
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Nandkumar Shinde College of Pharmacy, Vaijapur, Chh. Sambhajinagar, MS, India.
Transdermal drug delivery devices are used for administering medications topically. These are different-sized pharmacological preparations with one or more active components that are meant to be applied to intact skin to deliver the active ingredient after it has passed through the skin's barriers. They do not include first-pass metabolism. Approximately seventy-four percent of medications taken orally nowadays do not work as intended. A transdermal drug delivery device was developed to increase efficacy. The regulated release of medication into the patient's system is a significant benefit of transdermal drug delivery when compared to other techniques such as oral, topical, intravenous (IV), and intramuscular (IM) administration. This regulated release is accomplished either by employing a porous membrane that surrounds a reservoir of medication.
Transdermal delivery systems are topically administered medicament in the form of patches that deliver drugs for systemic effects at a predetermined and controlled rate. Transdermal Drug Delivery Systems (TDDS), or "patches," deliver drugs through the skin, bypassing first-pass metabolism and ensuring controlled, sustained release. They enhance patient compliance and minimize side effects by maintaining steady plasma drug levels. TDDS is effective for drugs with short half-lives and offers continuous therapeutic effects. The first FDA-approved system, Transdermal-SCOP, was launched in 1979 for motion sickness. TDDS is part of a broader category of advanced drug delivery methods, including controlled release and transmucosal systems. Transdermal Drug Delivery Systems (TDDS) involve delivering drugs through the skin for systemic effects, offering several advantages over traditional methods. With over twenty FDA-approved transdermal drugs, TDDS provide sustained, controlled drug release and easy cessation by simply removing the patch. This method bypasses the gastrointestinal tract and hepatic first-pass metabolism, improving drug bioavailability. A Transdermal Drug Delivery System (TDDS) is an innovative approach to drug administration that allows active pharmaceutical ingredients to be absorbed through the skin and into the bloodstream, bypassing the digestive system and the liver’s first-pass metabolism. This system offers an alternative to traditional drug delivery methods such as oral tablets, capsules, or injections. TDDS provides a controlled and sustained release of drugs over an extended period, which helps maintain steady drug concentrations in the blood, thus improving therapeutic outcomes while minimizing fluctuations in drug levels that can lead to side effects or toxicity. One of the main advantages of TDDS is its ability to provide continuous and controlled drug release. This controlled delivery allows for more consistent therapeutic effects, which is particularly beneficial for chronic conditions that require long-term medication. Furthermore, because TDDS bypasses the gastrointestinal (GI) tract, it avoids the digestive issues and potential instability associated with some oral medications, such as drug degradation in stomach acid. This route also circumvents first-pass metabolism in the liver, which can degrade drugs and reduce their bioavailability when taken orally. The structure of a typical TDDS involves several layers, each with a specific function. The backing layer provides protection to the drug and prevents it from evaporating, while the drug reservoir or matrix contains the active ingredient that is to be delivered. The adhesive layer ensures the patch remains attached to the skin, and the release liner protects the patch until it is ready for use. Together, these layers form a system that controls the rate at which the drug is released and absorbed by the skin. However, for TDDS to be effective, the drug must be able to penetrate the skin’s outermost layer, the stratum corneum, which serves as a barrier to many substances. To facilitate this, transdermal patches often incorporate enetration enhancers, such as surfactants or alcohols, which temporarily disrupt the skin barrier to allow the drug to pass through more easily. Additionally, the drug must have the right physicochemical properties—such as suitable molecular size, lipophilicity, and a moderate rate of absorption—so that it can diffuse through the skin and enter the bloodstream efficiently. Transdermal drug delivery is widely used in the treatment of chronic conditions that require long-term medication. For example, hormonal therapies like estradiol patches for hormone replacement therapy (HRT) in postmenopausal women, and nicotine patches for smoking cessation, are commonly used. Other examples include fentanyl patches for chronic pain management and scopolamine patches for the prevention of motion sickness or nausea related to chemotherapy. The ability to deliver medication continuously over hours or even days means that patients can often achieve better compliance with treatment regimens, as they need not remember to take medication multiple times a day. Despite its many advantages, there are limitations to TDDS. For instance, not all drugs are suitable for transdermal delivery. Large molecules, highly charged drugs, or those that are poorly soluble in fat (lipophobic) may not be absorbed effectively through the skin. Additionally, some patients may experience skin irritation or allergic reactions to the adhesives or other components of the patch, limiting its use for certain individuals. Furthermore, the onset of action for transdermal drugs is typically slower compared to oral or injectable medications, as the drug must first be absorbed through the skin before entering the bloodstream and reaching its site of action. In recent years, advances in transdermal drug delivery technologies have led to the development of microneedles, which are tiny needles that painlessly puncture the skinsurface to deliver drugs more effectively. Other technologies, such as iontophoresis (using electrical currents to drive charged drug molecules into the skin) and ultrasound-mediated delivery, are also being explored to enhance drug penetration and expand the range of drugs that can be delivered transdermally. In conclusion, Transdermal Drug Delivery Systems provide a valuable alternative to traditional methods of drug administration. They offer controlled, sustained release of medication, bypass first-pass metabolism, and improve patient compliance, especially for chronic conditions. However, their success is highly dependent on the drug’s characteristics and the ability of the system to overcome the skin’s natural barrier. Ongoing research in skin penetration technologies promises to broaden the scope of transdermal drug delivery and improve its effectiveness.
The route is unsuitable when –
The basic structure of a TDDS includes several critical components:
Contains the active pharmaceutical ingredient (API).
Regulates the release of the drug from the reservoir.
Ensures the patch stays attached to the skin, providing consistent drug delivery.
Protects the patch and prevents contamination or evaporation of the drug.
Transdermal systems are used for various therapeutic areas, including:
Patches like fentanyl or lidocaine provide controlled-release analgesia for chronic pain.
Estrogen and testosterone patches help in hormone replacement therapy (HRT).
Nicotine patches are commonly used in smoking cessation programs to provide steady nicotine delivery.
Nitro glycerine and clonidine patches are used to manage conditions like angina and hypertension.
Advantages of Transdermal Drug Delivery:
Transdermal drug delivery systems (TDDS) offer several advantages, making them an attractive option for administering medications. Here are the key benefits:
Ease of Use: TDDS are typically applied as patches, which are easy for patients to use without the need for injections, pills, or liquids.
Non-invasive: Since they do not require needles, they are more appealing for patients who are averse to injections or oral medications.
Convenience: Patches can be worn discreetly and typically need to be changed only once a day or even less frequently, reducing the need for frequent doses.
Sustained Release: TDDS provide a controlled, steady release of the drug over time, which can help maintain consistent drug levels in the bloodstream, reducing the peaks and troughs seen with oral or injectable forms.
Reduced Side Effects: The controlled release can minimize side effects that result from high concentrations of the drug, improving safety.
Avoids First-Pass Metabolism: Unlike oral medications, which are metabolized in the liver before reaching systemic circulation, transdermal drugs are absorbed directly into the bloodstream, bypassing the gastrointestinal (GI) tract and liver. This can increase the bioavailability of the drug.
No Need for Digestive Processing: This is particularly beneficial for drugs that may be broken down or poorly absorbed in the GI tract.
Localized Effect: Some TDDS can be designed to target specific areas of the body, providing localized drug action while minimizing systemic side effects.
Reduced Systemic Exposure: By targeting drug release directly to where it's needed, transdermal patches can limit the distribution of the drug to other parts of the body, reducing the risk of side effects in organs like the liver or kidneys.
Pain-Free: Transdermal systems do not cause the pain associated with injections, making them more suitable for long-term use, particularly in chronic conditions.
No Need for Frequent Medical Visits: For drugs that require regular administration (like hormone therapy or pain management), TDDS eliminate the need for hospital or clinic visits for injections.
Chronic Condition Management: TDDS are particularly useful in the treatment of chronic diseases such as hypertension, diabetes, or pain management, as they can provide a long-term therapeutic effect without the need for frequent dosing.
Avoids GI Irritation: Some oral medications can cause irritation in the stomach or intestines, leading to discomfort or nausea. TDDS avoid this issue entirely by bypassing the digestive system.
Some drugs that cannot be effectively administered orally due to poor absorption or degradation in the GI tract can be delivered transdermally, increasing their therapeutic potential.
Elderly or Disabled Patients: Transdermal patches can be an ideal option for patients who have difficulty swallowing pills or those who may forget to take medications.
Children: TDDS can also be more appropriate for pediatric patients who might have difficulty with traditional drug forms.
10. Potential for a Broad Range of Drugs
TDDS can be formulated for a variety of drug types, including analgesics, hormones, nicotine, antiemetics, and more, offering a versatile platform for drug delivery. These advantages make transdermal systems an effective and patient-friendly alternative for certain medications. However, their application is not suitable for all drugs, as factors like drug size, molecular weight, and skin permeability can limit the effectiveness of the system.
Disadvantages of transdermal drug delivery:
Transdermal Drug Delivery Systems (TDDS) offer several benefits, such as convenience and controlled drug release, but they also have certain disadvantages. Here are 10 disadvantages of TDDS:
Only certain drugs with appropriate molecular size, solubility, and skin permeability can be delivered effectively via TDDS. Larger or hydrophilic molecules may not penetrate the skin well.
Some individuals may experience local skin irritation, redness, or allergic reactions at the application site due to adhesives or other components in the patch.
TDDS typically provides a slow onset of action compared to oral or intravenous drug delivery, which can be problematic for drugs requiring immediate therapeutic effects.
Skin characteristics vary by individual and body site, which can lead to inconsistent drug absorption. Factors like age, hydration, and skin condition can affect permeability.
If the patch is not removed at the appropriate time, there’s a risk of drug accumulation and overdose, as some patches are designed to release the drug gradually over a long period.
TDDS has a limited capacity for holding a large quantity of the drug, which can restrict its use for drugs that require higher doses.
Patches may become displaced due to sweating, movement, or improper application, potentially leading to reduced drug delivery and therapeutic failure.
The production and development of transdermal patches can be expensive, making them more costly than traditional forms of drug delivery (e.g., tablets, injections).
Adhesives used in patches may not adhere well to all skin types, causing the patch to peel off prematurely or not stick at all.
If a patch is applied over broken or irritated skin, or in combination with other topical products, there may be interactions that affect drug absorption and therapeutic efficacy. These challenges highlight some limitations in the use of TDDS, although advances in technology continue to improve their effectiveness and applicability.
Anatomy and physiology of skin:
Skin: The Largest Organ
The skin, constituting the largest organ of the human body, spans approximately 2 square meters and receives nearly one-third of the body's blood circulation. It acts as a protective barrier against the transdermal absorption of diverse chemical and biological agents, with a thickness ranging from a few ml (2.97-0.28mm).
This organ:
The skin significantly influences various aspects of drug delivery, including drug permeation and absorption across the dermis. The skin's diffusional resistance relies heavily on its anatomy and ultrastructure. Functioning as a dynamic organ, the skin facilitates the migration of substances through and across its layers. the primary function of the skin is to provide protection against physical assaults and pathogens. This attribute contributes to the skin's toughness and rigidity, which can pose challenges for drugs administered via the transdermal route.
Anatomy of skin:
The human skin structure comprises three layers:
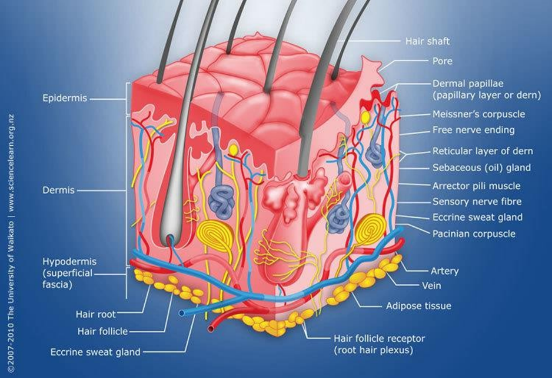
Fig. Human Skin
Epidermis:
The epidermis is a stratified, squamous, keratinizing epithelium. The complex layer of epidermis varies ingredient upon cell size, thickness and number of cell layers of epidermis which are going from 0.8 mm on palms and soles down to 0.06 mm on the eyelids. About 90% epidermal cells are keratinocytes or chest rated in five layers and creates keratin protein and 8% melanocytes are available. They create dark shade that adds to skin shading and ingests harming UV light.
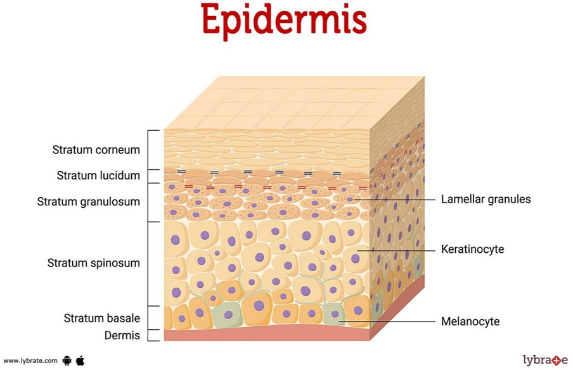
Fig. Epidermis
Dermis:
Dermis is 3 to 5 mm thick layer and is made out of a lattice of connective tissue, which contains veins, lymph vessels and nerves. The cutaneous blood supply has basic capacity in direction of body temperature. It additionally gives supplements and oxygen to the skin while removing toxins and squander items. Vessels reach to inside 0.2 mm of skin surface and give sink conditions to most atoms entering the skin hindrance. The blood supply in this manner keeps the dermal centralization of a saturate low and the subsequent contrast over the epidermis gives fundamental focus inclination to transdermal penetration.
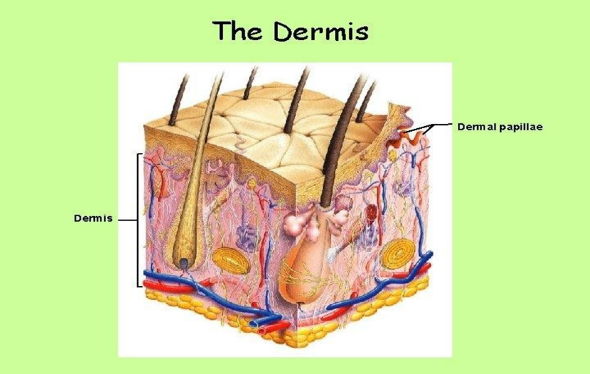
Fig. Dermis
Hypodermis:
The hypodermis or subcutaneous fat tissue underpins the dermis and epidermis. It fills in as a fat storage area. This layer controls temperature, gives wholesome help and mechanically security. It conveys chief veins and nerves to skin and may contain tangible weight organs. For transdermal medication conveyance, sedate needs to infiltrate through all these three layers and venture into foundational flow while if there should be an occurrence of topical medication conveyance just entrance through stratum corneum is fundamental and after that maintenance of medication in skin layers is desired.
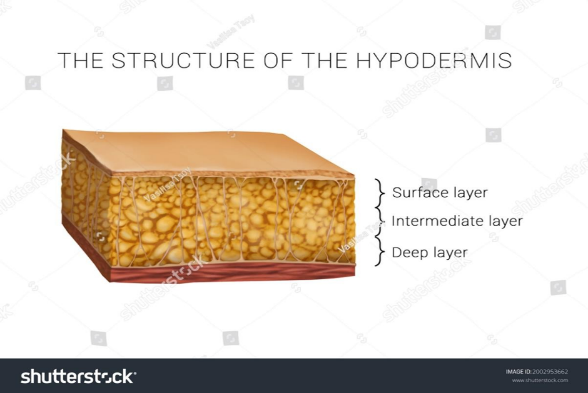
Fig. Hypodermis
Transdermal patch :
A transdermal patch is defined as adhesive medicated patch that is placed on to the above skin to deliver an exact dose of drug through the skin into the bloodstream with a predetermined rate of release to reach in the body. Today the most common transdermal system present in the market mainly based on semi permeable membranes which were called as patches. Transdermal drug delivery systems (TDDS), also known as “Transdermal patches” or “Skin patches” are dosage forms designed to deliver a therapeutically effective amount of drug across a patient’s skin and in the bloodstream.

Fig. Transdermal Patch
During storage it protect the patch. The liner should be removed before using. It is a part of primary packaging, which inhibit the loss of drug from polymer matrix.
This component is employed to bind the elements of the patch together and attach the patch to the skin. Examples of adhesives include Polyacrylate and Silicon-based adhesive polymers.
The membrane regulates the drug release from reservoir and multi-layer patches. It is typically made from materials like chitosan and poly-2-hydroxyethylmethacrylate. Examples: Silicones, polyester polyacrylonitrile, ethylene vinyl acetate copolymer and high-density polyethylene. 4.Drug
It is active ingredient which is in direct contact with release liner.
5. Polymer
The polymer must exhibit both biological and chemical compatibility with drugs and other additives such as permeation enhancers, plasticizers, adhesives, etc.
A reservoir is employed as a singular polymer layer with adhesive properties to disperse the drug. Below this single layer, an impermeable backing laminate is applied. The medication, situated within and adhering to the polymer layer, is released from the backing laminate layer, which serves as support for the drug reservoir.29 An illustration of a single-layer drug-in- adhesive transdermal patch is daytarana, which contains methylphenidatae.
Drug release is controlled over a period of time consist of a drug reservoir layer and adhesive layer.2,3 It contains a temporary protective layer and backing laminate in multilayer systems. Multi-layer patches can be prolonged for up to seven days are used to deliver pain medication, smoking cessation treatments, and hormone therapy.
elastomers, these patches consist of a single layer of adhesive polymer designed with a vapor release feature, allowing the release of vapours. Various vapor dermal patches are available for different purposes. One example is Nicoderm CQ®, a nicotine vapor transdermal patch containing essential oils that aid in smoking cessation. Introduced to the European market in 2007, it helps individuals quit smoking by releasing these oils. Another type is altacura vapor patches, which contain essential oils and are used for decongestion purposes. Additionally, there are vapor patches available in the market designed as antidepressant medications or sedatives.
Unlike the Single-layer and Multi-layer Drug-inadhesive systems the reservoir transdermal system has a separate drug layer. The drug layer is a liquid compartment containing a drug solution or suspension separated by the adhesive layer. This patch is also backed by the backing layer. In this type of system the rate of release is zero order.
The Matrix system has a drug layer of a semisolid matrix containing a drug solution or suspension. The adhesive layer in this patch surrounds the drug layer partially overlaying it.
A prototype patch can be fabricated for this a heat sealable polyester film (type 1009, 3m) with a concave of 1cm diameter will be used as the backing membrane. Drug sample is dispensed into the concave membrane, covered by a TPX {poly(4-methyl-1-pentene)} asymmetric membrane, and sealed by an adhesive. [(Asymmetric TPX membrane preparation): These are fabricated by using the dry/wet inversion process. TPX is dissolved in a mixture of solvent (cyclohexane) and nonsolvent additives at 60°c to form a polymer solution. The polymer solution is kept at 40°C for 24 hrs and cast on a glass plate to a pre-determined thickness with a knife. After that the casting film is evaporated at 50°C for 30 sec, then the glass plate is to be immersed immediately in coagulation bath [maintained the temperature at 25°C]. After 10 minutes of immersion, the membrane can be removed, air dry in a circulation oven at 50°C for 12 hrs].
Solutions containing polymers in various ratios are used in an organic solvent. Calculated amount of drug is dissolved in half the quantity of same organic solvent. Enhancers in different concentrations are dissolved in the other half of the organic solvent and then added. Di-N- butylphthalate is added as a plasticizer into drug polymer solution. The total contents are to be stirred for 12 hrs and then poured into a circular teflon mould. The moulds are to be placed on a leveled surface and covered with inverted funnel to control solvent vaporization in a laminar flow hood model with an air speed of 0.5 m/s. The solvent is allowed to evaporate for 24 hrs. The dried films are to be stored for another 24 hrs at 25±0.5°C in a desiccators containing silica gel before evaluation to eliminate aging effects. The type films are to be evaluated within one week of their preparation.
In this method drug is dissolved in polymer solution along with plasticizer. The above solution is to be stirred for 10 15 minutes to produce a homogenous dispersion and poured in to a leveled mercury surface, covered with inverted funnel to control solvent evaporation.
1In this method drug is dispersed in a mixture of water and propylene glycol containing carbomer 940 polymer and stirred for 12 hrs in magnetic stirrer. The dispersion is to be neutralized and made viscous by the addition of triethanolamine. Buffer pH 7.4 can be used in order to obtain solution gel, if the drug solubility in aqueous solution is very poor. The formed gel will be incorporated in the IPM membrane.
In order to prepare the target transdermal therapeutic system, 1?rbopol reservoir gel, polyethelene (PE), ethylene vinyl acetate copolymer (EVAC) membranes can be used as rate control membranes. If the drug is not soluble in water, propylene glycol is used for the preparation of gel. Drug is dissolved in propylene glycol, carbopol resin will be added to the above solution and neutralized by using 5% w/w sodium hydroxide solution. The drug (in gel form) is placed on a sheet of backing layer covering the specified area. A rate controlling membrane will be placed over the gel and the edges will be sealed by heat to obtain a leak proof device.
Transdermal drug delivery system may produce unstable matrices if the loading dose is greater than 10 mg. Aluminium backed adhesive film method is a suitable one. For preparation of same, chloroform is choice of solvent, because most of the drugs as well as adhesive are soluble in chloroform. The drug is dissolved in chloroform and adhesive material will be added to the drug solution and dissolved. A custommade aluminium former is lined with aluminium foil and the ends blanked off with tightly fitting cork blocks.
The proliposomes are prepared by carrier method using film deposition technique. From the earlier reference drug and lecithin in the ratio of 0.1:2.0 can be used as an optimized one. The proliposomes are prepared by taking 5mg of mannitol powder in a 100 ml round bottom flask which is kept at 60-70°c temperature and the flask is rotated at 80-90 rpm and dried the mannitol at vacuum for 30 minutes. After drying, the temperature of the water bath is adjusted to 20-30°C. Drug and lecithin are dissolved in a suitable organic solvent mixture, a 0.5ml aliquot of the organic solution is introduced into the round bottomed flask at 37°C, after complete drying second aliquots (0.5ml) of the solution is to be added. After the last loading, the flask containing proliposomes are connected in a lyophilizer and subsequently drug loaded mannitol powders are placed in a desiccator overnight and then sieved through 100 mesh. The collected powder is transferred into a glass bottle and stored at the freeze temperature until characterization.
In practically every pharmacological dose form, excipients are essential ingredients. Among other things, a formulation's stability is determined by how well the medicine and excipients work together. To create a stable product, the medicine and the excipients must work well together. Therefore, it is essential to identify any potential physical or chemical interactions as they may impact the medication's stability and bioavailability. Compatibility studies are crucial to formulation development if the excipients are novel and haven't been used in formulations with the active ingredient. By comparing their physicochemical characteristics, such as assay, melting endotherms, distinctive wave numbers, absorption maxima, etc., interaction studies are frequently conducted in thermal analysis, FT-IR, UV, and chromatographic procedures.
To guarantee the thickness of the prepared patch, the thickness of the drug-loaded patch is measured at several spots using a digital micrometer. The average thickness and standard deviation are then calculated.
Before testing, the created patches must be dried for four hours at 60°C. A predetermined patch area must be divided into various sections and weighed using a digital scale. From the individual weights, the average weight and standard deviation values must be determined.
A particular strip is to be cut uniformly and folded at the same spot repeatedly until it breaks. The value of folding endurance was determined by how many times the film could be folded in the same spot without breaking.
The prepared films are to be weighed individually and to be kept in a desiccator containing fused calcium chloride at room temperature for 24 hrs. After 24 hrs the films are to be reweighed and determine the percentage moisture content from the below mentioned formula. Percentage moisture content = [Initial weight- Final weight/ Final weight] ×100.
The weighed films are to be kept in a desiccator at room temperature for 24 hrs containing saturated solution of potassium chloride in order to maintain 84% RH. After 24 hrs the films are to be reweighed and determine the percentage moisture uptake from the below mentioned formula. Percentage moisture uptake = [Final weight- Initial weight/ initial weight] ×100.
Water vapour permeability can be determined with foam dressing method the air forced oven is replaced by a natural air circulation oven. The WVP can be determined by the following formula WVP=W/A Where, WVP is expressed in gm/m2 per 24hrs, W is the amount of vapour permeated through the patch expressed in gm/24hrs and A is the surface area of the exposure samples expressed in m2.
A specified area of patch is to be dissolved in a suitable solvent in specific volume. Then the solution is to be filtered through a filter medium and analyse the drug contain with the suitable method (UV or HPLC technique). Each value represents average of three different samples.
An accurately weighed portion of the patch is to be cut into small pieces and transferred to a specific volume volumetric flask, dissolved in a suitable solvent and sonicate for complete extraction of drug from the patch and made up to the mark with same. The resulting solution was allowed to settle for about an hour, and the supernatant was suitably diluted to give the desired concentration with suitable solvent. The solution was filtered using 0.2?m membrane filter and analysed by suitable analytical technique (UV or HPLC) and the drug content per piece will be calculated.
This test is to be performed to examine the drug crystals from patch by polariscope. A specific surface area of the piece is to be kept on the object slide and observe for the drugs crystals to distinguish whether the drug is present as crystalline form or amorphous form in the patch.
This test is to be performed for the measurement of the cohesive strength of an adhesive polymer. It can be influenced by the molecular weight, the degree of crosslinking and the composition of polymer, type and the amount of tackifier added. An adhesive coated tape is applied onto a stainless steel plate; a specified weight is hung from the tape, to affect it pulling in a direction parallel to the plate. Shear adhesion strength is determined by measuring the time it takes to pull the tape off the plate. The longer the time take for removal, greater is the shear strength.
In this test, the force required to remove an adhesive coating form a test substrate is referred to as peel adhesion. Molecular weight of adhesive polymer, the type and amount of additives are the variables that determined the peel adhesion properties. A single tape is applied to a stainless steel plate or a backing membrane of choice and then tape is pulled from the substrate at a 180º angle, and the force required for tape removed is measured.
Bypassing the digestive tract and first-pass metabolism, transdermal drug delivery systems (TDDS) offer a promising substitute for the administration of both hydrophobic and hydrophilic medications. This technique increases patient adherence and medicine absorption. The assessment methods, mechanisms, and optimization strategies required to create effective systems are all covered in detail in review papers on TDDS. However, improving TDDS necessitates a better comprehension of drug absorption mechanisms, skin physiology, and the function of excipients and polymers. Enhancing medication permeability, stability, and regulated release rates are important problems. With continuous improvements in formulation and study on skin interactions, TDDS has a lot of promise for use in medication delivery in the future. as studies progress, TDDS may emerge as a key remedy for medications with restricted oral bioavailability and sustained-release treatments, revolutionizing pharmaceutical drug delivery methods.
REFERENCES

Abhishek Morellu*, Ritesh Bharti, Ansar F. Shaikh, Rajendra Kawde, Review on Transdermal Drug Delivery System, Int. J. of Pharm. Sci., 2024, Vol 2, Issue 12, 3244-3255. https://doi.org/10.5281/zenodo.14564585
 10.5281/zenodo.14564585
10.5281/zenodo.14564585