
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Krishna School Of Pharmacy & Research, Drs. Kiran & Pallavi Patel Global University, Varnama, Vadodara, 391240.
Coronary Microvascular Angina (CMVA) is a chest pain which is caused by a blockage in the heart’s small blood vessels, even when the larger vessels are clear. In past times, it was referred as “Cardiac Syndrome X”. This condition is most common in women, particularly after menopause, and is sometimes ignored considering as stress-related disease. The main problem is insufficient relaxation and unusual constriction of these vessels, as well as autonomic instability, oxidative stress, endothelial dysfunction and swelling. Cardiometabolic parameters such as high blood pressure, insulin resistance, and low estrogen might worsen symptoms. Standard angiograms usually appear normal, making hard to diagnose. While biomarkers for oxidative stress and inflammation are being identified, advanced instruments such as, cardiac MRI, PET scans and AIbased imaging are now used to estimate microvascular blood flow. Using drugs such as ACE inhibitors, ?-blockers, statins, and sometimes endothelin receptor blockers. The main aim of the treatment is to improve vessel health and decreases the effect symptoms. To decrease wrong diagnosis and improve outcomes for this disease, researches are going on to increase the diagnostic standards and to improve health
Microvascular angina, also known as cardiac syndrome X, refers to as a situation where a person experiences chest pain despite normal coronary arteries as viewed during angiography. There are symptoms of decreased coronary blood flow, like ECG changes associated with exercise or stress testing, present in this case [1]. Coronary microvascular dysfunction (CMD) is the major pathophysiological theory, in spite of angiographically normal large-vessel anatomy, it is caused by small-vessel endothelial dysfunction and poor vascular reactivity [2]. Autonomic instability, increased pain perception and chronic systemic inflammation, are other contributing factors [3].
HISTORICAL BACKGROUND
This syndrome was first described in 1967 by Likoff and a group of women who had normal coronary angiograms, ischemia ECG alterations during exercise, and chest discomfort [4]. Harvey Kemp had given the term "Syndrome X" in 1973 to describe this illness, which is categorized by angina symptoms with normal angiography and unknown causes [5]. The word "microvascular angina" was first used in the 1980s by researchers named Cannon and Epstein, which mainly focused on endothelial dysfunction and reduced coronary flow reserve in small arteries even in the absence of epicardial blockage [6]. In the following decades the knowledge changed from assigning symptoms to benign causes such as anxiety or dyspepsia to realize that myocardial ischemia was caused by microvascular disease [7].
PREVALENCE / EPIDEMIOLOGY
Up to 49% of patients having angiography for suspected ischemia show no obstructive CAD, and among these, up to 60–64% exhibit signs of CMD consistent with MVA, according to observational cohort studies [8]. The prevalence of CMD was shown to be roughly 51–54% in a large PET-based investigation with over 1,200 participants, with equal rates for males (51%) and women (54%) [9]. According to other CCD (coronary reactivity) based cohorts, the prevalence was
63% in mixed-gender groups without obstructive lesions and 47% in women [10]. Together, these findings imply that microvascular dysfunction may be the cause of symptoms in approximately 50% of ischemia patients without macrovascular illness [11].
RISK FACTORS
A significant risk factor is female sex: around 60–70% of cardiac syndrome X or MVA cohorts are female, and among patients assessed for angina with normal coronaries, 41% of women and 8% of men showed non-obstructive illness, which is consistent with MVA [12]. Macrovascular disease and cardiovascular risk factors are similar: individuals with MVA often have high blood pressure, high cholesterol, smoking, insulin resistance, obesity, and estrogen shortage (e.g., postmenopausal condition) [13]. Insulin resistance and metabolic syndrome are especially closely related. MVA was linked to metabolic syndrome characteristics as insulin resistance, dyslipidemia, and hypertension in 14% of a cohort of 500 patients having angiography who had symptoms and normal angiograms (mostly perimenopausal women) [14]. Endothelial dysfunction has been linked to symptoms in Syndrome X/MVA patients, as evidenced by elevated plasma endothelin-1 and decreased nitric oxide bioavailability [15].
ETIOLOGY OF MICROVASCULAR ANGINA PECTORIS
The underlying cause of MVA, coronary microvascular dysfunction (CMD), is caused by a combination of anatomical and functional disease in the small coronary resistance channels (<300 µm), which results in angina and poor perfusion even in the presence of patent epicardial arteries
[16].
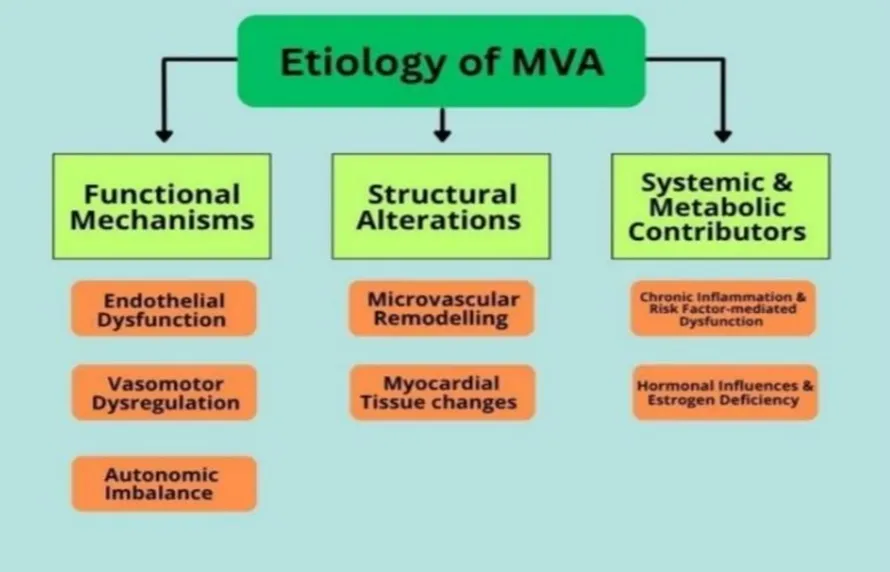
(Figure 1)
CLINICAL MANIFESTATIONS
Similar symptoms to angina pectoris, coronary artery disease, etc., may be present in patients with microvascular angina [17]. These patients frequently have effort-induced retrosternal compressive chest discomfort and/or dyspnea, although symptoms can also occasionally manifest at rest, at night, or after exercise [18]. It is noteworthy that this illness is more common in women than in males, particularly after menopause [19]. Conversely, men are more likely to have atypical signs of this illness [20].
PATHOPHYSIOLOGY OF MVA
Numerous factors influence the pathophysiology of MVA. The pathophysiology of MVA frequently involves impaired vasodilation response, either through endothelium- dependent or endothelium-independent mechanisms [21]. Endothelial dysfunction in MVA patients may also be caused by a vasodilator-vasoconstrictor imbalance, which is represented by decreased nitric oxide (NO) release and elevated plasma levels of endothelin-1 [22,23,24,25]. An imbalance between endothelium-derived constrictors like endothelin and relaxing agents like nitric oxide (NO) results in endothelium-dependent dysfunction. Myocyte tone is the basis for endothelium-independent function. Furthermore, obstructive epicardial coronary artery disease may or may not be present when CMD develops [26]. Risk factors for its development include smoking, diabetes mellitus, high blood pressure, high cholesterol, and insulin resistance [27]. The pathogenic role of estrogen deprivation in the development of endothelial dysfunction has also been highlighted by the high prevalence of MVA in menopausal women [28].
DIAGNOSTIC CHALLENGES
In order to categorize coronary microvascular dysfunction (CMD) more accurately, Camici and associates developed a clinical paradigm back in 2007. Based on underlying factors, this method classified CMD into four primary types:
1. CMD without structural heart or artery disease: Patients who have CMD symptoms without obvious coronary artery disease or myocardial pathology fall into this category.
2. CMD linked with myocardial disease: Patients with aortic valve stenosis, hypertrophic or dilated cardiomyopathy, chronic hypertension, or infiltrative diseases such as amyloidosis fall under this category.
3. CMD with obstructive coronary artery disease (CAD): In these situations, CMD coexists with acute coronary syndromes or stable CAD, making diagnosis and therapy more challenging.
4. Iatrogenic CMD: When tiny emboli block the distal microvasculature during coronary recanalization treatments, this type of CMD may develop a side consequence [29]. The significance of both invasive and non-invasive testing was acknowledged in revised guidelines published in 2021 by a joint task team comprising the AHA, ACC, ASE, CHEST, SAEM, SCCT, and SCMR. They approved a class 2A recommendation for the evaluation of patients with persistent, stable chest discomfort in spite of non-obstructive coronary results using either invasive coronary function testing or non-invasive imaging, such as PET or stress cardiac MRI [30].
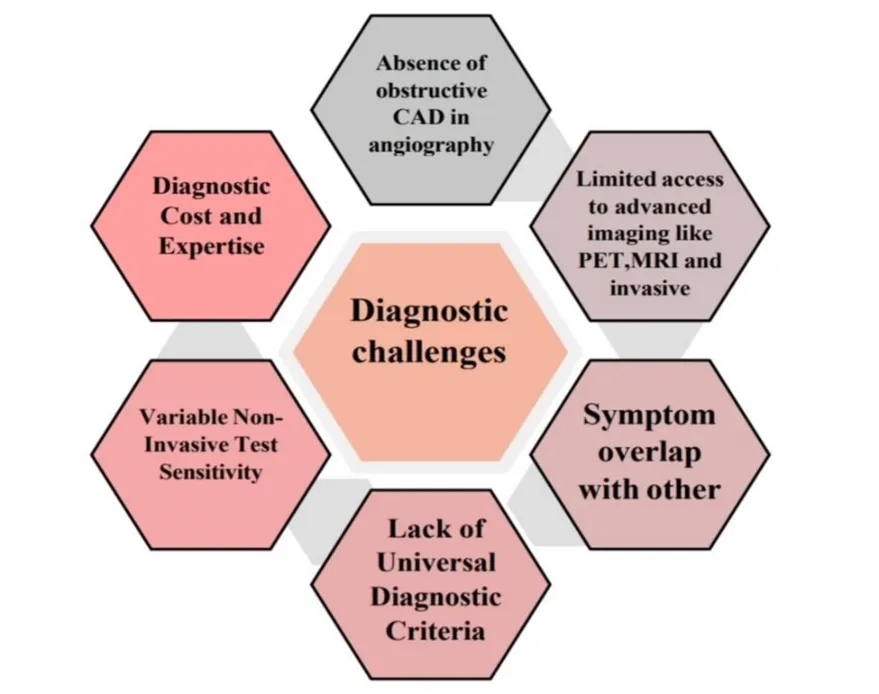
(Figure 2)
NOVEL DIAGNOSIS APPROACHES
1. Invasive Techniques
The smaller vessels in the coronary microcirculation cannot be detected immediately with angiography, in contrast to the big coronary arteries [31]. The only diagnostic technique that can fully assess all endotypes of ischemia with nonobstructive coronary arteries (INOCA) is invasive coronary vasomotor function testing (CFT) [32]. According to studies, people with microvascular angina (MVA) may benefit from invasive procedures to lessen their symptoms [33]. Although an endomyocardial biopsy can theoretically view small coronary vessels, this procedure is highly invasive and does not provide information about the functioning of these veins. Rather, a number of measurement-based techniques are employed to evaluate the flow of blood through these micro arteries and ascertain the effectiveness of the microcirculation [34,35].
(Table 1)
|
Sr. No. |
Invasive Methods |
Process |
Benefit |
|
1. |
Coronary Flow Reserve (CFR) Management |
Intracoronary Doppler flow wire or thermodilution technique during coronary angiography |
Assesses the capacity of coronary circulation to increase blood flow in response to stress |
|
2. |
Index of Microcirculatory Resistance (IMR) |
Uses a pressuretemperature sensor wire and thermodilution during adenosineinduced hyperemia |
Delivers a quantitative and reproducible measure of microvascular resistance independent of epicardial stenosis |
|
3. |
Acetylcholine Provocation Testing |
Intracoronary acetylcholine infusion during angiography to assess endothelialdependent microvascular reactivity |
Identifies microvascular spasm as a mechanism of angina in the absence of epicardial spasm |
Coronary Flow Reserve (CFR) Measurement
The blood flow of coronary arteries is dynamic, continually changing to satisfy the heart’s oxygen needs. Coronary Flow Reserve (CFR), a crucial physiological indicator, measures the heart’s capacity to augment this flow under stress [42]. Both invasive and non-invasive methods can be used to evaluate this. A doppler wire is inserted into a coronary artery during an invasive CFR test. The speed of blood flow is reflected in changes in the frequency of the sound waves that are emitted by the wire and reflect off red blood cells [36]. CFR is determined by dividing the blood flow velocity at rest by the blood flow velocity during stress (hyperemia). CFR is calculated inversely from the time it takes a saline solution to pass through the vessel. Resting and hyperemic durations are then compared.
Heart attacks, Heart failure, Strokes, and even death are among the major cardiovascular events that are associated with a lower CFR. A CFR value of less than 2.0 is deemed abnormal by the European society of cardiology [37,38,39].
Index of Microcirculatory Resistance (IMR)
IMR is a contemporary diagnostic metric that evaluates the coronary microvasculature's resistance. In order to assess pressure and flow during stress, which is typically brought on by adenosine, a specific guidewire must be inserted into the coronary artery. IMR is determined by multiplying the time it takes for a cold saline bolus to travel through the artery during hyperemia by the distal coronary pressure (Pd) [40]. The outcome shows the degree of resistance in the microvascular network. It is suggested that CMD is present if the IMR value is higher than 25 [41].
2. Non-invasive Techniques
Invasive methods are not necessarily necessary for the detection of coronary microvascular dysfunction (CMD). Thanks to developments in medical imaging, physicians may now rule out significant artery blockages using non-invasive techniques like CT coronary angiography. Certain stress tests can help identify CMD symptoms even when major arteries have been shown to be clear. It's crucial to keep in mind, nevertheless, that a normal stress test result does not always indicate the absence of CMD [42].
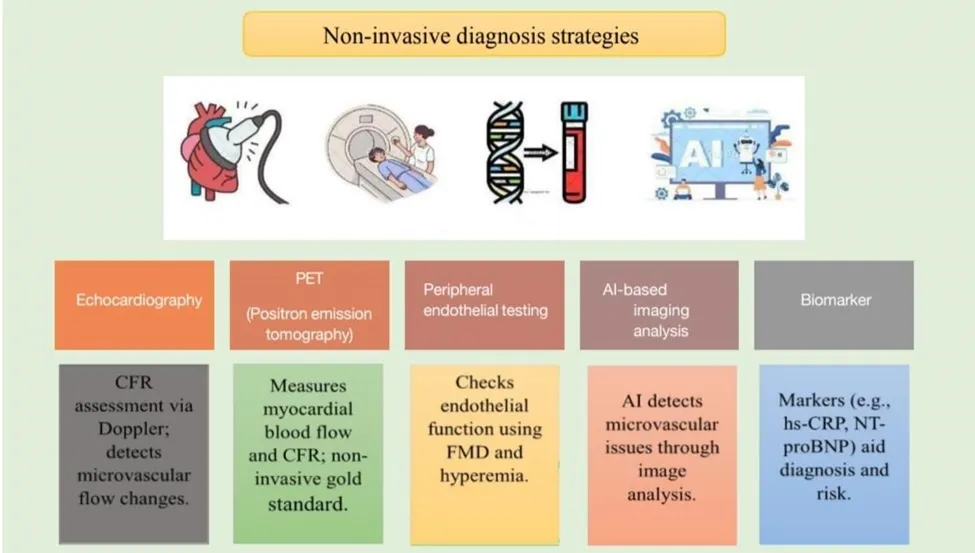
(Figure 3)
Whether or not a person has blockages in the main coronary arteries, CMD can still happen. However, when obstructive coronary artery disease (CAD) is not present, studying CMD is frequently simpler. This is due to the fact that when blockages are present, it becomes challenging to determine whether the blockage or CMD is the reason of the decreased blood flow. Doctors can confidently associate CMD with decreased blood flow or aberrant coronary flow reserve (CFR) by using CT angiography to rule out obstructive CAD.
Cardiac PET (Positron Emission Tomography) is the most accurate and dependable imaging modality for identifying CMD [43].
Echocardiography
One study examined 70 individuals, 44 of whom were female, who had chest pain but no coronary artery blockages. These patients underwent a number of procedures, including stress echocardiography, radionuclide scans, treadmill stress testing, and thallium imaging. Surprisingly, the researchers discovered that the results varied between tests. While some tests revealed anomalies in the heart muscle or symptoms of ischemia, others did not. There were no obvious problems with heart wall motion, despite the patients' chest discomfort and ECG abnormalities. This demonstrates how difficult it is to diagnose CMD [44]. During a routine echocardiography scan, physicians examine the flow in the left anterior descending (LAD) artery using color Doppler imaging.
A modified image that displays the LAD going along the front of the heart is typically used to do this [45].
PET (Peripheral Endothelial Testing)
PET scans are advanced method of detecting the cardiac muscle's blood flow. Doctors can monitor blood flow and obtain specific measures by using specialized tracers. This tracer includes 13N-ammonia, 82Rb-rubidium, 18F-flurpiridaz, and 15O-water which enables accurate monitoring of blood flow in different cardiac regions [46]. Using drugs like adenosine or dobutamine to mimic exercise, the scan may assess blood flow both at rest and under stress. This aids physicians in determining CFR, a crucial metric for diagnosing CMD. PET is a great option for this type of diagnostic since it can provide precise, realtime data [47,48,49]. The blood vessel problems in CMD patients are not limited to the heart. Studies show that people with CMD also tend to have stiffer arteries throughout their body. This is usually measured by checking pulse wave velocity (PWV), which tells us how fast blood moves through the vessels. Higher PWV means stiffer arteries. CMD patients usually show higher PWV and less ability for their arteries to relax properly, which is called endothelium dependent vasodilation. These findings have been repeated in many studies, confirming that CMD affects more than just the heart’s tiny vessels [50,51].
AI Based Imaging Analysis
In order to identify subtle functional and anatomical patterns linked to coronary microvascular dysfunction (CMD), which underlies microvascular angina (MVA), artificial intelligence (AI) and deep learning (DL) are increasingly being used in cardiac imaging modalities, particularly PET, CMR, and cardiac CT [52]. AI systems can automatically identify microvascular ischemia by extracting and integrating quantitative data from imaging investigations, such as cardiac perfusion maps or flow reserve metrics. DL-based analysis demonstrated better ischemia identification than conventional perfusion indices in a registry of more than 1,600 patients without known CAD undergoing stress myocardial perfusion imaging (MPI) (AUC 0.80 versus 0.78; p < 0.01) [53]. Even when epicardial arteries seem normal, these methods enable the diagnosis of non-obstructive but functionally important CMD.
Biomarkers
1. Circulating protein biomarkers: Inflammation, Endothelial & Coagulation Markers A group of inflammatory and endothelial biomarkers, such as TNF-α, IL-6, CRP, and sCD40L, were substantially correlated with CMD, which is defined as reduced coronary flow velocity reserve (CFVR < 2.0), in women with angina but no obstructive CAD. These grouped biomarkers significantly indicated compromised microvascular function, according to principal component analysis [54]. Four vascular biomarkers von Willebrand factor (vWF), GDF-15, tissue-type plasminogen activator (tPA), and Galectin-4 were substantially linked with poor microvascular dilatation in a proteomic investigation of 97 women with CMD evaluated by rubidium-82 PET (MBFR < 2.5)
[55].
2. Oxidative Stress Biomarkers
As CMD patients have lower antioxidant capacity than controls, oxidative stress indicators such decreased glutathione have been demonstrated in invasive CMD examinations to independently predict impaired coronary vascular reactivity [56].
3. Metabolic-Profiling & Machine Learning Signatures
Using multi-omics and machine learning, plasma metabolite profiling of postmenopausal women revealed particular chemical signatures that distinguish CMD patients from controls, providing proof-of-concept for non-invasive metabolic biomarkers in CMD identification [56].
4. Multi-Mechanism Biomarker Reviews
Endothelial dysfunction, vascular inflammation, and oxidative stress are the three primary domains into which a recent narrative review divides biomarkers for CMD/MVA, highlighting their advantages and disadvantages for clinical application as non-invasive diagnostic tools [58].
MANAGEMENT OF MVA
Intravascular ultrasonography studies have shown that most MVA patients do have some degree of concurrent coronary atherosclerosis [59]. Therefore, for the majority of patients, total control over heavy smoking, hypertension, hyperlipidemia, diabetes, lifestyle modifications, and obesity is recommended in order to lower risk factors. Additionally, the guidelines suggested that the mechanism or pathway failure causing MVA be addressed as part of the treatment. β-blockers, angiotensin-converting enzyme inhibitors (ACE-I), statins, lifestyle modifications, and weight loss are recommended for individuals with anomalous CFR <2.0 or IMR ≥25 units and a negative cholinergic provocation test. Similar to vasospastic angina, microvascular spasm can also be treated [60]. The primary objective of pharmacologic therapies for MVA patients is to manage symptoms and enhance their quality of life. The most often prescribed medications for MVA patients include beta-blockers, nitrates, statins, calcium channel blockers, and angiotensinconverting enzyme inhibitors. Myocardial perfusion and angina are known to be improved by these substances.
Agents used in MVA
Statins
Beyond their potential to decrease cholesterol by blocking 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase, statins have been shown to improve endothelial function by boosting NO bioavailability, having antioxidant qualities, and reducing inflammatory responses [61]. Statins have strong anti-inflammatory effects in addition to their ability to decrease cholesterol [62]. Additionally, a 2011 systematic review demonstrated that statin medication significantly improved peripheral and coronary endothelial function, underscoring its potential application in MVA [63]. Treatment with statins was linked to a significant improvement in endothelial function with a standardized mean difference of 0.66 (95% CI [0.46–0.85]; p<0.001), according to a recent systematic review and meta-analysis of randomized controlled trials evaluating the impact of statins on coronary and peripheral endothelial function [64].
Beta-blockers
β-Blockers are first-line treatment for patients with symptomatic CMD particularly when heart rate is raised because they increase diastolic perfusion time and decrease myocardial oxygen demand [65]. Some studies shows that atenolol and propranolol decreases anginal episodes in people with normal coronary arteries when compared to calcium channel blockers or nitrates [66]. Thirdgeneration β-blockers like carvedilol and nebivolol, improve nitric oxide bioavailability and coronary flow reserve (CFR) in ways that go beyond simply lowering heart rate [67].
ACE inhibitors
In patients with CMD, ACE medications such as quinapril and enalapril have been used to enhance endothelial-mediated vasomotor responses and CFR, including reversing microvascular remodeling in hypertensive persons [68]. Clinical research and meta- analyses also indicate that ACE inhibitor along with statin therapy improves capacity and quality of life in individuals with microvascular angina [69].
FUTURE PERSPECTIVE AND RESEARCH DIRECTION
Combination of invasive and non-invasive tests, such as coronary flow reserve (CFR), index of microcirculatory resistance (IMR), cardiac MRI, and PET, with AI-driven multimodal analytics improves detection accuracy and risk, further CMVA research is done for advance precision diagnosis and treatment [70]. In order to find new molecular targets, mechanistic research is dissecting structural and functional pathology, including endothelial dysfunction, remodeling, oxidative stress, inflammation, metabolic syndrome interaction, and vasomotion disorders including microvascular spasm [71]. Pharmacologic therapies employing drugs like ACE inhibitors, statins, ranolazine, and endothelin receptor antagonists are being driven by phenotype-guided precision medicine, as demonstrated by CorMicA stratified therapy and ongoing trials targeting
CMD subgroups [72]. In order to increase results in CMVA populations, research will focus on high-quality RCTs, standardized INOCA/MVA diagnostic criteria, biomarker identification for early screening and monitoring, and integrated multi-target therapy approaches [73].
CONCLUSION
Coronary microvascular angina represents the paradigm shift in the area of cardiology that shows the complexity of ischemic heart disease. The technologically advanced diagnostics and therapeutic options have showed hope to the sufferers as the understanding of the mechanisms has improved. The integration of molecular analysis and invasive studies into the prediction algorithms for artificial intelligence suggests an era when CMVA would not only be well treated but possibly prevented.
REFERENCES
10.3389/fcvm.2022.800918
CorMicA trial. J Am Coll Cardiol. 2018;72(23 Pt A):2841–2855do10.1016/j.jacc.2018.09.006. PMID: 30392770.
Taqueti VR, Di Carli MF. Coronary Microvascular Disease Pathogenic Mechanisms and Therapeutic Options: JACC State-of-the-Art Review. J Am Coll Cardiol. 2018;72(21):2625–2641. doi: 10.1016/j.jacc.2018.09.042.PMID:3049610
10.3389/fcvm.2022.800918
CorMicA trial. J Am Coll Cardiol. 2018;72(23 Pt A):2841–2855do10.1016/j.jacc.2018.09.006. PMID: 30392770.

Neha Singh, Vishva Patel, Krinal Patel, Srusti Mistry, Vandan Patel, Review on - Analytical Novel Diagnostic and Management Strategies in Coronary Microvascular Angina Pectoris, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 3906-3920, https://doi.org/10.5281/zenodo.20716062
 10.5281/zenodo.20716062
10.5281/zenodo.20716062