
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmacology, Met Institute of D Pharmacy, BKC, Adgaon, Nashik- 422003.
After tumor thickness and mitotic activity, ulceration is the third most potent predictor of survival in the AJCC Melanoma Staging System and is linked to poor clinical outcomes. Males have a higher incidence of ulcerated melanoma, which also rises with age and systemic inflammatory risk factors (high body mass index, smoking, diabetes, and low vitamin D). A key component of the American Joint Committee on Cancer's (AJCC) recently updated melenoma staging system is the pathologists' evaluation of ulceration. When comparing ulcerated melanomas to non-ulcerated lesions for thickness and disease stage, the survival rates were still lower for ulcerated melanomas. We used systems biology to investigate the role of host and tumor-specific processes in determining the phenotype of ulcerated melanomas, which were thicker and more mitotically active (with corresponding transcriptomic upregulation of cell cycle pathways). Consumption of the epidermis (COE), also known as ulcerated lesions, is associated with ulcerated lesions and correlates with increased tumor cell proliferation.
Melanoma Ulcer
According to the American Joint Committee on Cancer (AJCC) Melanoma Staging System, ulceration in melanoma is characterized by three main characteristics: a full thickness epidermal defect that extends to the basement membrane, signs of a distinctive host response (neutrophils, fibrin), and thinning, effacement, or reactive hyperplasia of the surrounding epidermis. Although not all thick or highly mitotic lesions are ulcerated, the presence of ulceration may also indicate a highly proliferative phenotype, which is frequently linked to a higher mitotic rate. Ulceration is third most powerful predictor of survival in the AJCC Melanoma Staging System, with the first and second being tumor thickness and mitotic activity, respectively [1][2][3]. While tumor thickness is also considered a prognostic criterion for melanoma, and thicker tumors are more commonly ulcerated, the presence of ulceration and the extent of ulceration are both independent predictive factors [1][2]. Cutaneous melanoma is still increasing in incidence and mortality in many countries. Although immunotherapy has improved outcomes for patients with advanced disease, 40% do not benefit, and the need to better understand the biology of the tumor and host variation in response remains crucial. We have reported evidence previously that ulceration may at least in part, be driven by host systemic inflammation in that obesity, diabetes, vitamin D deficiency and smoking were associated with ulceration, in the Leeds Melanoma Cohort (LMC) (Newton- Bishop et al., 2015). This hypothesis was subsequently supported by an Australian study in which ulceration in thick tumors was associated with diabetes, and that statin use (which is reported to reduce IL-6 levels (Sepehri et al., 2016)) was protective for ulceration (von Schuckmann et al., 2017). IL-6and other molecules resulting from IL-1β signaling mediate systemic inflammation associated with an increased risk of cardiovascular disease, and suppression of this pathway has been reported to reduce lung cancer deaths (Ridker et al., 2011) [8].
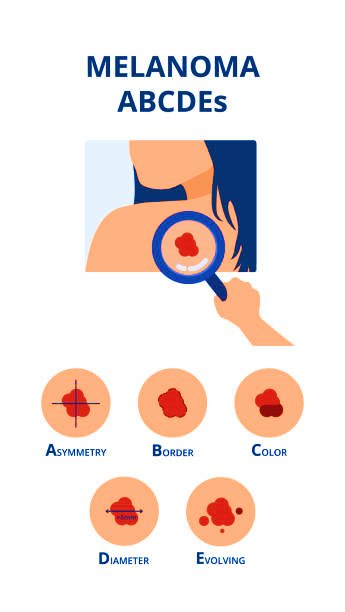
Figure 1.1 Melanoma ulcer
Epidemiology
The skin is the most common site of melanoma development (90% of melanoma cases), although this tumor can occur in any tissue containing melanocytes. The uvea is these condition most common site for melanoma and accounts for 5% of all primary melanoma cases, with UM representing the most frequently diagnosed primary intraocular malignant tumor in adults. There are constant variations in the occurrence of certain diseases in different regions of the world. Regarding UM, in the US, the incidence varies from 5.1 to 6 cases per million of the population per year, being highest in the southern latitudes. In Europe, the incidence is much higher and varies between 1.3 to 8.6 cases per million of the population per year, with eight cases per million of the population per year in Caucasians of northern European descent (Norway and Denmark) and lowest in Italy (3.3 cases per million population per year) and Spain (1.9 cases per million population per year). Although there is no consistent sex- related difference in UM, the age-adjusted incidence in epidemiological studies has revealed that men had an increased prevalence (5.8 per million in males compared to 4.4 per million in females).
Sign and symptoms

Figure 1.2 Signs and Symptoms of Melanoma ulcer
Mechanism of action
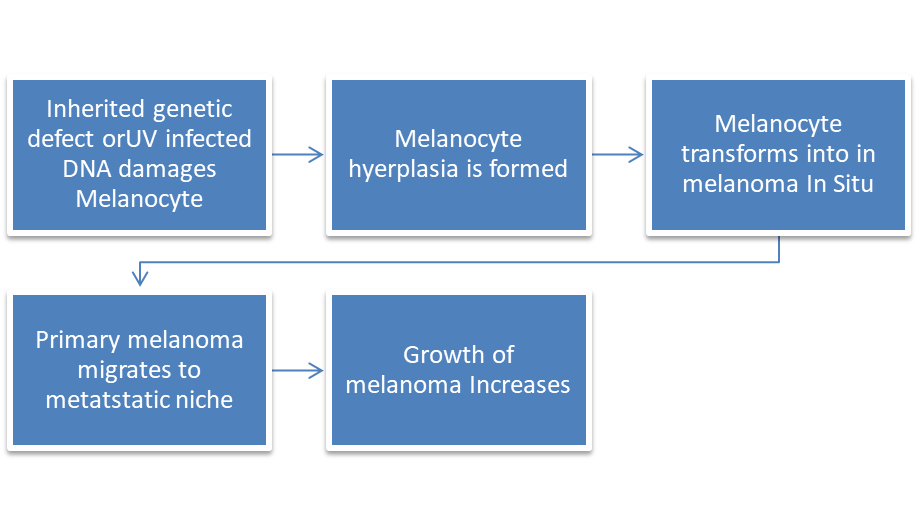
Figure 1.3 Mechanism of action of Melanoma ulcer
The cellular function of melanocytes
Cells known as melanocytes use an enzymatic cascade that comprises tyrosinase, tyrosinase-related protein-1 (TYRP1), and TYRP2/DCT (dopachrome tautomerism) to generate melanin pigments in organelles known as melanosomes. Both the orange/yellow pigment (pheomelanin) and the brown/black pigment (eumelanin) are produced when cysteine or glutathione is present. Skin and eye color polymorphism is determined by the ratio of these two types of melanin. Derived from neural crest cells, melanocytes are present in numerous parts of the human body, such as the skin, eyes, cochlea, mucosal epithelia, meninges, and heart.
Cell Morphology
Numerous distinct histologic characteristics of cutaneous melanoma, such as cell shape, have been examined to ascertain whether they may be associated with the existence of tumor ulceration. Mesenchymal cells typically have spindle cell morphology, which is characterized by an elongated nucleus and a fusiform cell shape. It is thought that between 3% and 14% of all melanoma cases are spindle-shaped cell-only melanomas. Although there is little evidence to support this claim, melanomas with exclusively spindle cell- composed portions are more common. In one study, ulcerated and non-ulcerated melanomas were equally distributed, with 7% of the included melanomas being made up of only spindle-shaped cells. Nonetheless, a greater proportion (29%) of the melanomas that were part of the study had partial spindle cell morphology, and overall, it was found that the existence of spindle cell morphology was strongly correlated with tumor ulceration in melanoma [1][11].
Ulceration
Based on microscopic analysis of the histologic sections, the AJCC defines ulceration as the lack of an intact epidermis covering a significant amount of the initial melanoma [4][11]. One poor prognostic factor for primary cutaneous melanoma is the existence of ulceration. One poor prognostic factor for primary cutaneous melanoma is the existence of ulceration. The separation of the epidermis from the underlying tumor due to sectioning or other artificial disruption must be distinguished from real ulceration. Acute inflammation and a tissue reaction to epidermal loss with fibrin are significant histopathologic indicators of actual ulceration. The prognosis is worse for patients with more widely ulcerated melanomas than for those with less ulcerated tumors. Interesting phenomena include consumption of the epidermis (COE, overall thinning of the epidermis) and cleft formation (CF, gap creation in the dermal/epidermal interface), which may be signs of early structural alterations and potential ulceration precursors. An elevated Breslow thickness and ulceration are associated with cystic fibrosis. Additionally, CD34-positive endothelial cells in the dermal/epidermal interface seal 19% of CF tumors. Between37 and 86%of all melanomas have been shown to have COE, which is characterized as thinning of the epidermis-attenuation of basal and suprabasal layers and lack of the usual rete-ridge arrangement in areas covering melanoma tissue in those regions. Although the biology underlying COE is unclear, tumor cells spreading into the epidermis (infiltrative type) or expanding and stretching the epidermis thin (attenuative type) could hypothetically be the cause of the thinning of the epidermis . One poor prognostic factor is ulceration [11].

Figure 1.2 Melanoma ulceration
Melanoma subtype
Desmo plastic melanoma is an uncommon subtype of melanoma (1-4%) characterized by the presence of spindled melanoma cells within fibro sclerotic stroma. Compared with other melanoma subtypes, it is associated with less frequent nodal metastasis, better overall survival and better response rates to immune therapy. It typically occurs in the head and neck region in severely sun-damaged skin of elderly patients. In most studies, other melanoma subtypes (apart from desmoplastic melanoma) are not independently associated with prognosis [12][13].
Impact of Sex, Age and Raceon Ulcerated Melanoma
Males experienced primary melanoma tumor ulceration at a greater rate (30.4%) than females (14.4%) in a study of 423 cases (p=0.019). Over 1800 patients participated in the multicenter, prospective, randomized clinical research known as the Sunbelt Melanoma Trial, which assessed the effectiveness of high-dose interferon alfa2b therapy in patients who had undergone a complete lymph node dissection after receiving treatment for a single positive sentinel lymph node metastasis [1][4]. Similar findings were seen in this study, which found that men with an initial cutaneous melanoma diagnosis were more likely to exhibit tumor ulceration. Other research, however, has shown that the incidence of ulceration is not associated with sex, anatomic location, or pigmentation level. Variations in sample size may be the cause of these contradictory results. Additionally, a review from the National Cancer Database suggests that ulcerated melanomas are more common among non-white people and those who are older (50 years or older) [1][5].
Risk Factors and Comorbidities
It has been demonstrated that the incidence of tumor ulceration in melanoma is correlated with a number of related illnesses and comorbidities. The incidence of tumor ulceration in cutaneous melanoma was linked to diabetes, smoking, poor vitamin D levels, and a higher body mass index (BMI) at the time of diagnosis, according to a published study examining the connection between ulceration and systemic inflammatory variables. Changes in Wnt/β-catenin signaling have been proposed as the cause of the link between ulceration and low vitamin D. Von Schuckmann et al. (2017) shown that, after controlling for age, sex, thickness, and mitotic rate, individuals who routinely took statins, aspirin, or NSAIDs had a lower chance of receiving a diagnosis of ulcerated melanoma (OR 0.68, 95% CI 0.46-1.00). 23 Statins may prevent the development of melanoma, according to early epidemiologic studies, however more recent research contradicts this conclusion. Instead, it is proposed that more regular medical surveillance might be linked to the start of statin therapy [1][6][7].
Patterns of Gene Expression, Associated Mutations, and Molecular Signatures
Several studies have attempted to describe the molecular markers, related oncogenic alterations, and gene expression profile of ulcerated melanoma. Numerous mechanisms via which afflicted patients may have an elevated risk of metastasis and recurrence have been identified by the identification of distinctive molecular characteristics linked to ulcerated tumors, and as such, may have prognostic significance [1].
METHODS [8]
Human sample and data methods
The LMC is a prospective cohort of 2184 primary melanoma patients recruited from a geographically defined area of the UK in the period 2000-2012, The Vitamin D and Immunity Study (VDI) REC reference 13/YH/0237 is a second cohort of 393 primary melanoma patients recruited at diagnosis, making their first visit to the Leeds Melanoma Multidisciplinary Clinic. Here, we report the analysis of ulceration status in association with clinicopathological variablesand serum vitamin D levels at diagnosis. The VDI histopathological data were extracted from the summary of the Leeds multidisciplinary team review, which was carried out for all participants according to protocol.
Association of tumor and host variables with ulceration and melanoma specific survival
The analysis of clinic pathological factors used data collected from the entire LMC cohort of 2184 people and that from 393 participants in the VDI study. Tumor analyses were carried out on the subset of LMC 703 tumors which were large enough to sample yet leave sufficient tumor in the formalin-fixed tumor blocks for subsequent clinical testing if needed. The quantity of DNA and RNA extracted from tumor tissue was limited by tumor size, and therefore, transcriptomic and sequencing data did not overlap completely
Genomic data generation
Formalin-fixed paraffin-embedded (FFPE) primary melanomas were sampled using a 0.6mm diameter tissue microarray (TMA) needle inserted horizontally consistently through the least inflamed part of the invasive tumor. DNA/RNA were extracted from 820 tumor cores. DNA samples were used to generate copy number data from 303 of the samples as reported. Samples were selected only on the basis of there being sufficient DNA available. Targeted capture was performed on 554 genes using Agilent Sure Select XT probes. The baits included 164 melanoma-associated genes, 245 known to be associated with other solid cancers, common melanoma promoter mutations, and 101 genes from the interferon signaling pathway. Human leucocyte antigen (HLA) regions were also screened. Sequencing designed to generate copy number data was carried out using the Illumina HiSeq4000 platform, using 75 bp paired-end reads and data were mapped to GRCh37d5 with BWAMEM 0.7.15 and somatic variants were called using the Caveman algorithm (v.1.11.2). The mutation load was analyzed for its association with ulceration, defined as summated non-synonymous mutations. As the melanoma primary samples are small, there was insufficient material to process all samples using the three different platforms and the overlaps.
Analysis of genomic data
Associations between individual mutations detected and ulceration status were tested using logistic regression. Differential gene expression by ulceration status was used to identify biological pathways associated with ulceration. The transcriptomic data were also subjected to a bioinformatic inference of the presence of specific immune cell subgroups in tissues (Angelova et al., 2015), in association with ulceration status. Gene level data associated with ulceration status were generated from segmented copy number using GISTIC (Software. broad institute.org). The resultant analysis identified ‘influencer’ genes and ‘influenced’ genes associated with ulceration.
RESULT
There were 187 ulcerated tumors in the LMC (of 576 total examined, 32%) and 153 ulcerated in the VDI study (out of 391 total 39%) Ulceration was more common with increasing age in both the LMC and VDI data sets, and this was independent of other variables in the larger LMC data set. Ulceration was more common in men but this was not independent of other factors Ulceration was more common in tumors arising in sun-protected sites such as acral and genital tumors in the LMC data set independent of thickness and age. Total tumor mutation load data were available for 498 participants in whom blood test results were also available, and in a unvariable analysis, there was evidence that ulceration was less frequent in tumors with a higher mutation load.
Melanoma Diagnosis and Histopathological Examination
A variety of biopsy methods, each suited to certain clinical situations and diagnostic needs, are employed to establish a pathological diagnosis of melanoma (see Image. Spitz Melanoma of the Skin). For the best possible diagnosis and treatment, the following factors and methods are advised by the 2024 National Comprehensive Cancer Network Guidelines for Cutaneous Melanoma (NCCN Cutaneous Melanoma):
Histopathological examination of biopsy specimens is paramount for confirming the diagnosis of melanoma and providing crucial information for subsequent management. Pathologists experienced in melanocytic neoplasms should report the biopsy, utilizing appropriate immune histochemical stains and molecular testing for histologically equivocal lesions. Essential elements to be reported include Breslow thickness, ulceration, microsatellites, margin status, dermal mitotic rate, lympho vascular or angio lymphatic invasion, histologic subtype, regression, and neurotropism. Synoptic reporting containing this information is strongly recommended for optimal patient care [9].
CONCLUSION
The incidence of ulcerated melanoma is greater in males, in patients 50 years or older. Risk factors such as diabetes, smoking, low vitamin D, and elevated body mass index have also been associated with an increased occurrence of ulcerated melanoma. Histologically, spindle cell morphology has been shown to correlate significantly with tumor ulceration, along with vascular density, vasculogenic mimicry, and angiotropism. Ulceration is third most powerful predictor of survival in the AJCC Melanoma Staging System, with the first and second being tumor thickness and mitotic activity, respectively. While tumor thickness is also considered a prognostic criterion for melanoma, Histologically, spindle cell morphology has been shown to correlate significantly with tumor ulceration, along with vascular density, vasculogenic mimicry, and angiotropism. Ulcerated tumours were thicker and more mitotically active which is consistent with the genomic analysis, in which upregulation of biological pathways associated with cell proliferation was observed. Here, we report that the neural network analysis identified Wnt/β-catenin signalling as associated with ulceration, a pathway known to be associated with reduced host immune responses to melanoma. Also here, we report that in the significantly smaller VDI study the data were consistent with an increased risk of ulceration in vitamin D deficiency. The tumour analyses provide evidence that ulcerated melanomas are thicker and more mitotically active which is well known. Older community-living people are affected by a high number of skin conditions and diseases, but the current evidence about the burden and effective prevention and treatment strategies is weak.
REFERENCES

Sakshi Rathod*, Atharv Nimse, Rahul Patil, Yogesh Wankhede, A Systematic Review on Epidemiology, Risk Factors, Diagnosis & Treatment Associated with Melanoma Ulcer, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 3, 2472-2479. https://doi.org/10.5281/zenodo.15084248
 10.5281/zenodo.15084248
10.5281/zenodo.15084248