
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Dr. D. Y. Patil college of pharmacy, Akurdi, Pune, Maharashtra, India
This review summarizes the current evidence regarding the chemistry, mechanism of action, antimicrobial spectrum, pharmacokinetics, pharmacodynamics, clinical efficacy, and therapeutic potential of nafithromycin. Nafithromycin [ also called WCK-4873] is marketed under the brand name Miqnaf, is an India’s first indigenously developed antibiotic targeting drug-resistant infections. Nafithromycin is developed by Wockhardt limited with support from biotechnology industry research assistance council. It is approved by CDSCO for the treatment of community-acquired bacterial pneumonia [CABP]. It is the first new antibiotic of its kind to be made in the world in more than 30 years. Nafithromycin is a new third generation ketolide macrolide that comes from erythromycin. It works well against a wide range of pathogens, including Streptococcus pneumonia and Staphylococcus aureus that are resistant to macrolides. It is nearly ten times more effective than azithromycin, has good lung tissue penetration and has a good safety record. Analytical characterization and validation of nafithromycin have been performed using RP-HPLC, RP-UPLC, and UHPLC-MS techniques, demonstrating robust analytical performance. The USFDA also gave nafithromycin the designation of Qualified Infectious Disease Product [QIDP]. In general, it looks like a promising short-term treatment against drug-resistant respiratory infections. In this review article current knowledge of nafithromycin, covering its introduction, chemical characteristics, MOA, antimicrobial spectrum, pharmacokinetic and pharmacodynamics, etc. highlighting its emerging role as a promising therapeutic option for respiratory tract infections.
Nafithromycin is a new semi-synthetic, fourth-generation macrolide antibiotic that comes from the ketolide subclass and is made from Streptomyces species [2,5].
It is India's first macrolide antibiotic that was developed in the country. Wockhardt Limited made it with help from the Biotechnology Industry Research Assistance Council (BIRAC) [10]. It was officially released on November 20, 2024, and was sold under the brand name Miqnaf. This was a big step forward for India in the fight against antimicrobial resistance (AMR) [10].
Nafithromycin is a modified version of erythromycin that has a 14-membered lactone ring. It also has some new features, such as a keto group at the C3 position that replaces the cladinose sugar and a unique thiadiazole–pyridine side chain [2,3].
These structural changes make it easier for ribosomes to bind, help the drug get into the lungs, and make it work against bacteria that are resistant to treatment [3,4].
Its molecular structure effectively gets around common ways that macrolides become resistant, such as Erm-mediated methylation, efflux pumps, and ribosomal mutations [3,5].
Nafithromycin works by binding to the 50S subunit of the 70S ribosome, which stops peptide chain elongation and stops bacterial protein synthesis [1,2].
It also stops the biosynthesis of peptidoglycan, which has both bacteriostatic and bactericidal effects [4]. This dual mechanism makes it work better against a wide range of pathogens [5].
Nafithromycin demonstrates significant efficacy against Gram-positive pathogens, including Methicillin-resistant Staphylococcus aureus (MRSA), Vancomycin-resistant Enterococcus (VRE), and Streptococcus pneumoniae , encompassing macrolide-resistant variants [2,4].
It also works against unusual respiratory pathogens like Mycoplasma pneumoniae and Chlamydophila pneumoniae [3].
Compared to regular macrolides like azithromycin, nafithromycin is much stronger and still works against organisms that are resistant to multiple drugs [5,9]. Nafithromycin exhibits pharmacokinetics characterized by fast absorption, high bioavailability after oral administration, broad tissue distribution, and elevated concentrations in the lungs [1,11]. Specifically, nafithromycin has higher concentrations in lung epithelial lining fluid and alveolar macrophages than in plasma, making sure that the drug can be delivered effectively to the infection site [3]. Nafithromycin’s long half-life enables once-daily dosing of the drug [1]. In clinical practice, nafithromycin has mainly been used for treating CABP caused by resistant bacteria [6,10]. According to clinical trials, nafithromycin is as effective as seven-day therapy based on moxifloxacin in curing CABP in a three-day period when taken orally once daily, with cure rates higher than 95% [6].
Nafithromycin is well-tolerated, with only mild side effects of the digestive system reported. There have been no reports of hepatotoxicity or nephrotoxicity [1,11].
The introduction of nafithromycin can be seen as the response to an urgent need for an effective drug that would provide treatment in cases of resistant infections of the type mentioned above, which is characterized by either insufficient coverage, lack of safety, or poor pulmonary absorption of currently available medications [5,7].
Being the first representative of its class launched in more than thirty years, nafithromycin provides a new effective treatment option [5,8].
In conclusion, it can be said that the introduction of this antibiotic was a step forward in terms of antibiotic innovation, improving India’s standing among the world leaders in the development of pharmaceuticals [8,10].
1.1 STRUCTURE OF NAFITHROMYCIN:
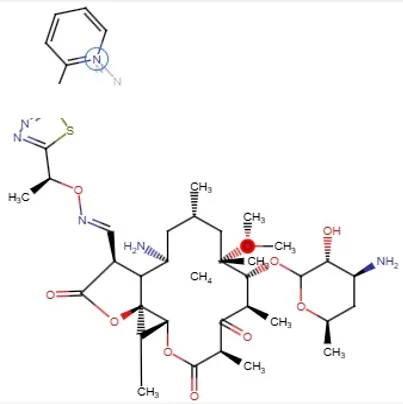
Chemical formula: - C42H62N6O11S
Chemical Class: Macrolide (ketolide)
Basic Structure:
Nafithromycin has a very large 14-membered lactone ring that is typical of macrolide antibiotics.
Important Structural Elements:
1. Macrocycle/lactone ring: Large ring consisting of 14-membered atoms with an ester (lactone) bond in the center.
Sugar units:
2. Attached to the lactone ring are some modified sugar units (desosamine type), which assist in bacterial ribosome binding.
3. Keto group:
In contrast to traditional macrolides such as erythromycin, Nafithromycin contains a keto group (C=O), making it a ketolide.
4. Substituent/side chain:
Has elongated side chains, thereby increasing its:
Binding efficiency to ribosomes
Resistance to resistant strains
5. Fluorinated derivative:
Improves potency and pharmacokinetics.
With the ketolide structural modification, nafithromycin can:
1.2 MOA: -
Nafithromycin is an innovative lactone ketolide antibiotic based on macrolides and designed for treating pathogenic respiratory bacteria that have become resistant to other types of antibiotics and with higher effectiveness [5,20,41]. It is capable of reaching effective concentrations intracellularly through passive diffusion into bacteria along with accumulation in target tissues, especially in lung epithelial lining fluid and macrophages [1,34,42].
Once entered the bacterial cell, nafithromycin interacts with the 50S ribosomal subunit. More specifically, the drug targets domain V of 23S rRNA, like most other macrolides do. The difference is in the increased affinity to this site due to the special structural modification of the drug's structure [20,41]. The structural changes made to its ketolide backbone, especially changes to the lactone ring, provide a better binding affinity for the ribosomes compared to previous macrolides [12,20,50].
Nafithromycin exerts its antibacterial effect by disrupting the translocation stage in the process of translation and hindering the relocation of the growing peptide from the A-site to the P-site on the ribosome [41,49]. Such an interference results in the inhibition of protein synthesis and thus prevents the development of bacteria [52].
What makes nafithromycin unique among other macrolides is its ability to interact with two sites of ribosomes simultaneously. This characteristic not only improves its bactericidal properties, but also provides additional resistance to the development of resistance [20,28].
Notably, nafithromycin was specifically developed to combat resistance that develops against macrolides, such as the presence of efflux pumps and ribosomal methylation (Erm-mediated resistance), because of its structural changes [28,43]. This makes it effective against macrolide-resistant bacteria such as Streptococcus pneumoniae [3,4,29].
Nafithromycin may exhibit a bacteriostatic action depending on the dose or bactericidal action if there is an increased dose against sensitive organisms [41,52].
1.3 Chemical Classification:
Nafithromycin is a new type of antibacterial drug that is part of the ketolide subclass of macrolide antibiotics. It is a more advanced version of this type of drug [12,13]. It is generally regarded as a fourth-generation macrolide antibiotic, engineered to address the shortcomings of previous macrolides, such as inadequate stability and the development of bacterial resistance [13,14]. Nafithromycin is a semi-synthetic derivative of erythromycin that keeps the basic macrocyclic lactone ring structure that is typical of macrolide antibiotics [12,14].
The core structure that gives it its antibacterial properties is this macrocyclic framework, which is usually a 14-membered lactone ring [14,16]. Nonetheless, Nafithromycin possesses essential structural alterations that differentiate it from traditional macrolides [13,17].
A characteristic of ketolide antibiotics, such as Nafithromycin, is the substitution of the L-cladinose sugar moiety at the C3 position with a keto (carbonyl) group [14,17]. This change makes the acid more stable and makes it much less likely that resistance will happen through ribosomal methylation and efflux mechanisms [17,18]. Consequently, Nafithromycin demonstrates enhanced binding affinity to bacterial ribosomes relative to prior macrolides [13,18]. Nafithromycin has a keto group that makes it a ketolide, but it also has unique structural elements, such as a amidoxime functional group and an extended biaryl side chain made up of heterocyclic rings (e.g., pyridine and thiadiazole) [14,17,19]. These substitutions lead to stronger and dual-site binding interactions with the bacterial 50S ribosomal subunit, which makes the drug more effective against bacteria and gives it a wider range of activity, especially against bacteria that are resistant to other drugs [18,19].
Nafithromycin is a macrocyclic, ribosome-targeting protein synthesis inhibitor with better pharmacodynamic and pharmacokinetic properties from a medicinal chemistry point of view [12,18].
Its chemical structure makes it effective against strains that are resistant to macrolides, making it a promising treatment for community-acquired bacterial infections [13,14,18].
In short, Nafithromycin is a semi-synthetic, macrocyclic lactone antibiotic of the ketolide class . It has been chemically modified in strategic ways, such as adding a C3 keto group and making advanced side-chain substitutions, which all work together to make it more stable, better at binding to ribosomes, and more resistant to other drugs [12-19].
1.4 RESISTANCE BREAKING PROPERTIES OF NAFITHROMYCIN: -
Nafithromycin, a novel ketolide antibiotic, has garnered significant attention due to its enhanced efficacy against bacterial resistance compared to conventional macrolides, particularly in respiratory infections where resistance is becoming more prevalent [20].
A major reason for this better performance is that Nafithromycin binds to both domains II and domain V of the 23S rRNA in the 50S subunit at the same time. This makes the binding more reliable and secure than with older drugs [21].
The drug still works even when bacteria use Erm-mediated methylation, which is a resistance mechanism that usually makes antibiotics less effective by making themselves less able to bind to bacteria [22].
Nafithromycin not only eliminates target modification, but it also has limited susceptibility to efflux pump systems, like those developed by mef genes. This means that it can stay inside bacterial cells at concentrations high enough to kill bacteria [22].
Another important thing is that it can still work even when the ribosome’s structure changes, like when proteins L4 and L22 mutate, which is known to make macrolide binding harder in resistant strains [22].
This resilience is further bolstered by its relatively greater affinity for the ribosomal target, indicating that even minor bacterial defense mechanisms frequently fail to dislodge the drug once it is bound [23].
From a clinical standpoint, Nafithromycin has exhibited consistent efficacy against multidrug-resistant Streptococcus pneumoniae , including strains that are unresponsive to standard macrolides and other antibiotic classes [24]. Nafithromycin is especially interesting because it can target multiple resistance pathways at once, such as ribosomal modification, active drug efflux, and structural mutations. This makes it less likely that the treatment will fail [24].
Pharmacokinetic observations provide an additional benefit, as the drug attains elevated and prolonged concentrations in lung tissues, particularly within epithelial lining fluid and alveolar macrophages, which are critical infection sites in pneumonia [24]. Interestingly, its shorter treatment duration, usually only three days, may also lessen the selective force on bacteria, which could slow down the development of more resistance compared to longer treatment courses [22].
Nafithromycin has also been effective against strains that are less sensitive to both traditional macrolides and some older ketolides. This shows that it is a significant improvement in this class of antibiotics [25].
These features indicate that Nafithromycin is not merely an addition to the macrolide family, but a strategically engineered compound capable of circumventing various bacterial resistance mechanisms concurrently [20].
1.5 ANTIMICROBIAL SPECTRUM
1. A look towards the antimicrobial spectrum
Nafithromycin is a new type of ketolide antibiotic that works against a wide range of bacteria, both typical and atypical, that cause respiratory infections. It is very effective against Gram-positive organisms, some Gram-negative bacteria, and pathogens that live inside cells. [27]. The drug has been carefully designed to get around common ways that macrolides become resistant, like ribosomal methylation and efflux pumps. [28]
2. Activity Against Gram-Positive Organisms
Nafithromycin displays remarkable activity against various Gram-positive microorganisms that contribute to respiratory infections. [29] The drug is extremely potent against Streptococcus pneumoniae (multi-drug resistant (MDR), macrolide-resistant, and penicillin-resistant). [28] Moreover, it possesses remarkable efficacy against Streptococcus pyogenes and Staphylococcus aureus (methicillin-susceptible and selected MRSAs). [30] It has been observed through research that nafithromycin shows greater potency than classic macrolides like clarithromycin and azithromycin. [31] It should be noted that the antibiotic maintains its efficacy against telithromycin-resistant microorganisms owing to
3.Effectiveness Against Gram Negative Bacteria
Nafithromycin is moderately effective against some Gram negative bacteria that can be found in respiratory tracts. [32]
This antibiotic is effective against Haemophilus influenza and Moraxella catarrhal is which cause respiratory tract infections. [31]
This antibiotic shows poor effectiveness against other Gram negative bacteria including Enterobacteriaceae and Pseudomonas aeruginosa. [32]
4. Effectiveness Against Atypical Pathogens
Nafithromycin has excellent effect against atypical intracellular pathogens. [33]
Nafithromycin is very effective against Mycoplasma pneumoniae, Chlamydia pneumoniae, and Legionella pneumophila. [33]
In addition, this antibiotic reaches high concentrations intracellularly, especially inside macrophages.
5. Activity Against Drug-Resistant Strains
Another significant strength of nafithromycin is its effectiveness against drug-resistant bacteria. [28]
It continues to be active against macrolide- and β-lactam-resistant strains of Streptococcus pneumoniae. [28]
Since the compound binds to more than one domain of the 50S ribosomal subunit, resistance formation becomes less likely. [30]
Furthermore, it overcomes methylation and efflux-mediated resistance. [28]
6. Superior Spectrum of Activity
As compared with older-generation macrolides and ketolides, nafithromycin demonstrates a broadened spectrum of activity. [31]
7. Significance of the Spectrum of Activity
The spectrum of activity of nafithromycin is highly suitable for respiratory infections. ¹
It is approved for CABP. [26]
Its spectrum avoids unnecessary disturbance to the normal flora but still treats the respiratory pathogens. [32]
8. Conclusion Regarding the Spectrum of Activity
Nafithromycin has broad coverage against Gram-positive bacteria, particularly those that are S. Pneumoniae resistant strains. [28]. It has good activity against atypical respiratory pathogens. [33]
Nafithromycin has moderate activity against selected Gram-negative respiratory bacteria. [32]
Activity is poor against other Gram-negative bacteria and Pseudomonas aeruginosa. [32]
1.6 CLINICAL INDICATIONS:
Indications of Nafithromycin in the Clinical Setting
The clinical indications for nafithromycin are mainly centered on the use of the medication in treating community-acquired bacterial pneumonia in adult patients [35].
This is because of the drug’s significant activity against some respiratory pathogens such as macrolide-resistant Streptococcus pneumoniae bacteria [36].
Therefore, it is indicated in the treatment of CABP cases that are mild or moderate and can be managed in outpatient clinics due to the oral administration route [37].
Furthermore, the medication is indicated for treating LRTIs caused by organisms such as Haemophilus influenzae and Moraxella catarrhalis [38].
Its high levels of penetration into the lungs and epithelial lining fluid are important for effective management of respiratory infections [36].
Furthermore, Nafithromycin can be used to treat atypical respiratory infections caused by bacteria like Chlamydia pneumoniae and Legionella pneumophila [38].
Hence, Nafithromycin serves as an excellent alternative when treating atypical pneumonia caused by β-lactam-resistant bacteria [36].
Nafithromycin is prescribed for MDR respiratory infections since it exhibits effectiveness against macrolide-resistant bacteria through its resistance-reversing properties [35].
Therefore, Nafithromycin is seen as a promising empirical antibiotic in areas with high levels of antimicrobial resistance [37].
Recent findings indicate that Nafithromycin could play a significant part in addressing inflammatory respiratory diseases resulting from infections due to its immunomodulatory effects [39].
Nevertheless, this area needs further investigation before it is considered clinically significant [37].
1.7 PHARMACODYNAMIC: -
Nafithromycin is a new lactone-ketolide antibiotic that kills bacteria that cause both typical and atypical respiratory infections.¹ It maintains efficacy against macrolide- and ketolide-resistant Streptococcus pneumoniae by circumventing Erm-mediated ribosomal methylation, efflux mechanisms, and ribosomal mutations.² The drug has very low minimum inhibitory concentrations (MIC₅₀ ≈ 0.014 mg/L; MIC₉₀ ≈ 0.06 mg/L) against S. pneumoniae , which shows that it is very powerful on its own.¹ Nafithromycin is said to be 2 to 8 times stronger than other macrolides like clarithromycin and telithromycin when it comes to resistant pneumococci.¹ It shows that it can kill a wide range of bacteria, such as Haemophilus influenzae , Moraxella catarrhalis , and Staphylococcus aureus that are sensitive to methicillin.¹
The drug has great intracellular activity against unusual respiratory pathogens like Legionella pneumophila, Mycoplasma pneumoniae, and Chlamydophila pneumoniae.
The AUC/MIC ratio is the best indicator of antibacterial activity because it is the best measure of pharmacodynamic efficacy. ³
AUC/MIC ratios for high epithelial lining fluid (ELF) show that the target site is highly visible and that the bacteria are killed. ³
Nafithromycin also has effects on the immune system that may help lower inflammation in respiratory tract infections. ⁴
Its pharmacodynamic characteristics facilitate short-course therapy (e.g., 3-day regimen) owing to increased drug exposure at infection sites. ⁵
1.8 PHARMACOKINETICS: -
Nafithromycin has good oral pharmacokinetics, meaning it is quickly absorbed and the amount of drug in the body is proportional to the dose. After being taken by mouth, the highest plasma concentrations (Cmax) range from about 0.099 to 2.987 mg/L, depending on the dose. The area under the concentration–time curve (AUC) goes up with the dose, from 0.54 to 43.46 h·mg/L.Eating food makes systemic exposure a little bit better, with the AUC going up by about 1.2 times when you are fed. [45]
Usually, steady-state concentrations are reached within 3 to 4 days of taking the drug once a day. [45]
Nafithromycin has a wide range of effects on lung tissues, which are where respiratory infections usually occurs. [44]
The amount of drugs in epithelial lining fluid is 2.5 to 37.9 times higher than in plasma. [42]
Concentrations in alveolar macrophages are significantly elevated (up to 2635-fold higher than plasma), facilitating activity against intracellular pathogens. [41]
The drug binds moderately well to plasma proteins (about 62–72%). [42]
Nafithromycin is mostly broken down by CYP3A enzymes, but it doesn’t stop CYP3A or CYP2D6 from working, which means it has a low risk of drug-drug interactions. [62]
Elimination happens through both the liver and the kidneys, and the clearance is balanced. [62]
The pharmacokinetic profile supports once-daily dosing and short-duration therapy due to sustained lung concentrations. [41]
1.9 PRE CLINICAL TRIAL DATA: -
1. In Vitro Antibacterial Activity
The unique ketolide structure of Nafithromycin confers potent activity on common respiratory pathogens Streptococcus pneumoniae, Haemophilus influenzae, and atypical agents like Mycoplasma pneumoniae and Chlamydophila pneumoniae. [46,47]
This agent is characterized by substantially lower MIC values for the aforementioned pathogens, especially those resistant to macrolide treatment. [47,48]
Furthermore, it is active against both erm- and mef-type resistance, allowing it to counteract methylation and efflux-driven resistance mechanisms. [48,49]
The bactericidal activity displayed by Nafithromycin during time-kill experiments differentiates it from macrolides, which have bacteriostatic potential. [47,50]
Also, it demonstrates antibacterial activity under acid conditions, showing promise in treating intracellular infections. [49,51]
2. Mechanism-based Preclinical Insights
Ribosome binding studies show that Nafithromycin has high affinity to domains II and V of 23S rRNA of 50S ribosomal subunit compared to macrolides like erythromycin. [48,52]
Structural changes in Nafithromycin contribute to sustained ribosome binding despite resistance to antibiotic action in some bacterial strains. [52,53]
This agent effectively inhibits protein synthesis due to dual site binding in comparison to conventional macrolides. [48,53]
3. In Vivo Efficacy Studies (Animal Models)
Nafithromycin demonstrated significantly better activity by reducing the bacterial burden in lung tissues infected with S. Pneumoniae in comparison to azithromycin. [47,54]
Dose-dependent reduction in CFUs was noted, with more efficacious activity seen at low doses as compared to other comparators. [64,53]
Furthermore, Nafithromycin showed good activity against pathogens in neutropenic mice models. [53,65]
It also demonstrated good survival rates in infected animals, thus showing promising activity in severely infected patients. [64,65]
4. Pharmacokinetic–Pharmacodynamic (PK/PD) Correlation
In preclinical studies on PK/PD analysis, Nafithromycin demonstrated good lung tissue penetration with higher concentrations than plasma. [24,54]
It also showed good PAE which contributes to its sustained antibacterial activity. [50,54]
AUC/MIC has been identified as the major PK/PD parameter responsible for driving efficacy in animal infection models. [54,55]
Good oral bioavailability in preclinical animal studies was noted. [24,55]
5. Safety and Toxicology Studies
Acute and repeated dosing toxicity studies on rodent and non-rodent species have shown that Nafithromycin has very good tolerability at therapeutic doses. [65,56]
Also, no cardiotoxicity or QT prolongation effects have been observed in safety pharmacology preclinical studies. [56,57]
There was no genotoxicity and mutagenicity seen in Ames test and micronuclei tests. [56,58]
Preclinical safety margins suggest there is a high therapeutic margin for continued drug development. [65,57]
6. Resistance Development Studies
Serial passage experiments revealed that nafithromycin is less likely than conventional macrolides to develop resistance. [49,59]
Mutational frequency experiments demonstrated that there would be a reduced chance of selecting resistance at clinically effective levels. [59,60]
There is efficacy against bacteria that have become resistant to other macrolides like erythromycin and azithromycin. [48,60]
Preclinical trials have indicated that Nafithromycin is an extremely potent next-generation ketolide with improved antibacterial properties and targeted delivery to the lungs. [47,54,57]
It is capable of overcoming resistance to macrolide drugs as well as having bactericidal effects in vitro and in vivo. [48,64,60]
1.10 CLINICAL TRIALS
Clinical trials carried out on nafithromycin were randomized double-blinded and placebo controlled using healthy adult volunteers to assess safety, tolerability, and pharmacokinetics. (PMCID 3834790)
Single dose escalating trials evaluated nafithromycin doses of 100 mg up to 1200 mg under fed and fasted conditions. (PMCID 3834790)
Multiple dose escalation studies used daily administration of 600 mg, 800 mg, and 1000 mg for 7 days under fed condition. (PMCID 3834790)
Tolerability was shown to be good at all doses without any reportable adverse event being observed. (PMCID 3834790)
Pharmacokinetic evaluation demonstrated that increasing doses led to increase in systemic absorption, with Cmax varying from 0.099 to 1.742 mg/L. (PMCID 3834790)
Area under the concentration-time profile (AUC0-t) was between 0.54 and 22.53 h•mg/L. (PMCID 3834790)
Diet was seen to affect drug bioavailability suggesting administration of nafithromycin under fed state for better results. (PMCID 3834790)
Phase II clinical trials investigated nafithromycin in patients with CABP to establish dosing optimization and preclinical efficacy. [61]
Safety, tolerance, pharmacokinetics, and clinical effectiveness were tested on infected patients. [61]
The results indicated significant improvement in CABP patients after treatment with nafithromycin within a brief time frame. [66]
Three days’ treatment with nafithromycin was found to be equally effective as other longer courses of antibiotics. [66]
Nafithromycin possessed excellent lung permeability, making it applicable in treating pulmonary diseases. [1]
Data from Phase II trials formed the foundation for further investigation of nafithromycin in Phase III trials. [1]
In a pivotal Phase III randomized, double-blind and controlled study, nafithromycin was tested in adults with CABP in several sites in India. [6]
Comparative effectiveness trial of oral nafithromycin 800 mg per day once for three days against oral moxifloxacin 400 mg per day once for seven days was undertaken. ([The Lancet] [7])
Trial patients comprised PORT classes of II, III, and IV corresponding to mild to moderate pneumonia. [6]
Primary end point of the study was Early Clinical Response (ECR) that is clinical improvement without clinical deterioration. [17]
Nafithromycin showed non-inferiority of its efficacy in relation to moxifloxacin in terms of clinical cure in CABP cases. [17]
3-day course oral therapy proved equally effective than the standard 7-days course therapy improving treatment compliance. [1]
Beneficial effect was seen particularly in older and sicker subjects with advanced stage disease (PORT III/IV). [66]
Drug was well tolerated by the subjects in terms of side-effects without significant safety issues. [66]
One of the early success stories of this kind in short-course treatment regimen for CABP. ([PMC] [4])
It was conducted with the assistance of Biotechnology Industry Research Assistance Council in India. [63]
Approval was attained for the use of nafithromycin in the management of adult CABP based on results of Phase III trials. [63]
Nafithromycin proved to be efficacious in combating both common and uncommon respiratory infections through clinical trial studies. [8]
The short course treatment schedule makes this drug more efficient in increasing compliance and preventing development of resistance. [1]
Its effective lung tissue penetration is a contributing factor to its clinical effectiveness. [1]
CONCLUSION:
The representation of Nafithromycin stands as a remarkable step in the realm of antimicrobial drugs, especially during the era where antibiotic resistance is becoming increasingly prevalent. With a novel molecular structure and unique pharmacological mechanism, the next-generation ketolide can surpass several factors that render conventional macrolide antibiotics ineffective due to their resistance against different pathogens.
Pharmacologically, the next-generation ketolide drug displays good oral bioavailability, excellent tissue distribution, and increased biological stability, which facilitate easier administration and better adherence in patients. Moreover, the pharmacodynamics of the agent shows that the drug exhibits strong, concentration-dependent antibacterial action against the organisms causing infection.
Efficacy, safety, and tolerability studies conducted to date demonstrate the promising role of the agent as an antibiotic in the treatment of community-acquired infections. In particular, community-acquired bacterial pneumonia is shown to be successfully treated using the new medication. Favourable drug interaction and tolerability properties further increase the potential value of the drug as an antimicrobial medication. It is important to note that the drug is a product of pharmaceutical innovation within the country.
In conclusion, Nafithromycin is one such treatment that holds promise in addressing the deficiencies associated with existing antimicrobial therapies. Nevertheless, vigilance will be needed to ensure that Nafithromycin remains efficacious and does not lose its utility as a result of resistance developing too quickly. Similar to a key used for locking away hard-to-reach items, Nafithromycin might not resolve all antimicrobial concerns but it can certainly open locked doors.
REFERENCES

K. H. Makhija*, N. S. Jadhav, P. S. Jadhav, N. R. Pathan, Nafithromycin: India’s First Indigenously Developed Ketolide Antibiotic for Drug-Resistant Respiratory Infections, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 5, 7597-7611. https://doi.org/10.5281/zenodo.20424117
 10.5281/zenodo.20424117
10.5281/zenodo.20424117