
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmaceutics, Konkan Gyanpeeth Rahul Dharkar College of Pharmacy and Research Institute, Karjat, Maharashtra.
Mouth dissolving films (MDFs), also known as orodispersible films, represent a cutting-edge oral drug delivery system designed to disintegrate rapidly on the tongue without water, enhancing bioavailability by bypassing first-pass metabolism. These thin, flexible films address swallowing difficulties in pediatric, geriatric, and bedridden patients, improving compliance through quick onset and taste masking. Key formulation aspects include solvent casting as the primary method, using hydrophilic polymers like HPMC, pullulan, and PVA for film formation, combined with plasticizers such as PEG-400. Drugs like domperidone, antihistamines, and analgesics benefit from solid dispersions with ?-cyclodextrin to boost solubility. Evaluation parameters encompass disintegration time (<60>75% in 15 min). Advantages include no choking risk and superior surface area over tablets, though high-dose limitations persist. Emerging technologies like hot-melt extrusion and 3D printing, alongside nanotechnology, promise personalized dosing and market growth to USD 6.8 billion by 2032. This review explores MDF evolution, methods, polymers/drugs, applications, and future prospects for optimized therapeutics..
Mouth dissolving films (MDFs) emerged in the 1970s as breath fresheners like Listerine PocketPaks, evolving into pharmaceutical dosage forms by the 2000s for enhanced drug delivery. They dissolve in seconds on oral contact, ideal for dysphagic patients affecting ~50% of geriatrics due to conditions like Parkinson's or stroke. Unlike tablets, MDFs offer larger surface area for faster disintegration (<60s), no water need, and reduced choking risk.
MDFs improve bioavailability for high first-pass drugs (e.g., domperidone, 10-15% oral BA) via mucosal absorption, with passive transcellular/paracellular pathways favored by lipophilic, unionized drugs at salivary pH 6.2-7.6. Oral mucosa permeability exceeds skin (4-4000x), with sublingual sites thinnest (100-200μm). Patient compliance rises, especially in pediatrics/geriatrics, with market CAGR 8.5% to 2032. (1,2)
Formulation hinges on water-soluble polymers (45% w/w), APIs (5-30%), plasticizers (0-20%), and saliva stimulants (2-6%). Historical shifts from tablets to films addressed residue/grittiness issues. Regulatory bodies like EMA define ODFs for rapid mucosal dissolution.
Table No.- 01 Advantages and Drawbacks of Mouth Dissolving Film(3)
|
Aspect |
Advantages |
Drawbacks |
|
Dosing |
Convenient, no water, accurate vs syrup |
High doses (>40mg) challenging |
|
Compliance |
High in ped/geriatric, taste-masked |
Bitter drugs difficult |
|
Performance |
Rapid dissolution (>75% in 15min), no choking, large surface area |
Mucosa irritants unsuitable, special packaging |
|
Vs Tablets |
More durable/compliant, faster |
Less dose capacity |
In the solvent casting method for mouth dissolving films, the film-forming polymer (e.g., HPMC, PVA, PVP, pullulan) is first dispersed or dissolved in water or a suitable hydroalcoholic solvent and allowed to hydrate to form a clear, uniform solution, after which a plasticizer such as PEG 400, glycerine, or propylene glycol and other excipients (sweeteners, flavours, saliva stimulants, surfactants, colours) are incorporated with gentle stirring. The drug is then dissolved in an appropriate solvent or uniformly dispersed (or added as a solid dispersion) and mixed into the polymeric solution to obtain a homogeneous casting solution that is subsequently deaerated by standing, vacuum, or ultrasonication to remove entrapped air bubbles. A calculated volume of this solution is poured onto a levelled casting surface such as a glass plate, Teflon plate, or Petri dish and spread using a film applicator to a defined wet thickness so that the final dried film achieves the desired thickness and unit dose per area. The cast film is dried under controlled conditions, typically in a hot air oven or tray dryer at a moderate temperature (around 40–60 °C, below the degradation point of the drug and polymer) until complete solvent removal, then carefully peeled off, visually inspected for defects like cracks or bubbles, and finally cut into uniform strips delivering the required dose and packed in moisture-protective packaging such as alu-alu blisters or sachets to maintain mechanical integrity and rapid disintegration performance in the mouth.(4–7)
Advantages(5,8,9)
Disadvantages(5,8)
Table no. 02 Steps for Mouth Dissolving Film by Solvent Casting Method.(10,11)
|
Step No. |
Step Description |
Key Materials/ Conditions |
Equipment/ Tools |
Time/ Temp |
Potential Issues & Tips |
|
1 |
Gather Materials |
HPMC E15 500 mg, PEG-400 1.5 mL, API 10 mg + β-CD |
Weighing balance |
RT |
Pharma-grade accuracy. |
|
2 |
Prepare Polymer Solution |
Dissolve HPMC in water; add PEG |
Stirrer/ hotplate |
50°C, 30-60 min |
Viscosity 200-500 cps. |
|
3 |
Drug Dispersion |
Knead API: β-CD; sonicate |
Mortar/ sonicator |
40°C, 25 min total |
Tween-80 for wetting. |
|
4 |
Combine & Excipients |
Add to polymer; degass |
Stirrer/ sonicator |
65 min total |
Bubble-free homogeneity. |
|
5 |
Casting |
Pour & spread |
Petri dish/knife |
200-500 μm wet |
Even surface. |
|
6 |
Drying |
Oven to <5% moisture |
Oven |
45-60°C, 4-12 h |
Low RH <40%. |
|
7 |
Peeling/ Cutting |
Cut 2x2 cm strips |
Forceps/blade |
RT |
Gentle peel. |
|
8 |
Packaging |
Foil pouches |
Desiccator |
RT |
Immediate seal. |
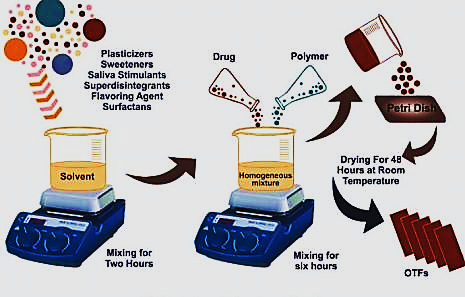
Figure no. 01 Solvent Casting Method(7)
Hot-melt extrusion (HME) for mouth dissolving films is a continuous, solvent-free process where a dry blend of thermoplastic polymer (e.g., PVA, PVP, HPMC), plasticizer (e.g., PEG 400/6000, triacetin; 20–40% w/w), heat-stable API, disintegrants, sweeteners, and flavours is first uniformly mixed using a high-shear mixer, then fed via gravimetric feeder into a co-rotating twin-screw extruder. Inside the extruder (typically 50–180°C barrel zones), shear and heat melt and intimately mix the components at a molecular level for uniform drug dispersion, followed by degassing to remove volatiles. The homogeneous molten mass is extruded through a narrow sheet die to form a thin film (50–200 µm), which is immediately pulled at controlled speed by calendering rollers to ensure uniform thickness, rapidly cooled on chilled rollers to solidify the structure, and finally wound into master rolls for slitting into unit doses and packaging. This method offers superior content uniformity and scalability over solvent casting but requires thermolabile drug avoidance and precise process optimization.(12,13)
Advantages(12,14)
Disadvantages(13,14)
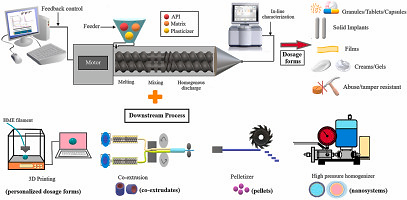
Figure no. 02 Hot-Melt Extrusion (HME)(15)
Table no. 03 Comparison Between Solvent Casting vs Hot-Melt Extrusion vs other methods.(16–18)
|
Aspect |
Solvent Casting |
Hot-Melt Extrusion (HME) |
Semi-Solid Casting |
Solid Dispersion Extrusion |
|
Solvent Use |
Yes (aqueous/organic) |
No (solvent-free) |
Minimal (gel-like matrix) |
No |
|
Temperature |
Low (40–60°C drying) |
High (50–180°C) |
Ambient/room temp |
High (similar to HME) |
|
Equipment Cost |
Low (basic lab setup) |
High (twin-screw extruder) |
Low (mixers, molds) |
High |
|
Scalability |
Batch, lab-scale |
Continuous, industrial |
Batch |
Continuous |
|
Uniformity |
Good, but dose variation risk |
Excellent (molecular mixing) ? |
Moderate |
Excellent |
|
Drug Suitability |
Thermolabile OK |
Heat-stable only ? |
Thermolabile OK |
Heat-stable |
|
Process Time |
Slow (drying step) ? |
Fast (continuous) ? |
Moderate |
Fast |
|
Residue Risk |
Solvent residues possible |
None ? |
Low |
None |
|
Film Defects |
Bubbles, cracks ? |
Brittleness if poor plasticization |
Stickiness |
Minimal |
Hydrophilic: HPMC (film-forming, 5-10%), pullulan (non-gelling), PVA, maltodextrin, NaCMC (45% w/w). Ideal: Non-toxic, wetting, ductile; e.g., HPMC E15 with PEG for tensile strength. Natural (gelatin, fenugreek mucilage) preferred for safety.
Recent innovations in polymers for mouth dissolving films (MDFs), also called orodispersible or fast-dissolving oral films, focus on enhancing disintegration speed, mechanical strength, solubility, and patient acceptability using advanced hydrophilic and nanotechnology-integrated materials.
These hydrophilic film-formers (40-60% w/w dry basis) must be inert, non-toxic, swellable in saliva (pH 6.2-7.6), and economical.(21)
Table no. 04 Common Polymers Categorized by Source(19,20)
|
Type |
Polymer Examples (% in Recipe) |
Properties & Recipe Role |
Common Combinations |
|
Cellulosic (Synthetic/Semi-synthetic) |
HPMC (E5/E15/K4M, 4-10%) |
Excellent film-former; moderate viscosity; controls release; solvent casting staple. |
HPMC E15 + PVA (50:20) for flexibility. |
|
NaCMC/MCC (2-5%) |
Super-disintegrant; enhances wetting/swelling. |
HPMC + NaCMC (6%) for <30s disintegration. |
|
|
HPC (LF/SSL, 3-8%) |
Low viscosity; fast hydration; patented in structured films. |
HPC + pullulan. |
|
|
Vinyl Derivatives |
PVA (Polyvinyl alcohol, 20-50%) |
Strong, flexible films; mucoadhesive; HME-compatible. |
PVA + PEO (40:10) in BEMA® (Belbuca). |
|
PVP (K30/K90, 5-15%) |
Water-soluble; reduces brittleness; taste-masking aid. |
HPMC + PVP (5:3) prevents cracking. |
|
|
Natural/Semi-natural |
Pullulan (5-10%) |
Colorless, non-sticky; oxygen barrier; premium for premium ODFs. |
Pullulan + maltodextrin (8:20). |
|
Maltodextrin/DE rice malt (20-40%) |
Cheap bulking; rapid dissolution; hygroscopic. |
HPMC + maltodextrin (5:30). |
|
|
Gums (xanthan/guar/pectin, 1-3%) |
Thickener; bioadhesive; natural appeal. |
HPMC E5 + pectin (5:2) boosts disintegration. |
|
|
Others |
PEO (Polyethylene oxide, 10-20%) |
High MW for strength; mucoadhesive. |
PVA + PEO in opioids. |
|
Soluplus (5-15%) |
Amorphous stabilizer; HME for poorly soluble drugs. |
Recent patents (WO2024231683A1). |
Added at 10-40% polymer weight to lower Tg (glass transition), improve folding endurance (>300 folds), and prevent cracking. Hydrophilic ones preferred for dissolution.
Table no. 05- Common Plasticizers(18,20,21)
|
Plasticizer |
Typical % (w/w polymer) |
Properties & Effects |
Best With Polymers |
Notes |
|
PEG-400/600 |
15-30% |
Most common; excellent flexibility; non-volatile; boosts elongation (20-50%). Optimal 1.5% in coatings. |
HPMC, PVA, PVP |
Gold standard; reduces brittleness in humid climates (e.g., India). |
|
Glycerol (Glycerin) |
20-40% |
Cheap, humectant; sticky if >30%; fast plasticizing. |
Pullulan, maltodextrin, HPMC |
1-3% optimal; hygroscopic—needs silica. |
|
Propylene Glycol (PG) |
10-25% |
Low viscosity; good for aqueous casting; mild humectant. |
HPMC E5, NaCMC |
1% best for defect-free films; volatile aid. |
|
Triacetin |
5-15% |
Non-hygroscopic; HME-suited; moderate plasticizing. |
PVA, PEO |
Less sticky; for sustained release. |
|
Castor Oil/Dibutyl Phthalate |
5-20% |
Oily; high efficiency but migration risk. |
Synthetic polymers |
Avoid in rapid-dissolve; taste issues. |
|
Natural (Sorbitol, Xylitol) |
10-25% |
Sweetener + plasticizer; cooling effect. |
Maltodextrin, gums |
Pediatric appeal; >20% delays disintegration. |
|
Citroflex (ATBC) |
10-20% |
Bio-based; low toxicity. |
HPMC, pullulan |
Emerging green alternative. |
Low-dose (<40mg), water-soluble, lipophilic: Antihistamines (levocetirizine), analgesics (diclofenac), antiemetics (domperidone, ondansetron), antidiabetics (metformin). Enhancers: β-CD solid dispersions (1:3 ratio). (2,24)
Comprehensive Drugs for MDF Delivery
Mouth dissolving films (MDFs), or orodispersible films (ODFs), are poised for exponential growth, transforming from niche patient-compliant formats to mainstream personalized therapeutics. With a global market valued at USD 3.4 billion in 2025, projected to reach USD 6.5-6.8 billion by 2032 (CAGR 9.3-9.6%), driven by Asia-Pacific (10%+ CAGR) including India, MDFs address dysphagia (affecting 50% geriatrics), pediatric needs, and chronic disease management. Recent 2023-2025 advances in nanotechnology, 3D printing, AI, and hybrid manufacturing overcome traditional limits like low-dose capacity (<40 mg), brittleness, and scaling, promising sustained/controlled release, high bioavailability, and customization.
1. 3D Printing and Personalization
3D printing revolutionizes MDFs via semi-solid extrusion (SSE) and fused deposition modeling (FDM), enabling patient-specific dosing, multi-layer designs, and on-demand production. Unlike solvent casting's uniformity challenges, 3D printing tailors film size/composition (e.g., pediatric 5 mg vs. adult 20 mg), reducing waste by 90%.
2. Nanotechnology Integration (2,14)
Nanotech addresses poor-solubility drugs (BCS II/IV, 40% pipeline), boosting dissolution >90% in <10 min via nanoemulsions, liposomes, and solid lipid nanoparticles (SLNs) embedded in HPMC/pullulan matrices.
3. Advanced Manufacturing: HME and Beyond
Hot-melt extrusion (HME) scales continuously, amorphizing APIs for bioavailability gains (e.g., Soluplus films). 2025 patents emphasize low-tack elasticity (WO2024231683A1: PVA/glycerol/PEG).
4. Therapeutic Expansion and Market Dynamics
Beyond antiemetics/opioids (ondansetron, Suboxone), MDFs target vaccines, biologics (nano-protected), and combos (e.g., migraine analgesics). High-dose (>100 mg) via nano-HME; OTC vitamins/probiotics grow 12% CAGR.
5. Regulatory, Challenges, and Horizons
FDA/EMA guidelines evolve for 3D-printed ODFs (content uniformity, stability). Challenges: High-dose scaling, biologics stability, cost (3D premium). Horizons: AI predictive formulation, smart films (pH-responsive), global access via e-pharma. By 2030, MDFs could claim 15% oral solids market, revolutionizing delivery.
In conclusion, MDFs evolve from compliance aids to smart, personalized platforms, fueled by 3D/nanotech/HME synergies—critical for your thesis on enhanced delivery.
CONCLUSION
Mouth dissolving films (MDFs), also known as orodispersible films (ODFs), have emerged as a cornerstone of modern pharmaceutical innovation, revolutionizing oral drug delivery through their unique ability to disintegrate rapidly on the tongue within 60 seconds without water, thereby enhancing patient compliance, bioavailability, and therapeutic outcomes across diverse populations including pediatrics, geriatrics, and dysphagic patients. This comprehensive review has elucidated the formulation intricacies—from solvent casting and hot-melt extrusion (HME) as primary preparation methods to the pivotal roles of hydrophilic polymers like HPMC E15 (40-60% w/w), pullulan, PVA, and plasticizers such as PEG-400 (15-30%) in achieving optimal film properties including tensile strength (10-30 MPa), folding endurance (>300), and disintegration times under 45 seconds, as demonstrated in recipes for model drugs like domperidone and ondansetron where β-cyclodextrin complexes boost solubility 4-10 fold while masking bitterness. Evaluation paradigms, encompassing in vitro dissolution (>85% in 15 minutes), in vivo volunteer studies for palatability and Tmax reduction (e.g., 15-30 minutes for antiemetics), and comparative scalability of HME over solvent casting for industrial throughput, underscore MDFs' superiority over conventional tablets and ODTs in terms of larger surface area, no choking risk, and partial transmucosal absorption evading first-pass metabolism, yielding 1.5-3x bioavailability gains for BCS Class II/IV drugs.
Therapeutically, MDFs excel with FDA-approved exemplars like Zuplenz (ondansetron), Suboxone/Belbuca (buprenorphine), Sympazan (clobazam), and IGALMI (dexmedetomidine), spanning antiemetics, analgesics, antihistamines, antipsychotics, and cardiovascular agents, while research and patented innovations—such as mitragynine ODFs (US20240307360A1), taste-masked iron films (US20230133317A1), and high-load adrenaline strips (WO2024008954A1)—illustrate expansion to botanicals, nutrients, and high-potency actives, addressing challenges like dose uniformity in microgram ranges and humidity-induced brittleness prevalent in regions like India. Advantages including rapid onset (Tmax 20-40 minutes for fentanyl), abuse deterrence, and reduced GI irritation are balanced against drawbacks such as high-dose limitations (>40 mg), special packaging needs, and thermolabile API constraints, yet recent polymer innovations (e.g., maltodextrin-glycerin, Poloxamer 188) and mucoadhesive hybrids mitigate these, paving the way for sustained-release buccal variants.
Looking ahead, the future of MDFs shines with transformative advances: 3D printing for personalized multi-layer films reducing waste by 90%, nanotechnology via SLNs and nanofibers for >90% dissolution in <10 minutes, continuous HME roll-to-roll manufacturing, and AI-driven quality control, projecting a market surge to USD 6.8 billion by 2032 with Asia-Pacific leading at 10%+ CAGR. Regulatory evolution by FDA/EMA supports these platforms, tackling biologics stability and smart pH-responsive designs for vaccines and chronic therapies. In essence, MDFs transcend mere convenience, embodying a paradigm shift toward precision, patient-centric delivery that enhances clinical efficacy, minimizes adverse events, and democratizes access—positioning them as in drug delivery systems in pharmaceutical sciences.
REFERENCES

Tejasvini Shevale, Dr. Mukesh Patil, Dr. Swapnil Phalak, Dr. Mohan Kale, Innovative Advances in Mouth Dissolving Films: Formulation Strategies for Superior Drug Delivery, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 4, 739-749 https://doi.org/10.5281/zenodo.19415833
 10.5281/zenodo.19415833
10.5281/zenodo.19415833