
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1Department of Biosciences, Integral University, Kursi Road, Lucknow-226026, Uttar Pradesh, India
2Institute of Biosciences and Technology, Shri Ramswaroop Memorial University, Barabanki-225003, Uttar Pradesh, India
3Department of Biotechnology, Era University, Lucknow-226003, Uttar Pradesh, India
Migraine is a prevalent and disabling primary headache disorder characterized by recurrent attacks of moderate to severe head pain accompanied by neurological, gastrointestinal, and autonomic symptoms. It affects more than one billion individuals globally and is a leading cause of disability among young and middle-aged adults. Advances in neuroimaging, molecular biology, and pharmacotherapy have significantly improved understanding of migraine pathophysiology, revealing it as a complex neurovascular disorder involving cortical hyperexcitability, trigeminovascular activation, and neuropeptide release, particularly calcitonin gene-related peptide (CGRP). This narrative review summarizes current knowledge on migraine epidemiology, classification, pathophysiological mechanisms, clinical features, diagnostic criteria, and evidence-based management, with emphasis on emerging targeted therapies and future directions.
Migraine is a chronic neurological disorder classified under primary headache disorders by the International Headache Society. It is characterized by episodic attacks of headache lasting 4–72 hours and associated with nausea, vomiting, photophobia, phonophobia, and functional impairment. Migraine imposes a substantial socioeconomic burden due to reduced productivity, healthcare utilization, and diminished quality of life. Despite its prevalence, migraine remains underrecognized, highlighting the need for continued education and research into its mechanisms and management. Migraine is described as either "a persistent syndrome of headache associated with other symptoms of neurologic dysfunction in varying admixtures" or "an episodic headache associated with certain features, such as sensitivity to light, sound, or movement” [1]. People have long suffered from migraines and the discomfort they cause. Julius Caesar, St. Paul, Thomas Jefferson, and Charles Darwin are just a few of the many individuals who have experienced migraines. An unidentified Sumerian poet from 3000 BC wrote of a condition in which the patient's headache was so bad that they wanted to die to end the suffering. It was thought in Mesopotamia that the awful headache symptoms were caused by the evil spirit of Ti'e attacking its victims. Archaeological digs have revealed skulls, suggesting that medical professionals advised excising portions of the patient's skull to alleviate excruciating headaches [1]. Ergots, triptans, CGRP receptor antagonists, nonsteroidal anti-inflammatory medicines, antidepressants, antihypertensives, and anti-epilepsy medications are among the medications used to treat migraines. Sadly, these are typically only somewhat effective and may have negative side effects like nausea, exhaustion, memory and concentration issues, and digestive disorders. Herbs, spices, and their active ingredients present as an alternative or supplemental intervention to improve the results of existing treatment because they can affect numerous processes related to migraine pathogenesis. Herbal components, for instance, have anti-inflammatory, antioxidant, and antinociceptive properties [2]. The necessity for nutraceutical and herbal manufacturers to demonstrate treatment efficacy, safety, and the quality of products is not as strictly enforced as it is in the pharmaceutical industry because of insufficient industry regulation. This emphasises how crucial it is to support the safety and effectiveness of nutraceuticals by well-designed, randomized-controlled research [2]. The head, commonly known in Latin as "Hemigranea." As a co-morbidity, migraines are a serious problem. Cardiovascular illness, sleep disorders, and psychological disorders are the most common co-morbid conditions associated with chronic migraine. Migraine co-morbidities include tiredness, fibromyalgia, epilepsy, and stroke. Because of the excruciating pain, it affects quality of life and necessitates long-term care [3].
Currently identified vasoactive neuropeptides with strong vasodilating effects include pituitary adenylate cyclase-activating polypeptide (PACAP), calcitonin gene-related peptide (CGRP), SP, and vasoactive intestinal polypeptide (VIP). They are therefore an important area of study to comprehend the mechanisms driving migraines. Migraine rat model to repeatedly stimulate the dura mater with electricity in order to investigate this. Following the administration of electroacupuncture at several locations, it was found to lower blood levels of CGRP, SP, VIP, and PACAP.
This reduces neurogenic inflammation and pain sensitivity [4].
2. Epidemiology
Migraine affects approximately 12–15% of the global population, with significant variation by sex, age, and geographic region. Women are affected three times more frequently than men, likely due to hormonal influences, particularly estrogen fluctuations. Migraine typically begins in adolescence, peaks between 30 and 50 years of age, and often declines later in life. Genetic susceptibility is well established, with first-degree relatives having a markedly increased risk [5]. One of the most debilitating neurological conditions in the world, migraine is one of the main causes of years lived with disability (YLDs). Both during and in between episodes, migraine severely reduces functional ability and quality of life. According to the 2021 Global Burden of Disease (GBD) survey, migraine affects an estimated 1.16 billion people worldwide and is the third most common cause of nervous system disability-adjusted life years (DALYs). According to the GBD 2023 Headache Collaborators, 2.9 billion people worldwide suffered from headache disorders in 2023(13). This translates to a global age-standardized prevalence of 35% and an YLD rate of 542 per 100,000 people. In 2023, migraine accounted for around 90% of YLDs linked to headache disorders, despite tension-type headaches being almost twice as common [13].
The majority of patients receiving migraine care are initially treated by primary care physicians (GPs) in the community. Neurologist referrals are widespread but not required, as patients can see neighborhood neurologists directly without a formal reference. In the public system, specialized headache care is mostly offered in specialized outpatient headache clinics, which usually require referrals and have lengthy wait times. Because of this, some patients, especially those with complex or refractory headache conditions, seek private neurological consultations. Similar trends have been seen in other nations with universal healthcare systems, indicating that coverage by itself does not guarantee prompt or fair access to expert headache care [13].
3. Classification
The International Classification of Headache Disorders, 3rd edition (ICHD-3), categorizes migraine into several subtypes:
3.1 Migraine without Aura
Migraine without aura is another name for the neurological disorder known as hemicrania simplex, or ordinary migraine. It usually causes a moderate to severe headache that starts on one side of the head, pulses or throbs, and gets worse with movement. People often experience nausea and are light-sensitive. Most people have this kind of migraine. Attacks are typically more severe and more frequent than aura attacks. Due to its strong correlation with the menstrual cycle, this kind of migraine is categorised as migraine without aura. The two main types are menstruation-related migraine and pure menstrual migraine. A pure menstrual migraine only happens during the period and not at other times of the cycle, according to ICHD (2004) [4].
3.2 Migraine with Aura
Short-term neurological effects include headaches and vision problems. In contrast, pulsating headaches accompanied by symptoms like light and sound sensitivity and nausea accompany a migraine without aura [6]. Migraine aura is defined as one or more brief, completely reversible neurological impairments that develop over five minutes or more, each lasting between five and sixty minutes, and at least one of which must have a unilateral localization. According to a thorough prospective diary research, 26% of patients have at least one of three auras that persist longer than an hour. This highlights the polythetic issue because it would be a significant waste of resources to investigate an aura that lasts longer than an hour. Maybe 4 hours is a good cut-off, as 5% of auras are longer than that. In addition to the most prevalent deficit, sensory, motor, speech, brain stem, and retinal aura symptoms, approximately 90% of individuals have a visual aura that may exhibit positive (fortification spectra), negative (scotoma), or both phenomena. Aura symptoms might appear before the headache phase, persist throughout the headache phase, or even start during the headache phase [5].
3.3 Chronic Migraine
According to the ICHD-3, a patient is considered to have chronic migraine if they suffer headaches, but not necessarily migraines, on 15 or more days per month for more than three months, with migraine-like symptoms on at least eight days per month. Crucially, the reliance on the patient's ability to precisely recall the number of headache days is a barrier for these diagnostic criteria. It has been suggested that the present definition of chronic migraine be re-examined and the number of days dropped because some individuals experience 8 to 14 headache days per month, but their illness burden is comparable to that of 15 days or more. Patients with a lower threshold may not receive the necessary medical care, which provides additional difficulty in the management of persistent migraines. Chronic migraine onset, which may be explained by genetic predispositions or environmental factors that impact both illnesses, such as stress or life events. In this research, lower affinity to the 5-HT4 receptor was found to be correlated with elevated serotonin levels. Patients with chronic migraines were shown to have elevated serotonin levels during migraine attacks, and this was found to be caused by 5-HT4 receptor downregulation. Serotonin receptors are therefore probably crucial for the onset, maintenance, and management of migraines [7].
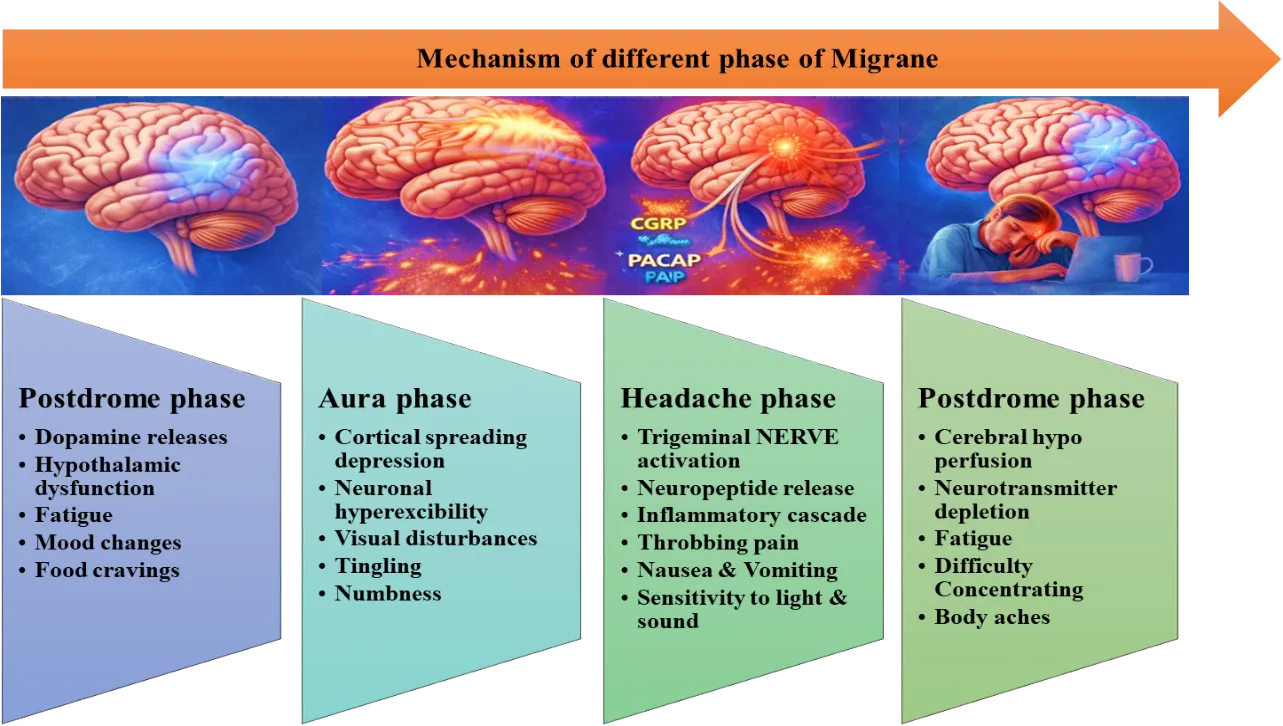
Fig no 1. Phases of a Migraine Attack & timeline illustrating prodrome, aura, headache, and postdrome phases with associated clinical features
4. Pathophysiology of Migraine
For about 600 years, people have been aware of headaches. At the start of the 17th century, the present concept of chronic migraine was recognized. The pathophysiology of migraine was once primarily based on neurological or vascular causes; reports of the disorder's metabolic components were made relatively recently [8]. This applies to functional interictal research since there is no external confirmation that the attack has stopped or that nothing has begun. One could argue that triggered trials offer the benefit of homogeneity with regard to the onset of the migraine attack process. How one accounts for false-negative histories in controls is another general problem that pertains to all migraine physiology research, in fact, all studies that involve controls. For women in North America, the lifetime cumulative incidence of episodic migraine is 43%. It is exceedingly difficult to be certain that a control does not have migraine biology when taking into account probable migraine, chronic migraine, and the heated dispute about overlap with tension-type headache [5].
4.1 Cortical Spreading Depression- Peripheral axons from the trigeminal ganglion innervate the meninges and intracranial blood vessels in the trigeminovascular system. These axons converge centrally in the trigeminocervical complex (TCC), which is made up of the upper cervical spinal cord and the spinal trigeminal nucleus caudalis. Second-order neurons connect to important brain centers in the diencephalon and brainstem, including the locus coeruleus (LC), periaqueductal gray (PAG), and hypothalamus, after ascending from the TCC to thalamocortical neurons. By releasing neuropeptides including calcitonin gene-related peptide (CGRP) and pituitary adenylate cyclase activating polypeptide (PACAP) at the dura mater level, activation of the trigeminovascular pain pathways is hypothesized to mediate some of the characteristics of migraine pain [9]. The two main excitatory neurotransmitters in the brain are glutamate and aspartate. Early research on migraineurs revealed that individuals with migraine with aura had higher levels of these neurotransmitters in between attacks than controls. Plasma glutamate levels have been shown to be higher than aspartate levels between these two neurotransmitters, reaching as high as 0.89 mg/dL and 0.167 mg/dL, respectively. As a result, of the two excitatory neurotransmitters, glutamate has received the most attention and is also observed to be equally elevated in migraineurs without aura [7].
4.2 Vascular theory of migraine's molecular components- The trigeminovascular system is one of the brain regions that are crucial to the pathophysiology of migraine. The trigeminal nerve, facial nerve, glossopharyngeal nerve, and vagus nerve all provide sensory information regarding touch, nociception, and temperature to the trigeminal nucleus, which is located in the medulla of the brain stem. Functional imaging techniques have led to the long-standing association of migraine triggers with the brain stem. In one study, a rise in neuropeptide Y, substance P, and CGRP in external jugular blood was seen after activating the human trigeminal ganglion, challenging the vascular theory by suggesting a possible function for peptides in migraine [7]. There is substantial evidence that the serotonin receptors 5-HT1B and 5-HT1D play a crucial part in migraine discomfort. When serotonin and its agonists are aroused, the 5-HT1B receptors mediate vasoconstriction in the cerebral arteries, reversing the vasodilation in arteries to lessen migraine headache. The 5-HT1D receptor is found in the brain and is involved in preventing the release of nociceptive neuropeptides from the trigeminal system, as well as having minimal vasoconstrictive effects, whereas the 5-HT1B vasoconstrictive effect is also observed in coronary arteries and contributes to its cardiovascular hemodynamic effect. Additionally, nociceptive transmission between the brainstem trigeminocervical complex and the spinal cord is inhibited when 5-HT1B/5-HT1D receptors are activated by serotonin. In essence, when triggered, these receptors help to stop migraine headaches, and the identification of these receptors led to the development of the triptans class of medications [7].
4.3 Central Sensitization- Uncertainty surrounds the mechanism of migraine chronification. The central sensitization theory, one of the most popular theories, suggests that central neurons in the trigeminal nociceptive pathway, particularly the trigeminal nucleus caudalis (TNC), are more excitable. Central sensitization has focused on neurons as the hub of pain information processing, transmission, and integration. Thus, the primary target of many "classic" analgesic medications is neurons. However, a growing body of research indicates that microglia activation either directly or indirectly affects the development of neuronal hyperexcitability, which is crucial for the onset or maintenance of chronic pain conditions like migraine [10]. Different purinergic P2 receptors are induced or enhanced by activated microglia. P2X4R is a member of the P2X family of receptors, which are primarily found in microglia. P2X4R-positive microglia are crucial to the mechanism of neuropathic pain, according to numerous lines of evidence. Neuropathic pain's central sensitization is inhibited by blocking P2X4R expression and activity [10].
The preliminary treatment with TAK-242 reduced the production of IL-1β and prevented IS-induced upregulation of molecules downstream of TLR4, including as MyD88, TRIF, and NF-κB. Furthermore, IS-induced microglia activation and subsequent BDNF release were significantly eliminated by TAK-242. These findings corroborate TLR4's involvement in the hyperalgesia of migraine-related pain and suggest that TLR4 could be a potential target for migraine treatment. Rats treated with IS offered a reliable model for migraine with mechanical hypersensitivity in the face. After dural inflammation, the TLR4-NF-κB signaling pathway plays a significant part in the development of hyperalgesia. TLR4 influences IS-induced microglia activation in the TCC in addition to neuronal regulation. Furthermore, IS-induced hyperalgesia and glia activation were successfully reduced by TLR4 suppression with TAK-242 pre-treatment. However, a number of limitations, including the small sample size and the absence of an evaluation of the chronic process by repeated IS delivery, call for more research [11].
Numerous clinical studies have revealed oxidative imbalance in migraineurs both during headache attacks and during periods without headaches. In migraine patients, studies employing MDA and NO as indicators of oxidative stress and antioxidant enzymes including superoxide dismutase (SOD), glutathione peroxidase (GSH-Px), glutathione reductase (GS-R), and arylesterase produced at least somewhat contentious results (12). In this initial investigation, we discovered elevated oxidative stress in both white matter hyper intensities (WMH) and non-WMH migraineurs and lowered CAT levels exclusively in WMH migraineurs. Thus, measuring serum CAT levels may be useful in predicting the onset of WMH. However, our findings support novel antioxidant defense system-based treatment and monitoring approaches [12].
According to a Danish population-based health databases study, only 7% of patients received preventive medication, and there was a high rate of non-persistence with initial prophylactic treatment. According to a cross-sectional study based on Swedish registries, 12% of people take triptans along with preventive migraine drugs [13].
5. Putative Circulating Biomarkers in Migraine Disorders
5.1 Neuropeptides
The primary excitatory neurotransmitter in the central nervous system, glutamate, and other (neuro)peptides that are thought to be of clinical significance and implicated in the modulation of migraine-related structures [22]. Craniocervical vasodilatation is linked to CGRP, substance P (SP), PACAP, vasoactive intestinal peptide (VIP), and neuropeptide Y (NPY). SP is also involved in plasma protein extravasation, while CGRP and PACAP are involved in peripheral and/or central sensitisation, the primary mechanisms associated with migraine pathophysiology. On the other hand, glutamate has been connected to neuronal hyperexcitability and is crucial in initiating migraine attacks [14].
5.1.1 Calcitonin Gene-Related Peptide (CGRP) - CGRP is a neuropeptide that is a member of the calcitonin family. It is encoded by two distinct genes, CALCA and CALCB, and exists in two isoforms, α and β. While the β form is mostly found in the enteric nervous system, α form is mostly expressed in the central and peripheral nervous systems. Although CGRP plays a significant part in the pathophysiology of migraine, there is ongoing debate regarding its suitability as a biomarker for migraine diagnosis [14].
Higher plasma, serum, saliva, and CSF CGRP levels are seen in EM (episodic migraine) and CM (chronic migraine) patients compared to healthy controls (HC) in a number of studies involving patients evaluated during the interictal phase [14]. To determine if migraine with aura is similar to migraine without aura in terms of CGRP, more research is required. A prior study of normal interictal levels of CGRP in migraineurs contrasts with the current finding of interictally elevated CGRP plasma levels [15]. Since all patients in the current investigation were headache-free at least 72 hours before testing and demonstrated that CGRP levels returned to baseline levels within 2 hours of the attack's conclusion, a phenotypic effect of elevated CGRP levels during the attack seems extremely implausible (15). Adult migraineurs may have dysregulated neurogenic modulation of the cephalic and extra cephalic vasculature, which would explain their elevated interictal CGRP levels. Prior research on migraineurs' cerebral hemodynamic reactions to physiological cues including CO2, O2, and functional engagement has indicated that vascular dysregulation may exist in migraineurs outside of attacks [15].
The trigeminovascular system contains amylin, adrenomedullin, and calcitonin, as well as their receptors; however, their expression and locations vary. In migraineurs, pro-calcitonin and other members of the calcitonin family of peptides were found at different amounts. In particular, procalcitonin serum levels were higher in EM patients during the ictal phase than in HC and the interictal period. 55% of migraineurs experienced migraine attacks after receiving an adrenomedullin infusion for 20 minutes, compared to just 15% of patients who received a placebo [14].
Substance P and CGRP have been linked to dural vasodilation and neurogenic inflammation of trigeminal nerve fibers in the etiology of migraines. There was only one report on interictal CGRP levels, and there were none on SP levels. There have been reports that CGRP levels outside of assaults are much greater than in controls. Study to demonstrate adult migraineurs' plasma SP levels and the strong positive association between SP and CGRP levels. We hypothesize that vascular dysregulation under neurogenic control, one of the key elements in migraine pathogenesis, may be connected to elevated levels of SP and CGRP in interictal migraineurs [16].
5.1.2 Pituitary Adenylate Cyclase-Activating Polypeptide (PACAP) - PACAP comes in two forms (−27 and −38). Both isoforms share structural and functional similarities with VIP and can bind to G-protein-coupled receptors that are less selective (VPAC1 and VPAC2; with equivalent affinity to VIP, PACAP-27, and PACAP-38) to PACAP. However, based on experimental findings using selective modulators, the functional existence of as-yet-unidentified PACAP receptors has recently been suggested [17].
The predominant isoform in neural tissues is PACAP-38. It has been linked to effects that induce differentiation and proliferation in the developing nervous system, as well as cytoprotective, anti-apoptotic, and anti-inflammatory characteristics in a variety of target organs. It is known to play hypophysiotropic, neuromodulatory, and neurotransmitter roles. Only a tiny percentage of small to medium-sized neurons in the TG co-localize PACAP and CGRP. Early research revealed that VIP was only released in a subset of migraineurs who also experienced facial symptoms as rhinorrhea, nasal congestion, and scleral injection (perhaps as a result of the parasympathetic nervous system being activated). Crucially, every cluster headache participant displayed both VIP release and facial symptoms [17].
Additionally, there has been a steady increase in interest in the mechanism behind PACAP's function in migraine. According to studies, PACAP-38 injections may directly stimulate the trigeminal sensory fibers and cause individuals with migraine to experience clear migraine-like convulsions and ongoing extra cranial artery dilatation. It should be mentioned that preproPACAP, the precursor, was the type of PACAP found in our western blot. We cannot rule out the potential that the minor form PACAP-27 was also altered in the migraine model, but an increase in the precursor protein would also lead to a rise in the major active form PACAP (PACAP-38) [18].
Only age and VIP increased the likelihood of being in the OnaBT therapy group after adjustments, but PACAP and age were all greater in chronic migraine patients receiving OnaBT treatment than those without preventatives in univariate analysis. In one trial, CGRP levels dropped from 76.85 pg/mL to 52.48 pg/mL in CM patients deemed responders [19].
5.1.3 Vasoactive Intestinal Polypeptide (VIP) - VIP stands for the most potent neural vasodilator available on that particular bed. VIP-positive nerves originate in the sphenopalatine and otic ganglia, according to tracing studies, but PACAP-positive neurons are present in the human trigeminal ganglion, which lacks VIP immunoreactivity, as well as the aforementioned parasympathetic ganglia [20].
The primary connection between nociception, the development of pain, and related symptoms is provided by TNC activation. The superior salivatory nucleus may be involved in severe activation of the central pain pathways, which could lead to parasympathetic VIP release and the appearance of other facial symptoms [21].
VIP had a migraine induction incidence of 71%, according to the current investigation. Using the same criteria for migraine-induced attacks, VIP caused no attacks in one trial and four attacks (18%) in another investigation involving migraineurs without aura. Notably, the study that reported four patients experiencing VIP-induced migraine attacks was not placebo-controlled, and the results may be in line with the nocebo effect reported in migraine models in humans [22]. VIP in migraine pathophysiology and imply that migraine attacks may be triggered by a prolonged dilatation of the arteries. Perivascular nerve fibers may be activated as a result of the activation of VIP receptors on smooth muscle cells, an increase in intracellular cAMP, and the activation of ion channels. We propose that VIP and its receptor selective antagonists may be viable targets for new migraine medications [22].
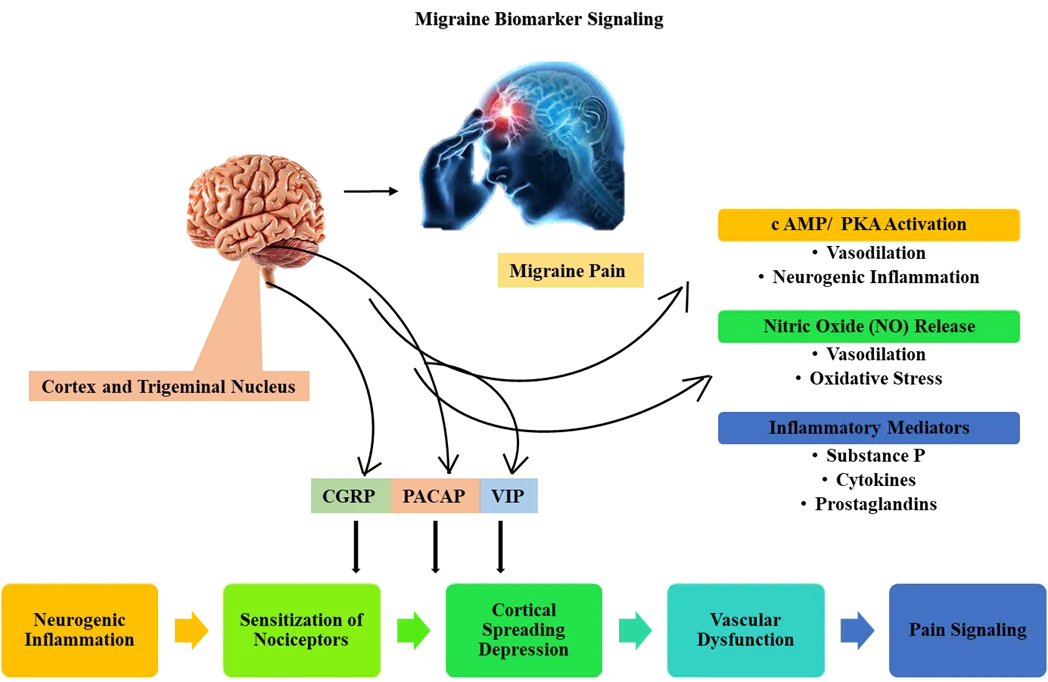
Fig no 2. Neurovascular and Inflammatory Pathways in Migraine Pathogenesis
The reason why PACAP infusion triggers migraine-like symptoms in migraineurs but not VIP infusion is yet unknown. According to the results, it is doubtful that direct vasodilatory action on cerebral vessels is the source of the migraine-like headache brought on by PACAP-38 infusion. VIP and PACAP immunoreactivity has been found in neurons and nerve fibers, but not in satellite ganglion cells, according to the current study. It's interesting to note that both human and rat satellite glial cells exhibited PAC1 and VPAC1 immunoreactivity, suggesting that the peptides may be involved in intraganglionic activity [23].
6. Natural treatments for migraines using herbal remedies
6.1 Feverfew- Potentially the most well-known plant for preventing and treating migraines nowadays is Tanacetum parthenium, also known as feverfew. Originally from central Eurasia, this modest member of the Asteraceae family is now extensively grown throughout North America [24].
An examination of comprehensive questionnaires filled out by roughly 300 consumers produced a wealth of data regarding migraineurs who take feverfew. In order to cover up the bitter taste of the plant, users typically consumed one to four little fresh leaves each day. According to the data, 88% of users experienced actual migraines, with five out of every six being female. They were identical to typical migraine sufferers in every way, with the exception that traditional medications tended to be ineffective. Of the consumers surveyed, 75% had never used any other herbal medicines, and many of those who claimed to have had used vitamin formulations that weren't considered herbal goods [25].
The frequency of chromosomal aberration in lymphocytes and urine mutagenicity are unaffected by long-term preventive use of feverfew, according to toxicity studies. Contact dermatitis has been reported anecdotally. The reported adverse effects in the analyzed trials were mostly modest and transitory. Long-term feverfew users also experienced gastrointestinal issues and mouth ulcers, which were the most commonly reported side effects. Obviously, using feverfew formulations that are more thoroughly made can prevent such issues. Long-term feverfew users reported experiencing a post-feverfew syndrome when they stopped using the medication [26]. Parthenolide was thought to be the active ingredient in feverfew extract until recently. In vitro tests that highlighted the biological activity of feverfew provided evidence in favor of this theory. These investigations showed that the plant inhibits serotonin release from blood platelets and leucocytes as well as platelet aggregation [26]. It is interesting to examine the results of the examinations of the capsules and tinctures into the parthenolide unit amounts and the suggested daily consumption amounts [27].
At 30 minutes, parthenolide (1 x 10(-5) mol/L) non-competitively counteracted the effects of d-fenfluramine, but it had no discernible effect on 5-HT2B and 5-HT2A receptors in the rat fundus and ileum. However, this effect became significant when the incubation period was extended to 1.5 hours in the rat fundus. 5-HT2B and 5-HT2A receptors were immediately and strongly inhibited by feverfew extract (1 x 10(-5) mol/L), which also released 5-HT from neurons. The extract effectively and permanently prevented the aforesaid at 5 x 10(-5) mol/L. Extract could considerably block 5-HT receptors and neuronal release of 5-HT when thermally deteriorated up to 10%; however, it drastically lost its inhibitory effect upon further degradation [28].
6.2 Butterbur - Butterbur, or Petasites hybridus, is a perennial native to Europe that thrives on the sides of streams and other damp places. For ages, it has been utilized in medicine. Its analgesic and spasmolytic properties are used to treat a variety of ailments, including back pain, asthma, migraines, and urinary tract spasms. These effects are mostly ascribed to a class of sesquiterpene chemicals called petasins [29].
The distinct butterbur extract was administered to 187 migraineurs at doses ranging from 100 to 150 mg per day for a minimum of three months. With the exception of “gastric venting," no discernible differences were found between the product and placebo in terms of adverse events that were deemed to be at least potentially causally connected. This well-known side effect, which affected roughly 20% of research participants, is mild and temporary. Approximately 90% of trial participants gave global tolerability a "good" or "excellent" rating [29].
The extract of butterbur root (Petadolexs) is marketed as a natural treatment to prevent migraines. In comparison to a placebo, the overall effect size of the 150 mg extract dose appears to be small (about a 15% lower migraine frequency rate each month or a 15% higher responder rate (in terms of more than 50% improvement) [30].
For the prevention of migraines, 150 mg of Petasites root extract (Petadolexs) used daily for three to four months has shown moderate evidence of efficacy [30].
The fact that both butterbur root and music therapy reduced headaches more than a medication placebo when completers were examined provided evidence of their effectiveness in preventing pediatric migraines [31].
6.3 Riboflavin (Vitamin B2) - Human absorption of riboflavin occurs via active transport. As a result, the process is competitive, saturable, and particular; that is, structures that resemble riboflavin may compete with its absorption. In the human intestine, riboflavin is mostly absorbed in the upper ileum [32].
Examine therapeutic options for preventing episodic migraine headaches. Using this technique, clinical trials are rated as Class I, II, III, or IV based on how rigorous the study's methodology was. Evidence-based recommendations for different pharmaceutical treatments for migraine headache prevention are then derived from these categories of clinical research. Level A recommendations call for at least two Class I trials; Level B calls for one Class I or two Class II studies; Level C calls for one Class II study; and Level U denotes insufficient or contradictory data [32].
A placebo comprising 850 mg of microcrystalline cellulose and 0.473 mg of β-carotene or riboflavin 400 mg/d was randomly assigned to 55 patients who met the International Headache Society (HIS) diagnostic criteria for migraine headache with and without aura. The main outcome of the three-month research was a shift in the frequency of attacks from the run-in period to the final treatment month [32].
6.4 Magnesium - 81 migraineurs who received 600 mg of trimagnesium dicitrate once daily in a bigger double-blind, placebo-controlled, randomized research reported a 41.6% decrease in attack frequency in the magnesium group and a 15.8% decrease in the controls. 18.6% of patients reported diarrhea, 4.7% reported gastrointestinal irritation, and three patients withdrew from the research owing to adverse effects [33].
Pediatric migraineurs with or without aura have lower amounts of magnesium in their serum, red blood cells, and mononuclear blood cells than patients with tension-type headaches and controls, indicating a magnesium shortage. In order to avoid pediatric migraines, magnesium supplementation may be a safe and well-tolerated migraine prophylactic. Nevertheless, the difference in the slopes of the two lines was not statistically significant, even though a double-blind, placebo-controlled, randomized study of patients aged 3 to 17 years revealed a statistically significant decline in headache frequency in those treated with magnesium oxide [33].
Furthermore, a two-week study revealed that migraine patients intracellular erythrocyte magnesium concentrations considerably rose in comparison to those of healthy controls when they drank mineral water containing 110 mg/L of magnesium daily (varying from 7.4 to 12 mmol per day for 15–18 days) [34].
6.5 Ginger (Gingerol) - The Zingiberaceae family includes the plant Zingiber officinalis, often known as ginger. "The rhizome is used to make medication that treats acute migraine headaches." It has anti-inflammatory qualities, eases nausea, and calms the stomach. Migraine sufferers may benefit from it because it includes volatile oils and other substances. Ginger has shown significant promise in terms of analgesic effectiveness [4, 35].
Three times a day, 500–600 mg of ginger powder combined with water was found to be an effective migraine preventive treatment with no known adverse effects. Our meta-analysis, which comprised 227 individuals, revealed that the addition of ginger was linked to significantly better pain-free at 2 hours and lower pain scores at 2 hours following treatment in migraine patients, but it had no discernible impact on treatment response [35]. According to the findings of our meta-analysis, ginger has a beneficial effect on migraine patients' nausea and vomiting. The total number of adverse events was comparable between the control group and the ginger group. These suggested that migraineurs could safely use ginger [35].
In this study, we will look into how ginger might affect inflammatory biomarkers like C-reactive protein, calcitonin gene-related peptide, and tumor necrosis factor. Therefore, more research is recommended to characterize how ginger affects inflammatory factor levels in migraineurs. It appears that ginger can be used to FDA-approved medicines to avoid prophylaxis; because ginger is readily available, inexpensive, and has mild side effects, it is easy to benefit from its positive effects [36].
6.6 Turmeric - The primary ingredient of the annual herb Curcuma longa, also referred to as turmeric, is curcumin, a polyphenol that has been utilised for thousands of years. It was first isolated in 1815 [37].
Curcumin's anti-inflammatory and antioxidant qualities have been linked to its mode of action in the treatment of migraines. Numerous studies have examined the connection between oxidative stress, inflammatory factors (calcitonin gene-related peptide, IL-6, IL-1β, and TNF-α, etc.) and migraine, but the exact processes behind migraine aetiology remain unclear [37].
When compared to a placebo, 80 mg nano-curcumin supplementation daily for two months decreased migraine attacks (SMD −0.55; 95% CI: −1.07 to −0.02), severity (SMD −0.64; 95% CI: −1.10 to −0.19), and duration (MD −2.90; 95% CI: −4.66 to −1.13). Combining nano-curcumin with nutraceuticals like omega-3 and coenzyme Q10 showed improved efficacy in lowering migraine attacks (SMD 1.19; 95% CI: 0.90–1.48). A before and after intervention analysis revealed a decrease in migraine attacks (SMD −0.77; 95% CI: −1.00 to −0.54), severity (SMD −0.92; 95% CI: −1.50 to −0.33), and length (SMD −0.63; 95% CI: −1.05 to −0.20) among individuals who solely received nano-curcumin supplementation [38].
6.7 Menthol - Because of its well-known cooling, analgesic, and muscle-relaxing qualities, peppermint oil—which is extracted from the Mentha piperita plant—is a common natural treatment for migraines and headaches. By blocking calcium channels, suppressing pain signals, and creating a cooling sensation that relieves tension and vascular discomfort frequently linked to migraines, its primary ingredient, menthol, has a therapeutic effect [39].
When applied topically, a 10% menthol in ethanol solution outperformed a placebo in terms of pain-free, pain-relieving, pain-free, and sustained pain-relieving end-points. Additionally, menthol solution was more successful in reducing related symptoms. Menthol application was linked to more adverse events than the placebo, however this difference was not statistically significant. Additionally, drug intolerance only caused 5.7% of the intent-to-treat group to withdraw from the trial. Menthol may prevent higher brain regions from receiving nociceptive impulses from the pain-producing cranial arteries through branches of the trigeminal nerve. Menthol's ability to activate the two types of "transient receptor potential cation channel, subfamily M" (TRPM) receptors explains its analgesic effects [40].
Its rapid in action cutaneous application most likely minimizes systemic consequences. Additionally, menthol can be utilized as an adjuvant in transdermal patches that contain ergots and triptans, two more migraine therapies that are ineffective [40].
However, menthol had no impact on TRPM8 mutant animals, and its effect was inhibited by co-administration of the TRPM8 antagonist AMTB on the dura mater. In contrast, dural treatment of menthol decreased the duration of nocifensive behavior induced by meningeal application of inflammatory mediators in mice. Meningeal inflammation increases the expression of TRPM8 in first-order trigeminovascular neurons, and icilin-induced facial TRPM8 activation can reduce pain by opposing TRPV1 at the TG neuron level in mice [41].
6.8 Salicin (Willow Bark) - Salicin (SA), the main active components in and White Willow (Salix alba), respectively, have been traditionally used as a remedy for various types of pain, including headaches [42]. These outcomes provide more evidence in favor of using S. alba-based dietary supplements to prevent and/or reduce migraine attacks. There could be other reasons for the blunting effects on serotonin decomposition and nitrite levels [43].
In addition to the conventional salicylate pathway, various biochemical pathways linked to inflammation and metabolic control are impacted by the consumption of salicin and salicinoids. There have been reports of decreases in pro-inflammatory lipid mediators such as prostaglandin E₂ (PGE₂), leukotriene B₄, and downstream eicosanoid signaling products, as well as modifications in oxylipins generated from arachidonic acid and certain lysophospholipids. Additionally, changes in phenolic conjugates and metabolites associated with oxidative stress have been observed, indicating a wider metabolic footprint than salicylate exposure alone [44]. Salicin enhanced behavioural performance, reduced oxidative and inflammatory indicators, and enhanced nerve conduction, indicating possible neuroprotective advantages beyond its conventional analgesic role [44].
6.9 Ginkgolide B - The leaves of the Ginko biloba tree are used to extract Gingkolide B, a natural anti-platelet activating factor (PAF) (45). G. biloba extract is extensively sold as an herbal treatment and dietary supplement for a number of illnesses, such as inflammatory diseases, cardiovascular problems, and cognitive impairment [46].
PAF has been shown to be a potent nociceptive and pro-inflammatory substance that is released during an inflammatory process. Furthermore, glutamate acid, the primary excitatory neurotransmitter in the central nervous system, is modulated by gingkolide B. PAF released by platelets and leukocytes during the first phase of migraine without aura assaults sensitizes the trigeminal-vascular terminals causing pain, and aberrant glutamate levels in sensitive individuals can trigger migraine aura and spreading depression [45].
6.10 Linalool (Lavender oil) - Linalool and linalyl acetate are the two main volatile components of lavender (Lavandula angustifolia) oil, which is widely used in fragrances, cosmetics, and medications. The beneficial biological benefits of inhaled volatile compounds are believed to be caused by their rapid actions via the limbic system [47].
The results showed that adults' postoperative pain is significantly reduced by inhaling lavender aromatherapy [47]. 92 of the 129 headache bouts that were reported reacted either completely or partially to lavender. In the first two hours of using lavender, all respondents experienced a complete or partial reduction in headache (5% in the first 30 minutes, 20% in the second 30 minutes, 32% between 1 and 1.5 hours after using lavender, and 43% between 1.5 and 2 hours after treatment). Thirty-two of the sixty-eight headache attacks that were reported in the control group either fully or partially reacted to a placebo. In the first two hours of treatment, 89% of respondents in the placebo group replied. The proportion of responses was significantly higher [48]. This study demonstrates that lavender is at least as effective as subcutaneous sumatriptan and may even be better than oral triptans, acetaminophen, NSAIDs, and ergot substances in the treatment of migraine symptoms [48].
Using linalyl acetate (0.6%) and linalool (0.4%), the lavender essential oil was standardized.
Lavender's soothing, analgesic, and sedative properties as well as its effectiveness in treating anxiety disorders have been demonstrated by earlier research. These results suggest that the herb influences the nervous system physiologically. These effects, particularly the analgesic one, indicate that lavender oil may be helpful in lowering the frequency and severity of migraines [49].
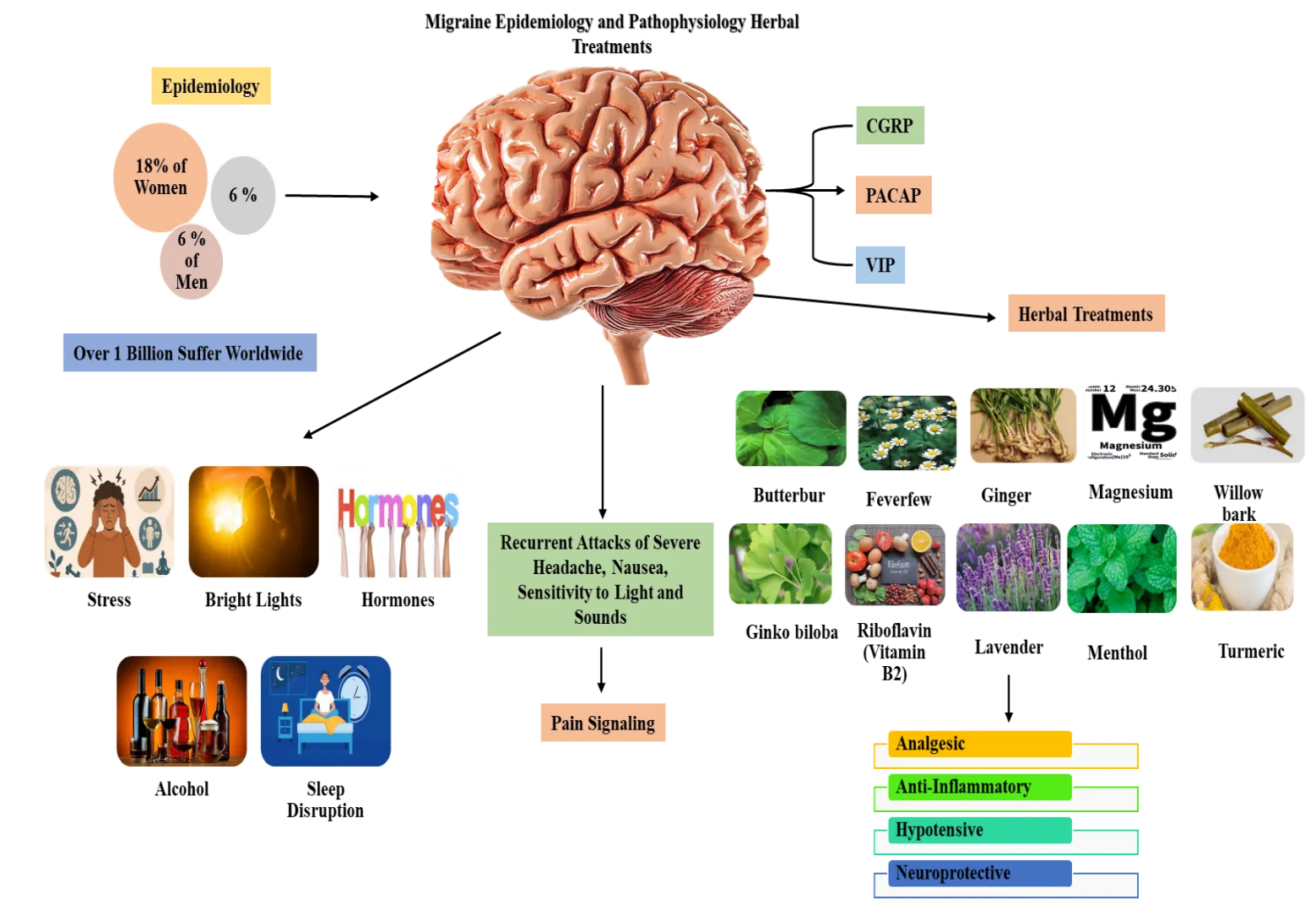
Fig no 3. Migraine Pathophysiology, Epidemiology, and Herbal Therapeutic Targets.
Table 1. Classification of CNS Acting Drugs, Antihistamines, Triptans and Analgesic Agents
|
Drug to control Migraine attacks & Pain |
||||
|
S. No. |
Antidepressants & CNS acting agents |
Antihistamines |
Triptans |
Others |
|
1 |
Amitriptyline /Nortriptyline |
Diphenhydramine |
Sumatriptan (prototype drug) |
Aspirin |
|
2 |
Fluoxetine/ Duloxetine |
Promethazine |
Rizatriptan |
Naproxen sodium |
|
3 |
Citalopram/ Escitalopram |
Chlorpheniramine |
Zolmitriptan |
Nimuslide + Paracetamol |
|
4 |
Sodium Valproate / Valporic acid |
Cetirizine |
Naratriptan |
Ketorolac |
|
5 |
Sertraline |
Fexofenadine |
Eletriptan |
Ibuprofen |
|
6 |
- |
Loratadine |
- |
Indomethacin |
7. Analgesics and NSAIDs in Migraine Treatment- Numerous clinical investigations have shown the effectiveness of aspirin, paracetamol. Less effective, paracetamol is mainly helpful for those who cannot take NSAIDs. While intravenous paracetamol has insufficient proof, intravenous ketorolac is likely effective. In terms of intranasal formulations, there is not enough data to support inhaled corticosteroids and ketorolac nasal spray [22].
Second-line treatments for headaches are triptans, which are 5-HT1B/1D receptor agonists. Triptans work by constricting cranial arteries and inhibiting the production of neuropeptides, which helps reduce pain [22].
In head-to-head comparisons, the most widely evaluated medications for migraine prevention (topiramate, valproate, propranolol, botulinum toxin type A, and amitriptyline) were frequently contrasted with one another. With the exception of valproate, a number of more recent treatments (such as CGRP antagonists and transcutaneous supraorbital stimulation) provided migraine reductions that were either slightly bigger or nearly comparable, but they also had less side effects and dropout rates. Valproate showed the biggest migraine decrease of any treatment used to prevent migraines: a pooled analysis of seven trials revealed a reduction of 3.4 migraine days per month, albeit this data was deemed low quality. In particular, valproate significantly reduced the frequency of chronic migraine (13.2 migraine days per month) while having less of an impact on episodic migraine [50].
CONCLUSION
Significant personal, financial, and societal costs are associated with chronic migraine, a very crippling condition. It is still unclear how chronic migraine develops from episodic migraine. It has been suggested that anatomical alterations in the brain, increased cortical hyperexcitability, central sensitisation, and dysfunction of the descending pain modulatory pathway are significant factors in the development of chronic migraine. It is plausible that chronic migraineurs are in a continuous premonitory phase, which may sustain abnormalities in the descending pain modulatory pathway, cortical hyperexcitability, and central sensitisation, despite our limited understanding of the underlying pathogenesis of this condition.
The etiology of migraine and the potential effects of Herbal therapy, using validated scales, biomarkers, neuroimaging, autonomic response evaluations, and a sufficient sample size to more accurately comprehend the neurobiology of Herbal therapy. Migraineurs, who formerly suffered from a disorder that was frequently disregarded and poorly treated, are now receiving innovative treatments that are increasingly customized to meet patient needs and are radically changing how we view the illness.
ACKNOWLEDGEMENT
The author would like to thank Juveriya and Neda for their valuable contributions, discussions, and support during the preparation of this review article.
CONFLICTS OF INTEREST
There is no conflict of interest.
REFERENCES



Hira Moid, Juveriya Israr, Neda Fatima, Migraine as a neurovascular disorder: Insights into pathogenesis, biomarkers, and treatment, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 5, 7248-7266. https://doi.org/10.5281/zenodo.20407832
 10.5281/zenodo.20407832
10.5281/zenodo.20407832