
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
DJPS College of Pharmacy, Pathri, Parbhani
The present study was aimed at the formulation and evaluation of sustained release matrix tablets of Apremilast using hydrophilic polymers to improve therapeutic efficacy and patient compliance. Apremilast is a phosphodiesterase-4 (PDE4) inhibitor used in the treatment of psoriasis and psoriatic arthritis, but its short half-life requires frequent administration. To overcome this limitation, sustained release matrix tablets were prepared by the direct compression method using polymers such as HPMC K4M and HPMC K15M. Preformulation studies including organoleptic properties, solubility study, melting point determination, UV spectrophotometric analysis, and drug–excipient compatibility studies were performed. The prepared formulations were evaluated for pre-compression and post-compression parameters such as angle of repose, bulk density, hardness, friability, drug content, and in vitro dissolution studies. All formulations showed satisfactory pharmaceutical properties within acceptable limits. Dissolution studies demonstrated that polymer concentration significantly affected drug release behavior. Among all formulations, batch F5 showed optimized sustained drug release up to 12 hours with acceptable hardness, friability, and drug content. Drug release kinetics followed Higuchi and Korsmeyer–Peppas models, indicating diffusion-controlled release. Stability studies conducted according to ICH guidelines confirmed the stability of the optimized formulation under accelerated conditions. The study concluded that sustained release matrix tablets of Apremilast can be successfully developed using hydrophilic polymers for prolonged drug delivery.
Introduction to Psoriasis
Psoriasis is a chronic, immune-mediated inflammatory skin disorder characterized by abnormal proliferation and differentiation of keratinocytes, leading to the formation of thick, erythematous, and scaly plaques on the skin. It is a multifactorial disease influenced by genetic, immunological, and environmental factors. The disease commonly affects the scalp, elbows, knees, lower back, and nails, and in severe conditions it may also involve joints, resulting in psoriatic arthritis. Psoriasis affects approximately 2–3% of the global population and significantly impacts the physical, psychological, and social well-being of patients [1].
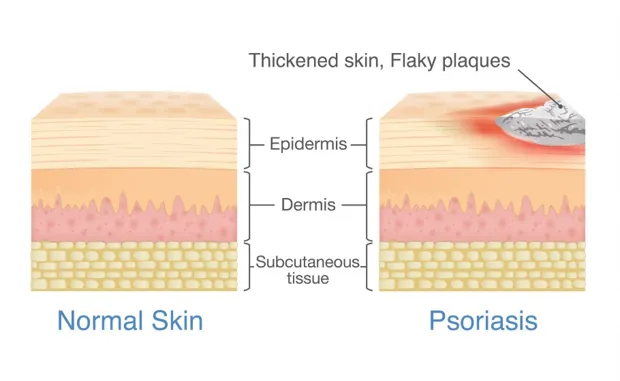
Figure 1: Comparison between normal skin and psoriatic skin
The exact pathogenesis of psoriasis is complex and involves dysregulation of the immune system. Activated T-lymphocytes release inflammatory cytokines such as Tumor Necrosis Factor-alpha (TNF-α), Interleukin-17 (IL-17), and Interleukin-23 (IL-23), which stimulate rapid multiplication of skin cells. This accelerated cell turnover results in accumulation of immature keratinocytes on the skin surface, producing characteristic psoriatic lesions.
Apremilast and Its Therapeutic Importance
Among the modern therapeutic agents used in psoriasis treatment, Apremilast has gained considerable attention due to its targeted mechanism of action and favorable safety profile. Apremilast is an orally active selective phosphodiesterase-4 (PDE4) inhibitor that regulates intracellular cyclic adenosine monophosphate (cAMP) levels and suppresses inflammatory mediators responsible for psoriasis progression [3].
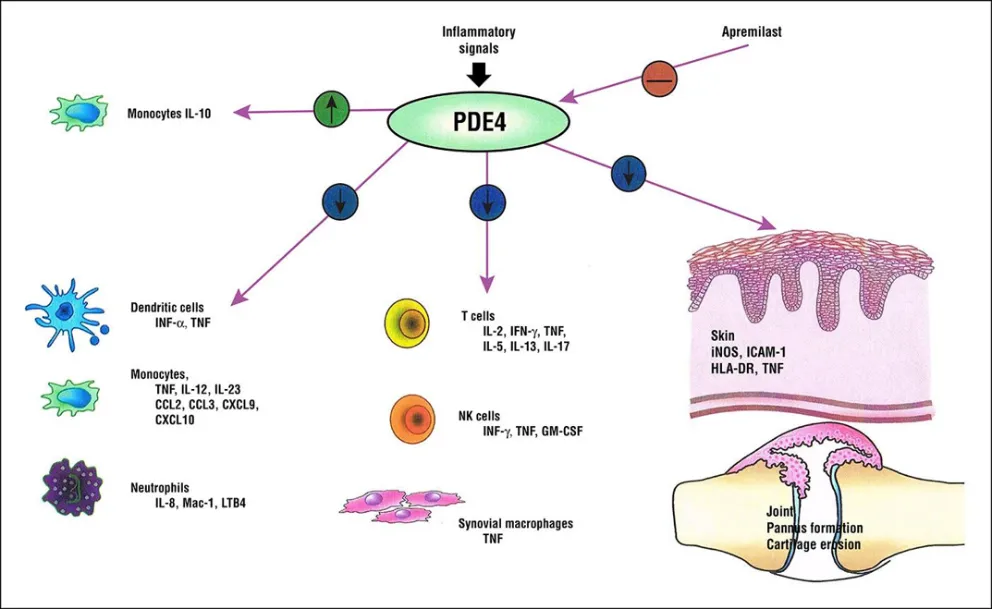
Figure 2: Mechanism of Action of Apremilas
By inhibiting PDE4 enzyme activity, Apremilast decreases the production of pro-inflammatory cytokines such as TNF-α, IL-17, IL-23, and interferon-gamma while increasing anti-inflammatory cytokines like IL-10. Due to this mechanism, Apremilast effectively reduces inflammation and improves clinical symptoms in patients with moderate to severe plaque psoriasis and psoriatic arthritis [4].
Despite its therapeutic advantages, Apremilast possesses certain limitations such as:
These limitations necessitate the development of a sustained release dosage form capable of maintaining prolonged therapeutic drug levels and reducing dosing frequency [5].
Sustained Release Drug Delivery System
Sustained release (SR) drug delivery systems are designed to release the drug slowly and continuously over an extended period of time, thereby maintaining constant plasma drug concentration within the therapeutic range. These systems improve therapeutic efficacy, minimize side effects, reduce dosing frequency, and enhance patient compliance [6].
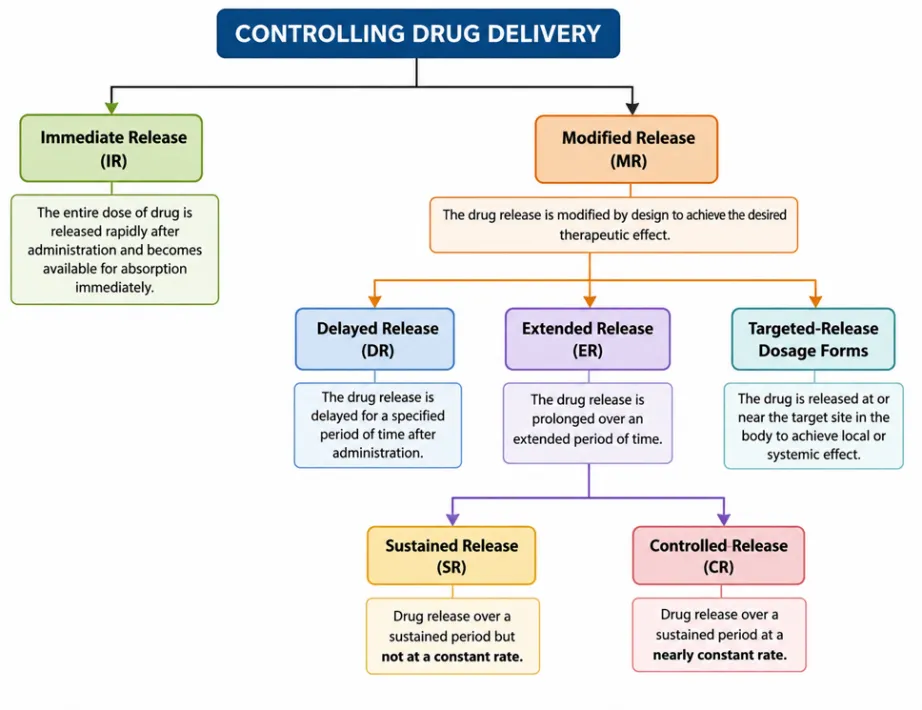
Figure 3: Classification of Controlled and Modified Drug Delivery Systems
Among various controlled release approaches, matrix tablet systems are widely preferred because of:
In matrix tablets, the drug is dispersed uniformly within a polymer matrix. Upon contact with gastrointestinal fluids, the polymer hydrates and forms a gel barrier around the tablet. Drug release occurs through diffusion, swelling, and erosion mechanisms [8].
Role of Polymers in Sustained Release Formulation
Polymers play a crucial role in controlling the release behavior of drugs from sustained release systems. Hydrophilic polymers such as Hydroxypropyl Methylcellulose (HPMC) swell upon hydration and form a viscous gel layer that regulates drug diffusion. Hydrophobic polymers such as Ethyl Cellulose retard penetration of dissolution media and prolong drug release [9].
The present study utilizes polymers such as:
These polymers were selected based on their swelling behavior, gel-forming capacity, viscosity, and ability to sustain drug release over an extended duration [10].
Need for the Present Study
Although Apremilast is clinically effective in psoriasis management, frequent administration decreases patient adherence and may produce fluctuations in therapeutic response. Development of sustained release matrix tablets can overcome these limitations by:
Therefore, the present investigation focuses on the formulation and evaluation of sustained release matrix tablets of Apremilast using different polymer combinations.
Goals of the Research
The major goals of the present research work are:
Research Objectives
The development of sustained release matrix tablets of Apremilast represents an important approach for improving therapeutic effectiveness and patient adherence in the management of psoriasis. By employing suitable hydrophilic and hydrophobic polymers, controlled drug release can be achieved effectively. The present study aims to formulate and evaluate an optimized sustained release matrix tablet capable of providing prolonged drug release with acceptable pharmaceutical characteristics [12].

Figure 4: Classification of Controlled and Modified Drug Delivery Systems
MATERIALS AND METHODS
Materials
Apremilast was obtained as a gift sample and used as the active pharmaceutical ingredient (API) for the preparation of sustained release matrix tablets. Hydroxypropyl methylcellulose polymers such as HPMC K4M and HPMC K15M were used as release-retarding agents. Microcrystalline cellulose (MCC) and lactose were used as diluents, while magnesium stearate and talc were used as lubricant and glidant respectively. All chemicals and reagents used in the study were of analytical grade.
Methods
Preformulation Studies
Preformulation studies of Apremilast were carried out to evaluate its physicochemical properties and compatibility with excipients. The following studies were performed:
Formulation of Sustained Release Matrix Tablets
Sustained release matrix tablets of Apremilast were prepared by the direct compression method. Accurately weighed quantities of drug, polymers, and excipients were passed through sieve no. 60 and blended uniformly. Magnesium stearate and talc were added at the final stage as lubricant and glidant. The prepared blend was compressed into tablets using a rotary tablet compression machine.
Evaluation of Powder Blend
The prepared powder blends were evaluated for pre-compression parameters including:
Evaluation of Tablets
The compressed tablets were evaluated for post-compression parameters such as:
In-vitro Dissolution Study
In-vitro drug release studies were carried out using USP Type II dissolution apparatus (paddle method). The dissolution medium consisted of 900 mL phosphate buffer pH 6.8 maintained at 37 ± 0.5°C with a paddle speed of 50 rpm. Samples were withdrawn at predetermined intervals up to 12 hours and analyzed spectrophotometrically at 268 nm.
Stability Studies
The optimized formulation was subjected to accelerated stability studies according to ICH guidelines at 40°C ± 2°C and 75% ± 5% RH for a period of three months. Samples were evaluated periodically for physical appearance, hardness, friability, drug content, and dissolution profile.
RESULTS & DISCUSSIONS
The present study was aimed at the formulation and evaluation of sustained release matrix tablets of Apremilast using different polymers. The results obtained from preformulation studies, formulation development, evaluation parameters, dissolution studies, kinetic modeling, and stability studies are discussed in detail.
Preformulation Studies
Preformulation studies were carried out to evaluate the physicochemical properties of Apremilast and its suitability for sustained release matrix tablet formulation.
Organoleptic Properties
The organoleptic properties of Apremilast were examined visually for color, odor, and appearance.
Table1: Organoleptic Properties of Apremilast
|
Parameter |
Observation |
|
Color |
White to pale yellow |
|
Odor |
Odorless |
|
Appearance |
Crystalline powder |
The drug appeared as a white to pale yellow crystalline powder with no characteristic odor. These observations complied with the standard characteristics reported for Apremilast, indicating purity and suitability for formulation development.
Solubility Study
Table 2: Solubility Study
|
Solvent |
Solubility |
|
Water |
Slightly soluble |
|
Methanol |
Soluble |
|
Ethanol |
Freely soluble |
|
pH 6.8 Buffer |
Moderately soluble |
The poor aqueous solubility suggests that dissolution may be a limiting step in drug absorption. However, moderate solubility in intestinal pH indicates that drug release can be effectively controlled in the gastrointestinal tract.
This supports the development of a sustained release system, where controlled dissolution enhances therapeutic effectiveness.
Melting Point
The melting point was found to be 156–158°C.
The observed melting point is within the reported range, confirming the purity and identity of the drug.
λmax Determination
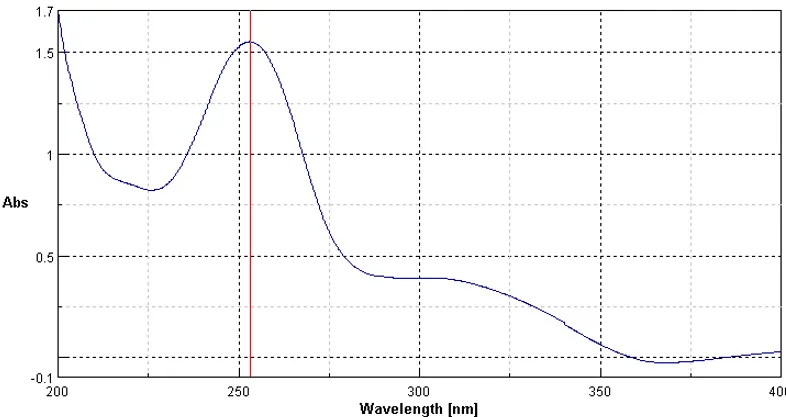
Figure 5: λmax Determination
Apremilast showed maximum absorbance at 268 nm. This wavelength was selected for further analytical studies including drug content estimation and dissolution analysis. The sharp peak confirmed good absorbance behavior and analytical suitability.
Drug–Excipient Compatibility Study
FTIR studies were performed to evaluate compatibility between Apremilast and excipients.
Table 3: FTIR Compatibility Study
|
Functional Group |
Pure Drug Peak (cm⁻¹) |
Drug-Excipient Mixture (cm⁻¹) |
|
C=O Stretching |
1760 |
1758 |
|
N-H Stretching |
3360 |
3358 |
|
S=O Stretching |
1145 |
1143 |
No significant shifting or disappearance of characteristic peaks was observed in drug-excipient mixtures. This confirmed compatibility between Apremilast and selected polymers/ excipients.
Evaluation of Tablets
Post-Compression Evaluation
Table 4: Post-Compression Evaluation
|
Formulation |
Hardness (kg/cm²) |
Friability (%) |
Drug Content (%) |
|
F1 |
5.2 |
0.6 |
98 |
|
F2 |
5.5 |
0.5 |
99 |
|
F3 |
5.8 |
0.5 |
99 |
|
F4 |
5.3 |
0.6 |
98 |
|
F5 |
5.6 |
0.5 |
99 |
|
F6 |
5.9 |
0.5 |
99 |
The hardness values ranged from 5.2–5.9 kg/cm², indicating sufficient mechanical strength of tablets. Friability values were below 1%, demonstrating good resistance to abrasion during handling. Drug content ranged from 98–99%, confirming uniform drug distribution within the formulations.
In-Vitro Dissolution Study
The dissolution study was carried out using USP Type II dissolution apparatus in phosphate buffer pH 6.8.
Table 5: In-Vitro Drug Release Data of Formulations F1–F6
|
Formulation |
Hardness (kg/cm²) |
Friability (%) |
Drug Content (%) |
|
F1 |
5.2 |
0.6 |
98 |
|
F2 |
5.5 |
0.5 |
99 |
|
F3 |
5.8 |
0.5 |
99 |
|
F4 |
5.3 |
0.6 |
98 |
|
F5 |
5.6 |
0.5 |
99 |
|
F6 |
5.9 |
0.5 |
99 |
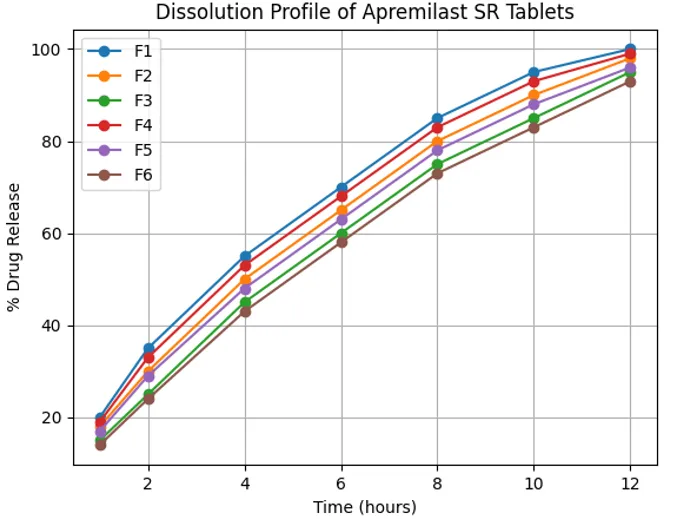
Figure 5: Comparative Dissolution Profiles of F1–F6
The dissolution study demonstrated that polymer concentration significantly influenced drug release behavior.
Formulations F1–F3
These formulations contained HPMC K4M, a lower viscosity polymer. Drug release was comparatively faster due to rapid hydration and quicker diffusion of dissolution medium through the matrix. F1 released almost complete drug within 10 hours.
Formulations F4–F6
These formulations contained HPMC K15M, which has higher viscosity. Increased viscosity resulted in stronger gel layer formation and slower drug diffusion. Drug release was sustained for up to 12 hours.
Effect of Polymer Concentration
Increasing polymer concentration decreased the rate of drug release because:
Optimized Formulation (F5)
Formulation F5 showed optimum sustained release characteristics with:
The release profile of F5 indicated an ideal balance between polymer concentration and drug diffusion characteristics.
Drug Release Kinetics
The dissolution data were fitted into different kinetic models.
Table 6: Drug Release Kinetic Model Analysis
|
Model |
Observation |
|
Zero Order |
Moderate fit |
|
First Order |
Drug release concentration dependent |
|
Higuchi Model |
Best fit |
|
Korsmeyer–Peppas |
Non-Fickian diffusion |
The optimized formulation followed Higuchi kinetics, indicating diffusion-controlled drug release. Korsmeyer–Peppas analysis suggested anomalous transport involving both diffusion and erosion mechanisms. The hydrophilic polymer formed a gel barrier around the tablet, controlling the penetration of dissolution medium and drug diffusion.
Stability Studies
The optimized formulation F5 was subjected to accelerated stability studies.
Table 7: Stability Study Data
|
Time (Months) |
Hardness (kg/cm²) |
Friability (%) |
Drug Content (%) |
Drug Release at 12 hr (%) |
|
0 |
5.2 |
0.45 |
99.5 |
98.2 |
|
1 |
5.1 |
0.48 |
99.0 |
97.8 |
|
2 |
5.0 |
0.50 |
98.7 |
97.2 |
|
3 |
5.0 |
0.52 |
98.5 |
96.9 |
No major changes were observed during the stability study period. Hardness and friability remained within acceptable limits. Drug content showed minimal variation, indicating chemical stability of the formulation. The dissolution profile remained nearly unchanged after storage, demonstrating that the polymer matrix maintained sustained release behavior throughout the study period. The results confirmed that formulation F5 possessed satisfactory stability under accelerated conditions.
CONCLUSION:
The present study successfully developed sustained release matrix tablets of Apremilast using hydrophilic polymers by the direct compression method. Preformulation studies confirmed the suitability and compatibility of the drug with selected excipients. All prepared formulations showed acceptable pre- and post-compression characteristics, including good flow properties, hardness, friability, and uniform drug content. In-vitro dissolution studies demonstrated that polymer concentration significantly influenced drug release behaviour. Among all formulations, batch F5 showed the best sustained release profile with controlled drug release up to 12 hours and satisfactory tablet properties. Drug release followed Higuchi and Korsmeyer–Peppas kinetics, indicating diffusion-controlled release mechanism. Stability studies confirmed that the optimized formulation remained stable under accelerated conditions without significant changes in physicochemical properties or drug release pattern. Overall, the study concluded that sustained release matrix tablets of Apremilast can be successfully formulated to improve therapeutic efficacy, maintain prolonged drug release, and enhance patient compliance in the treatment of psoriasis and psoriatic arthritis.
REFERENCES

Sachin Chaudhari, Hanuman Kolse, Ramesh Ingole, Formulation and Evaluation of Sustained Release Matrix Tablets of Apremilast Using Different Polymers, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 2761-2771. https://doi.org/10.5281/zenodo.20629369
 10.5281/zenodo.20629369
10.5281/zenodo.20629369