameters identified in this patient. The neutropenia stage was found to be severe.
A patient of 56 years old female, has admitted in the oncology department on 14/01/2026 with the chief complaints of weight loss, change in shape of breast, lump on breast skin and under arms and redness on breast skin since 2 weeks.
Upon biopsy, ultra sound and clinical breast examination, it is diagnosed as Left Breast cancer. Now came for treatment. All the laboratory investigations are correlated clinically and planed for 3-weekly chemotherapy. Upon examination the patient is conscious and coherent, pulse rate - 92bpm, BP - 130/70mmHg, Temp - 97.4F, SpO2 - 98%ra, RR- 18/min.
On 14/01/2026 :
Week 1 Chemotherapy - on Paclitaxel : 290 mg / IV in 1 unit NS over 3 hrs
Upon Mammography & Ultrasound screening BIRADS - IVB Lesion noted in left outer , upper quadrant.
Based on examination the patient was diagnosed with left breast cancer, cycle 1 was started with premedications of Inj. Palnox 0.25 mg + Inj. Dexa 8mg in 100ml NS over 15 min & Inj.Avil 1 amp + Inj. Rantac 50mg in 100ml NS over 15 min. Following which chemotherapy was started started with Inj. Paclitaxel 290 mg in 1 unit NS for 3 hrs.
Patient and their attenders are advised for the laboratory investigations of CBP including WBC, Neutrophils results must be bought every week.
On 04/02/2026 : Week 2 Chemotherapy on Paclitaxel - 290mg / IV
Laboratory investigations found in the normal range for all the above cycles.
On 23/12/2025 : Week 3 Chemotherapy on Paclitaxel - 290mg / IV
The investigations found abnormal parameters like WBC - 2.16 cells/cumm, Neutrophils - 68.4%, ANC - 1.411 Thousand / mm3. These were the abnormal parameters identified in this patient. The neutropenia stage was found to be Mild.
CONCLUSION :
Paclitaxel remains a key chemotherapeutic agent in the management of breast cancer, widely used in both weekly (80-90 mg/m2) and 3-weekly (175-290 mg/m2) regimens due to its effective antimitotic activity. Across the five case studies, weekly paclitaxel demonstrated better tolerability during the initial cycles, with delayed onset and comparatively lower severity of haematological toxicity.
However, chemotherapy-induced neutropenia (CIN) was observed in both dosing schedules, with a clear difference in severity. Weekly regimens were associated with mild to moderate neutropenia, whereas 3-weekly regimens resulted in more severe neutropenia (Grade 3-4), likely due to higher single-dose exposure and non-linear pharmacokinetics of paclitaxel. The onset of neutropenia was also earlier and more pronounced in patients receiving 3-weekly dosing.
These findings highlight that dose intensity and scheduling play a crucial role in haematological toxicity. Regular monitoring of complete blood counts and absolute neutrophil count (ANC) is essential for early detection and management of neutropenia. Timely intervention through dose modification, treatment delay, or supportive care can help prevent complications such as infections and ensure continuity of chemotherapy, thereby improving patient outcomes.
Case-wise Summary :
Overall, the study demonstrates that 3-weekly paclitaxel regimens are associated with greater severity of neutropenia compared to weekly schedules, emphasizing the importance of individualized treatment planning and vigilant hematological monitoring to balance efficacy and safety.
ACKNOWLEDGEMENTS:
I would like to extend my thanks to Bharat School of Pharmacy for providing facilities to carry out this project.
REFERENCES

Dornala Manoj, Jarupla Mahika, Nermetla Mahesh, Oddi Sahithi, Mogilicharla Archana, Dr. Swathi Boddupally, Evaluation of Neutropenia in Breast Cancer Patients Receiving Weekly and 3-Weekly Paclitaxel Therapy: A Case Study, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 3062-3074. https://doi.org/10.5281/zenodo.20652249
 10.5281/zenodo.20652249
10.5281/zenodo.20652249