
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
*Research Scholar1, Assistant Professor2, Research Scholar3, Research Scholar3, HOD Pharmacology department3,Channabasweshwar Pharmacy College (Degree), Latur.
One of the most serious non-communicable disease crises of the twenty-first century is Liver damage caused by drugs, chemicals, toxins, alcohol, and herbal products is a significant global health concern. The liver plays a crucial role in detoxifying the body by eliminating harmful substances, which makes it highly vulnerable to damage. Hepatotoxicity can be classified by cause (intrinsic, idiosyncratic, immune-related), symptom type (hepatocellular, cholestatic, mixed), tissue changes (necrosis, steatohepatitis, cholestasis, granulomatous or vascular injury, autoimmune-like hepatitis), and severity (mild to life-threatening liver failure). Drug-induced liver injury (DILI) is a common cause of sudden and severe liver failure, often linked to antibiotics and herbal products. Chemical-induced liver damage is typically associated with occupational or environmental exposure and can result from industrial solvents, pesticides, heavy metals, and other harmful substances. Other harmful agents include alcohol, toxins, and environmental pollutants. The process of liver injury involves multiple mechanisms, such as oxidative stress, mitochondrial damage, lipid metabolism disruption, immune reactions that lead to inflammation, and the progressive formation of scar tissue in the liver. Medical professionals often use tests such as alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), bilirubin, glutathione, malondialdehyde, and alpha-fetoprotein to detect and monitor liver damage at an early stage. Advances in research have increased our understanding of how the liver is affected by various factors. The models, including animal models, human-like liver systems, three-dimensional liver cultures, and co-culture systems of liver cells, to investigate these issues. Older individuals and those with pre-existing liver issues are particularly at risk. Therefore, early detection, careful risk assessment, and effective prevention strategies are essential in reducing the worldwide burden of liver damage
Hepatotoxicity refers to the condition where the liver suffers damage or operates improperly due to excessive exposure to drugs or other harmful substances (Francis & Navarro, et al. 2025). The liver is a crucial organ that performs several essential functions in the body. It helps in breaking down food, producing proteins, creating bile for digestion, and eliminating old red blood cells. Additionally, it regulates blood sugar levels and filters out harmful chemicals (PubMed, 2023). Liver damage is a significant cause of acute hepatitis and acute liver failure globally (PubMed, 2025).
The liver functions effectively because of various complex processes, such as fat metabolism, glucose regulation, and the removal of harmful substances. Since the liver is central to the body’s metabolism, it is particularly vulnerable to the effects of medications and other harmful substances (Drug-Induced Liver Injury, 2023). Factors that can raise the risk of liver damage include age, gender, alcohol consumption, smoking, taking multiple medications, having a pre-existing liver condition, and differences in genetic and environmental factors (PubMed, 2023).
A wide range of harmful substances can lead to liver problems. These include chemicals like alcohol, carbon tetrachloride, and chlorinated hydrocarbons; certain cancer medications like azathioprine, doxorubicin, and cisplatin; immunosuppressive drugs such as cyclosporine; pain relievers and anti-inflammatory drugs like paracetamol and thioacetamide; tuberculosis medications including isoniazid and rifampicin; vaccines such as the Bacillus Calmette-Guérin (BCG) vaccine; radiation; heavy metals like cadmium and arsenic; toxins produced by Molds known as mycotoxins, including aflatoxin; and other harmful substances like galactosamine and lipopolysaccharides (Francis & Navarro, et al. 2025).
Liver damage can be classified in various ways. Based on the cause, it can be intrinsic, which is predictable and occurs at specific dosages; idiosyncratic, which is unpredictable and not dose-dependent; or immune-related, involving allergic or autoimmune reactions (Drug-Induced Liver Injury, 2023). Based on symptoms, it can be hepatocellular, involving damaged liver cells; cholestatic, which involves blocked bile flow; or a combination of both. Based on the affected parts of the liver, it can be steatohepatitis (fatty liver disease), cholestasis (blocked bile flow), granulomatous hepatitis (inflammatory reaction), or vascular issues. Based on the severity of damage, it can range from mild to severe, depending on the extent of liver injury and the body's response (PubMed, 2025).
The causes of liver damage include toxic substances directly harming liver cells, leading to increased levels of free oxygen in the body (oxidative stress), dysfunction in the liver’s energy production (mitochondrial issues), immune system attacks, and blockage of bile flow causing cholestasis. These processes can lead to the death of liver cells through either natural cell death (apoptosis) or sudden, uncontrolled cell death (necrosis) (PMC, 2013).
Certain biological markers help in detecting and understanding liver damage. Elevated levels of blood enzymes such as aspartate aminotransferase (AST), alanine aminotransferase (ALT), alkaline phosphatase (ALP), and total bilirubin indicate liver injury or blocked bile flow. Higher levels of malondialdehyde (MDA) suggest more damage from fat breakdown, while changes in glutathione (GSH) levels point to oxidative stress. Alpha-fetoprotein can also signal liver injury (PubMed, 2025).
Scientists study liver damage through various models, such as animal models and human cell models in the laboratory. In animal models, they use drug-induced, alcohol-induced, chemical-induced, herb-induced, and models that mimic fatty liver disease or human conditions. In cell models, they use cell lines, liver slices, or 3D and co-culture systems. 3D systems resemble real liver environments more closely, leading to healthier liver cells and better drug metabolism. Co-culture systems, which include liver cells along with other cell types, enhance liver cell function and enable them to respond more naturally to different signals (Francis & Navarro, et al. 2025).
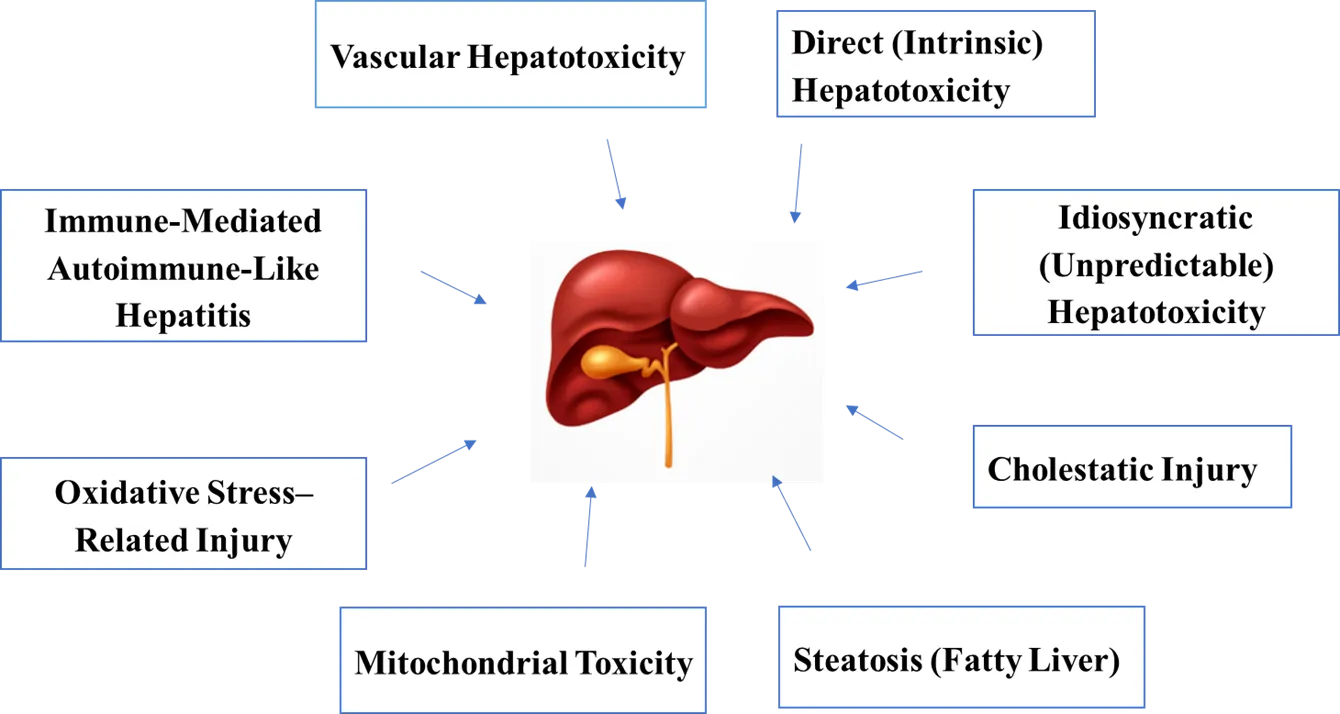
Fig. 1: Causes of Hepatotoxicity
Hepatotoxicity causes:
Epidemiology
Hepatotoxicity is a major health problem worldwide, caused by exposure to drugs, chemicals, and other harmful substances. Drug-induced liver injury (DILI) is not very common but still very important in clinical settings. Globally, about 4.94 cases happen for every 100,000 people each year (Shen T et, al. 2019). Since 2010, the number of cases has gone up, and there are big differences depending on the region. The highest rates are in Asia (17.82 per 100,000 person-years) and the lowest in North America (1.72 per 100,000 person-years).
Older people are more likely to be affected, but the rates are similar for men and women. The most common cause of DILI is antibiotics, especially amoxicillin-clavulanate, followed by anti-tubercular drugs, statins, nonsteroidal anti-inflammatory drugs, and herbal supplements (Zhang, L., et al. 2023). Chemical-induced liver damage is often seen in workplaces and industries where people are exposed to solvents, pesticides, chlorinated hydrocarbons, carbon tetrachloride, and heavy metals like arsenic and cadmium. The risk depends on how much someone is exposed, how long they are exposed, the way they are exposed, and how well safety measures are followed. Even small amounts over a long time can lead to serious liver damage, especially in areas with poor industrial safety rules (Balali Mood, M., et al. 2021).
Other harmful substances, like mycotoxins (for example, aflatoxin), alcohol, ionizing radiation, and environmental toxins, also cause liver damage around the world. Alcohol-related liver injury is one of the main causes of chronic liver damage globally, while mycotoxin exposure is more common in warm and humid regions. Together, these factors show that liver damage can come from many different causes and is influenced by where people live. This highlights the need for better monitoring, prevention, and early detection to help reduce the global impact of liver disease (Teschke, R, et al. 2024).
Classification of hepatotoxicity
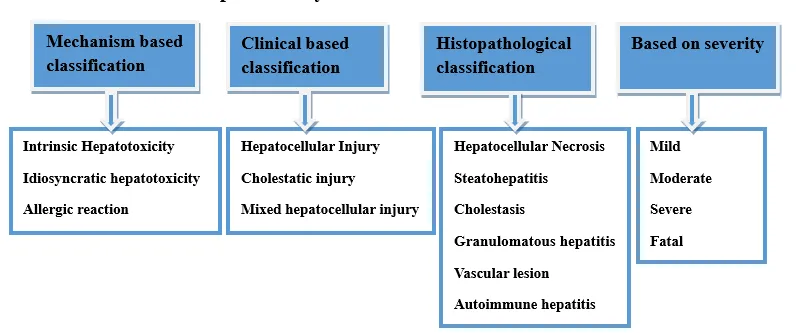
Fig. 2: Classification of Hepatotoxicity
A] Mechanism Based Classification
1) Intrinsic Hepatotoxicity:
The liver is often affected by harmful substances, such as certain drugs and chemicals. This kind of damage happens when the amount of these harmful substances in the body goes beyond a certain level, and the more of them there are, the worse the damage becomes. This type of liver harm is easy to predict and happens in a way that’s connected to how much of the harmful substance is present. It's the most studied form of liver damage because it's very important in real-world medicine. Everyone can be affected if they take in a high enough amount, with more harm coming from higher doses. After being exposed, there's a noticeable time period before symptoms show up. This exposure also causes specific kinds of liver injuries that can be seen under a microscope. A good drug should work well but cause liver damage only at very high doses, relative to the amount that could be deadly. Inflammation in the body, caused by microbes or things they produce, can make tissues more sensitive to harmful substances. This makes them more likely to be damaged by toxic chemicals.
2) Idiosyncratic hepatotoxicity:
Idiosyncratic hepatotoxicity is when a drug or chemical causes unexpected liver damage, but only in certain people who are more sensitive to it. This type of reaction isn't clearly linked to how much of the drug is taken. The word "idiosyncratic" means something that happens in a special or unusual way for certain individuals, and these are called idiosyncratic drug reactions (IDRs) (Alastair Mak, 2017). It's hard to diagnose IDILI because there are so many different drugs, herbs, and symptoms that can be involved, and there aren't clear markers to help identify it. This condition can lead to serious liver failure (Andrade, R. J., et al. 2019). IDRs make up about 10% of all harmful reactions to drugs (Thomas Hunziker, et al. 2002). Most cases of IDILI are probably due to the immune system. The delayed appearance of symptoms is because the body takes time to develop a reaction, like when T and B cells start multiplying after being exposed to a foreign substance. This process happens after the innate immune system has already started responding and presenting the harmful substance to the body's defences (Medzhitov, R., et al. 1997). In practice, IDILI is known for happening in a unique way and showing up later, usually 1 to 3 months after starting the drug, but it can also happen sooner, even after more than a year of use, or even after stopping the drug more than 3 weeks ago (Alison Jee, et al. 2021).
3) Allergic reaction:
Allergic hepatotoxicity is a kind of liver injury that happens when the immune system reacts badly. People who get this condition may feel feverish, develop a skin rash, have more eosinophils in their blood, and the symptoms can appear quickly (Zhang-Xu Liu, et al. 2002). The liver's immune system is different from other parts of the body. It mainly depends on the innate immune cells, and the role of the adaptive immune system is smaller. The liver has special types of white blood cells, like NKT cells, which act like both T-cells and natural killer cells. These NKT cells make up about half of the T-cells found in the liver (Abo T, et al. 1997). Even though we understand more about how drugs are processed and how harmful byproducts are made, we still don't know much about the immune responses they trigger. These reactive or unstable byproducts can stick to proteins inside cells, making new antigens that can start an immune response through antibodies or T-cells. This immune response can then harm liver cells (Alastair Mak, et al. 2017).
B] Clinical based classification:
1) Hepatocellular injury:
Drug-induced liver injury that resembles acute viral hepatitis mainly harms the liver cells. When a liver biopsy is done, it typically shows serious damage and swelling in the liver cells, with only a small amount of bile buildup in the early stages. Other signs from the body and blood tests can also show that the liver cells are damaged. When someone has symptoms, they often feel very tired and weak. The levels of two important liver enzymes, ALT and AST, are usually very high, often more than ten times the normal maximum level. However, the levels of other enzymes like ALP and GGT are only slightly higher.
2) Cholestatic injury:
Drug-induced cholestatic liver damage often looks like a blockage in the bile ducts or the presence of gallstones. When a liver biopsy is done, it shows signs of bile buildup, inflammation around the portal areas, and changes in the bile ducts and small bile channels. People with this condition usually have yellowing of the skin and eyes, which is called jaundice, and they may feel itchy all over. Some people also feel pain in the upper right part of their abdomen. Blood tests typically show very high levels of alkaline phosphatase (ALP) and gamma-glutamyl transpeptidase (GGT), but the levels of alanine aminotransferase (ALT) and aspartate aminotransferase (AST) are only slightly or moderately increased. The level of bilirubin in the blood is usually higher than what would be expected based on the amount of liver cell damage (Bethesda MD, et al. 2012).
3) Mixed hepatocellular injury:
Some medicines can cause liver damage that affects two main parts of the liver. This kind of damage is often seen with many drugs and is the most common type of liver injury caused by medicines. It's not usually found in other kinds of sudden liver problems. If a doctor takes a small piece of the liver for testing, they might find many dead liver cells, swelling, and a buildup of bile. People with this problem may feel very tired and have a skin rash that itches a lot. Blood tests usually show higher than normal levels of two enzymes, ALT and ALP.
C] Histopathological classification:
1) Hepatocellular necrosis:
Hepatocellular necrosis is when the main cells of the liver, called hepatocytes, get injured and die. It can happen in different ways:
2) Steatohepatitis:
Fatty liver, also called hepatic steatosis or hepatosteatosis, happens when fat builds up inside the liver cells. While it can happen with many health conditions, the term is mostly used for fatty liver disease. In a healthy liver, there is very little or no fat.
A small amount of fat is usually not a big issue. But when there is too much fat, it can lead to other health problems like diabetes, heart disease, and stroke. If the condition gets worse, fatty liver disease can turn into cirrhosis, which is serious liver damage. Cirrhosis greatly raises the risk of liver cancer (Stephanie Hernandez, et al. 2025).
3) Cholestasis:
Cholestasis is a condition where the flow of bile is blocked somewhere between the liver cells that make bile and the duodenum, which is the first part of the small intestine. When the bile flow is stopped, a substance called bilirubin, which is made when old or damaged red blood cells break down, leaks into the blood and builds up.
Normally, bilirubin is processed in the liver, put into bile, carried through the bile ducts to the intestine, and mostly removed from the body through stool, with a little bit also leaving the body in urine.
Causes of cholestasis include:
4) Granulomatous hepatitis:
Granulomatous hepatitis is a type of liver inflammation where small groups of special immune cells, called granulomas, form inside the liver. These granulomas are made up of certain types of immune cells like epithelioid macrophages and other inflammatory cells. About 2.4 to 10% of liver biopsies show these granulomas. The most common reasons for this condition are sarcoidosis and tuberculosis, but in about 36% of cases, the exact cause is not known.
Granulomas happen when the immune system tries to fight off something it can't get rid of, like certain bacteria or other foreign substances. This causes the release of immune signals called cytokines, which bring more immune cells to the area. These cells can sometimes join together to form larger cells called multinucleated giant cells. The level of inflammation can be mild or severe. When granulomas are found along with a lot of surrounding inflammation, it is called granulomatous hepatitis. A liver biopsy is used to confirm this condition (Hima Doppalapudi, et al. 2024).
5) Vascular lesion:
Drug and toxin exposure can lead to various types of liver damage that affect the blood vessels in the liver. These issues can involve the hepatic veins, sinusoids, portal vein, and hepatic arteries. Some of the conditions that can result include blockage of the hepatic veins, enlargement of the sinusoids, formation of blood-filled cysts, scarring around the sinusoids, and other changes in the blood vessels. In some cases, drugs can also cause tumors in the blood vessels or changes in the blood vessels within other types of liver tumors. It is important to understand how these problems develop and how common they are, so that they can be detected early and prevented, as they can harm the liver (Elie Serge Zafran, et al. 1983).
6) Autoimmune hepatitis:
Autoimmune hepatitis is a long-term illness that causes inflammation in the liver. It occurs when the body's immune system, which usually helps fight off infections, starts attacking the healthy liver cells by mistake. This ongoing attack leads to inflammation in the liver, which can get worse over time. Usually, the immune system creates antibodies to protect the body from harmful germs. However, in autoimmune hepatitis, the immune system doesn't function correctly and ends up harming the liver instead. There is no known cure, but taking medicines that slow down the immune system for a long time can help reduce inflammation, prevent the liver from getting more damaged, and lower the risk of serious complications. If not treated, the disease can cause serious liver damage, such as cirrhosis or liver failure, which can be life-threatening. Autoimmune hepatitis is not very common. It's estimated that about 10 to 50 people in every 100,000 have this condition (Jong Woo Hahn, et al. 2023).
D] Based on severity:
Hepatotoxicity can range from very mild to life-threatening. The seriousness depends on how much the liver is affected. It is usually described using certain guidelines like:
Mechanism of hepatotoxicity
Hepatocytes, cholangiocytes, Kupffer cells, ductal cells, and endothelial cells all play a role in drug-induced liver damage. Drugs can directly affect parts of cells like mitochondria, endoplasmic reticulum, cytoskeleton, microtubules, and the nucleus (Alejandra Cano Paniagua, et al. 2017).
Carbon tetrachloride (CCl4) is an industrial chemical that is well-known for causing liver damage. It can be found in some insecticides, fire extinguishers, and fumigated grains, which means people might be exposed to it. Because its effects on the liver are well understood, CCl4 is often used in experiments to study liver injury, oxidative stress, and liver scarring (Renye Que, et al. 2022).
In humans, exposure to CCl4 can lead to liver damage and scarring, which is why it's commonly used in research to create models of liver toxicity (Y.H. Yeh, et al. 2013). In the liver, CCl4 is broken down by enzymes like cytochrome P450, mainly CYP2E1, CYP2B1, CYP2B2, and possibly CYP3A, to form a highly reactive molecule called the trichloromethyl radical (CCl3·). This radical can react with oxygen to create another reactive molecule, the trichloromethyl peroxyl radical (CCl3OO·).
Both of these radicals are very reactive and can harm cells by attacking lipids, proteins, and DNA, leading to liver cell damage and death. Because of this, CCl4 is widely used in experiments to study liver toxicity. The CCl3· radical can stick to parts of the cell, disrupting how lipoproteins are handled and affecting how fats are transported.
This can lead to fat accumulation in liver cells, known as steatosis (Ying Xu, et al. 2018). It can also attach to DNA, creating CCl3-DNA adducts, which might start the process of liver cancer. The CCl3OO· radical starts a process called lipid peroxidation, which damages fats in cell membranes, especially the unsaturated fats in phospholipids, and can break down the cell membrane (Lutz W. D. Weber, et al. 2003).
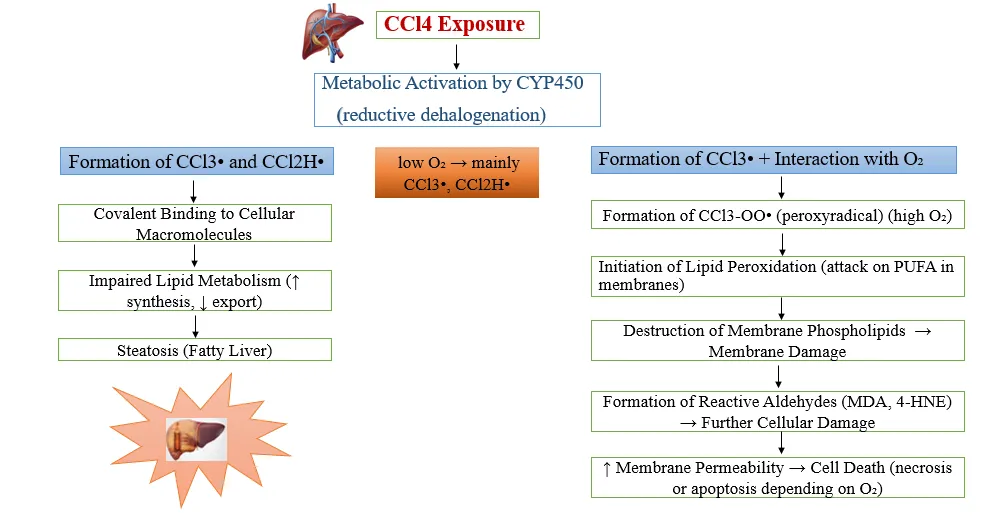
Fig. 3: Mechanism of Hepatotoxicity
Lipid peroxidation:
When the body breaks down carbon tetrachloride (CCl4), it creates two types of harmful chemicals: trichloromethyl (CCl3·) and trichloromethyl peroxyl (CCl3OO·) radicals. These are very strong chemicals that can stick to important molecules in the body like DNA, proteins, and fats, causing harmful side effects. In the presence of oxygen, the trichloromethyl radical (CCl3·) turns into trichloromethyl peroxyl radical (CCl3OO·), which is even more active. This new form can take away hydrogen atoms from certain fats, especially those with multiple double bonds like polyunsaturated fatty acids (PUFAs). This starts a chain reaction that harms the cell membranes that contain these fats. This process is known as lipid peroxidation, and it makes the membrane structure weaker.
Lipid peroxidation begins when free radicals like hydroxyl (OH·), alkyl (RO·), or peroxyl (ROO·) take a hydrogen atom from PUFAs, forming a carbon-based radical (L·). This L· then reacts with oxygen to create a lipid peroxyl radical (LOO·). This LOO· takes a hydrogen from nearby fatty acids, forming lipid hydroperoxides (LOOH). When metals are around, LOOH can split into lipid alkoxyl radicals (LO·). Both LO· and LOO· can break down into harmful aldehydes, such as malondialdehyde (MDA), 4-hydroxynonenal (HNE), and acrolein (ACR).
These aldehydes can change proteins and DNA in cell membranes, leading to more oxidative stress and inflammation, which are connected to several diseases. As the membranes become damaged, their structure changes, making them leaky. This affects their ability to move ions and carry out important functions. This can lead to liver cell damage and eventually liver failure (Hina Khalid, et al. 2021).
Oxidative stress and cell damage:
Reactive oxygen species (ROS) are made naturally in the body during regular processes that use oxygen. They help with cell communication, protection, and controlling genes. Free radicals are a kind of ROS, and they have one unpaired electron, which makes them very active and unstable (Finkel, et al. 2000). While ROS are needed for normal cell activities, too much of them, along with reactive nitrogen species (RNS), can be harmful. They can damage fats, proteins, and DNA, leading to cell injury (McCord J.M, et al. 2000). In the liver, high levels of ROS are a main reason for liver cell damage and the beginning of scar tissue. Oxidative stress changes how fats, proteins, and DNA are structured and work, causing cells to die. This can also trigger apoptosis, which is a type of programmed cell death. Additionally, oxidative stress increases signals that lead to inflammation. ROS also make liver cells and other immune cells release harmful chemicals, and they directly activate cells that build scar tissue, making fibrosis develop faster (Sanchez-Valle, et al.2012).
Inflammation and fibrosis:
Hepatotoxicity often comes with an inflammatory reaction. Certain harmful chemicals and the body's own stress from free radicals can lead to the death of liver cells, either through necrosis or apoptosis. When this happens, substances inside the cells, called damage-associated molecular patterns, are released. These DAMPs activate immune cells that are already in the liver, like Kupffer cells, as well as immune cells that come from other parts of the body. This activates the release of proteins that cause inflammation and attract more immune cells. This type of inflammation, which happens without infection, can make liver damage worse but is also important for repairing and regenerating the liver. However, if the inflammation continues or gets too strong, it can make the liver damage worse and lead to the development of scar tissue, or fibrosis, as described by (Kavita Gulati, et al. 2018).
Mitochondrial Dysfunction:
Mitochondria are essential for the body's energy process. They help break down fats through a process called fatty acid beta-oxidation, take part in the tricarboxylic acid cycle, and produce energy through oxidative phosphorylation. They also create reactive oxygen species (ROS), which can lead to cell damage and death if they build up too much. When mitochondria can't properly break down fats, it can cause a type of fat buildup in the liver called micro vesicular steatosis. This can get worse and lead to serious problems like liver failure, coma, and even death. If this fat buildup happens over a long time, and the mitochondria also have trouble with their energy-making process, it can increase ROS production. This causes more damage to the fats in the liver, leading to conditions like steatohepatitis. This condition causes liver cells to die, causes inflammation, forms structures called Mallory bodies, and leads to scarring of the liver. These changes also lower the levels of a protective substance called glutathione (GSH) and raise levels of a harmful byproduct called malondialdehyde (MDA), which shows that there is a lot of oxidative stress. The ROS produced in this situation can also cause the mitochondrial permeability transition pore to open, leading to mitochondrial damage.
Biomarkers:
Hepatotoxins can cause various signs and symptoms affecting the liver, both in terms of clinical presentation and microscopic changes. The condition of the liver can be evaluated through biochemical indicators like alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), and bilirubin levels. When these enzymes are found in higher-than-normal amounts in the blood, it suggests damage to liver cells. An increase in total and conjugated bilirubin levels points to the liver's overall functioning. A significant rise in both transaminases and bilirubin levels, exceedingly twice the normal upper limit, is a strong sign of liver toxicity. Further confirmation of liver damage can be obtained through visual inspection, microscopic analysis of tissue samples, and the evaluation of other biochemical tests (Anita Singh, et al. 2021).
Fig. 4: Different Biomarkers of Liver Injury
Alanine aminotransferase, also referred to as serum glutamic pyruvic transaminase, is a significant biomarker used to evaluate liver damage. This enzyme plays a crucial role in the metabolic processes involving amino acids and the production of glucose. It facilitates the transfer of an amino group from alanine to alpha-ketoglutarate, resulting in the formation of glutamate and pyruvate.
The typical range for normal levels of ALT in the blood is between 5 and 50 units per liter. Higher than normal ALT levels suggest potential harm or injury to the liver, as this enzyme is mainly found in liver cells. Hence, the measurement of ALT activity offers a more precise reflection of liver health compared to other enzymes that are not specifically associated with the liver (Dufour DR, et al. 2016).
Aspartate Aminotransferase (AST), also known as Serum Glutamic Oxaloacetate Transaminase (SGOT), is an enzyme found in the liver that plays a role in the process of protein metabolism. This enzyme helps in moving an amino group from aspartate to alpha-ketoglutarate, resulting in the formation of oxaloacetate and glutamate. Although AST is mainly found in the liver, it is also present in other organs such as the heart, skeletal muscles, brain, and kidneys.
When there is damage to any of these tissues, the level of AST in the blood can increase. Typically, the normal range for AST in the blood is between 7 and 40 units per liter. (Rahul A Nathwan, et al. 2005) AST serves as a marker for cell death in the liver, but it is not as specific as another enzyme called alanine aminotransferase (ALT). To help distinguish between liver-specific injury and damage occurring in other parts of the body, the ratio of AST to ALT in the blood is often examined(Amacher DE, et al. 2002).
Alkaline Phosphatase (ALP) is a type of enzyme known as a hydrolase, which is mainly released into bile. This enzyme helps break down esters that contain a single phosphate group, and it works best in an alkaline environment. ALP is most abundant in the cells that line the bile ducts within the liver, but it is also found in other tissues such as bone, placenta, kidney, and intestine. In humans and animals used in research, several different forms, or isozymes, of ALP have been identified. The usual range for ALP levels in the blood is between 20 and 120 units per liter. When ALP levels increase, it is often because there is a problem with the flow of bile, which can happen if the liver is damaged. Conditions that harm the liver or block the bile ducts can lead to higher ALP levels because the enzyme is not properly removed from the body through bile (Wright TM, et al. 2007).
Bilirubin is a substance that naturally occurs in the body and is formed as a result of the normal breakdown of haemoglobin, which is found in red blood cells. This substance is processed by the liver and then released into bile. In the blood, typical levels of bilirubin are usually between 0.2 and 1.2 mg/dL. When there is damage to liver cells, the liver may not be able to properly remove bilirubin from the blood, leading to its buildup in the bloodstream and surrounding body fluids. Higher levels of bilirubin can also occur if there is an increase in serum albumin, which helps move bilirubin from tissues into the blood, or if the liver is not effectively clearing it. An excessive amount of bilirubin can lead to jaundice and other symptoms related to liver damage. A rise in bilirubin with little or no increase in ALT (alanine aminotransferase) levels often suggests a condition called cholestasis. In cases of sudden liver injury, total bilirubin levels may provide a more accurate indication of how severe the disease is compared to ALT levels. Bilirubin is measured in two forms: total bilirubin and direct bilirubin. Total bilirubin gives an overall picture of all bilirubin present in the blood, while direct bilirubin refers to the water-soluble, conjugated form that the liver produces, and it typically ranges from 0 to 0.3 mg/dL. Indirect bilirubin, which is the unconjugated form, is determined by subtracting direct bilirubin levels from total bilirubin levels.
Total protein is a clinical measure that reflects the combined amount of albumin and globulins present in the blood. Since the liver is primarily responsible for producing most plasma proteins, a decrease in total protein—especially in albumin—can signal impaired liver function, particularly in cases of chronic or severe liver disease. Assessing total plasma protein levels is important for distinguishing between normal and impaired liver function. The typical range for total protein in the blood is between 6.0 and 8.3 grams per decilitre. In conditions involving liver injury, total protein levels might decrease slightly. However, the albumin-to-globulin (A/G) ratio tends to decrease more significantly, which indicates reduced albumin production and changes in globulin levels due to damage to the liver cells.
Malate dehydrogenase (MDH) is an enzyme found in the citric acid cycle that helps in the reversible conversion of malate into oxaloacetate, with NAD+ acting as a helper molecule. The enzyme is most active in the cytoplasm of the liver, followed by the heart, skeletal muscle, and brain. Since MDH is located near the portal areas of the liver, it can be released into the bloodstream when there is damage to the tissue. The typical range of MDH levels in the blood is between 23.5 and 47.7 units per liter. Increased levels of MDH have also been linked to structural changes in the liver. Studies have shown that measuring MDH activity provides more accurate information about the extent of liver damage compared to measuring AST levels.
Glutathione (GSH) is the most plentiful non-protein thiol found inside cells, with high concentrations present in the liver, where it is mainly produced and processed. While GSH is found in almost all tissues and organs, the liver has the highest levels because it plays a key role in metabolic detoxification. GSH is important for managing excess oxidative stress in the liver and provides wide-ranging protection to cells. In addition to its main role as an antioxidant, GSH helps support normal metabolic processes, keeps cell membranes stable, maintains enzyme function, aids in internal communication between cells, and influences gene activity (Youzhi Lin, et al. 2017). As the main defense against oxidative stress that occurs during cell respiration, GSH is also a common target of harmful substances. The balance of glutathione levels is a complex process involving multiple organs, with the liver playing the main role, while skeletal muscle, the lungs, and the kidneys also contribute significantly (M. Kretzschmar, et al. 1996).
Alpha-fetoprotein (AFP) is a type of glycoprotein that is mainly produced in the liver and certain types of tumors, such as hepatocellular carcinoma (HCC), hepatoblastoma, and non-seminomatous germ-cell tumors. In adults, the normal level of AFP is typically less than or equal to 20 ng/mL. However, these levels can temporarily increase due to liver damage or when the liver is regenerating. If AFP levels remain elevated or continue to rise in individuals with chronic hepatitis or cirrhosis, it may indicate an increased likelihood of developing HCC. Although approximately 20% of HCC cases do not produce AFP, higher levels of AFP are often associated with larger tumors, less differentiated cells, and more aggressive cancer behavior. Despite this, the use of AFP in clinical practice is somewhat limited because not all tumors release this protein (Bérence Charrière, et al. 2016).
Models of hepatotoxicity
Fig. 5: Models of Hepatotoxicity
In vivo model of hepatotoxicity
Animal models are frequently used to assess hepatotoxicity because they can show complex interactions that occur within a living organism, how the body processes substances throughout the system, and the long-term impacts that cannot be observed in two-dimensional cell cultures. Because these models closely resemble human physiology, they offer useful predictions about how drugs will behave in humans, with preclinical research often accurately predicting about 70% of toxic effects seen in people. Liver injury models are especially important for understanding complicated biological processes like how drugs are broken down in the body and the body's immune reactions. The selection of an animal model depends on the goals of the study, the kind of liver damage being studied, and the properties of the drug under investigation. Rodents are often used because they are small, reproduce quickly, have a physiology similar to humans, and are easy to manage. However, other models such as primates, pigs, and rabbits may be used when they are more suitable. Additionally, models that have specific genetic backgrounds or disease conditions can be chosen to better match the needs of the experiment.
1] Acute damage (DILI) model:
Most medications are identified by the body as foreign materials, which leads to different chemical changes. These changes lower their ability to dissolve in fats and change how they work in the body, allowing them to be removed from the body (Tostmann A, et al. 2008). Drug-induced liver injury (DILI) is liver damage that happens as a side effect of taking drugs. It is often not recognized properly. DILI is a major reason why drug development projects are stopped, why warnings are issued after a drug is on the market, or why drugs are taken off the market. Globally, it affects about 14 to 19 people out of every 100,000 (Li X, Ni J, et al. 2023). Although DILI makes up less than 1% of all cases of acute liver injury (ALI), it is the most common cause of acute liver failure (ALF) in Europe, the United States, and Japan. Acetaminophen (APAP) is responsible for nearly half of these cases. Viral hepatitis (types A and B) and autoimmune hepatitis cause fewer cases. Since the liver plays a key role in breaking down drugs, it is especially sensitive to the effects of drugs, dietary supplements, and herbal products (Polson and Lee, et al. 2005).
2] Alcoholic liver disease (ALD) model
Excessive alcohol consumption is linked to hepatotoxicity, a significant global health issue (Lieber CS, et al. 1994). Alcoholic liver disease (ALD) is a long-term condition marked by liver damage caused by heavy drinking. A key factor in alcohol-induced liver damage is oxidative stress, which increases the activity of cytochrome P450 enzymes. These enzymes help break down not only alcohol but also other substances like acetaminophen. The process of metabolizing alcohol results in the formation of acetaldehyde, a harmful chemical that leads to a decrease in glutathione, damage to proteins, the production of free radicals, and the breakdown of lipids. These processes interfere with methionine metabolism, causing gradual and severe liver damage (Saukkonen JJ, et al. 2006). The progression of ALD involves several stages such as fatty liver, liver inflammation, fibrosis, and eventually cirrhosis. Therefore, assessing hepatotoxicity in ALD models is crucial for research in this area (Osna NA, et al. 2017).
One of the most commonly used models in ALD research is the chronic binge ethanol-feeding model in mice, which involves a special liquid diet called the Lieber–DeCarli diet. This model effectively mimics important aspects of ALD, such as increased blood alcohol levels, fatty changes in the liver, and liver damage. These changes can be observed as early as nine hours after alcohol is given (Wang D, et al. 2022).
3] MASLD/MASH model
Metabolic dysfunction–associated steatotic liver disease (MASLD) is one of the most common chronic liver diseases globally, and its prevalence is rising quickly, as shown by recent Global Burden of Disease data. A more serious form of MASLD is metabolic dysfunction–associated steatohepatitis (MASH), which involves inflammation and scarring of the liver, potentially leading to cirrhosis and hepatocellular carcinoma (HCC) (Eslam M, et al. 2020). Previously, MASLD was called non-alcoholic fatty liver disease (NAFLD), and MASH was referred to as non-alcoholic steatohepatitis (NASH). The new terms better represent the range of liver conditions caused by metabolic issues, including fat accumulation and inflammation. The causes of MASLD and MASH are complex, involving a mix of genetic, environmental, and metabolic factors (Suzuki-Kemuriyama N, et al. 2020).
4] Humanized model
Humanized animal liver models serve as essential tools for evaluating hepatotoxicity, as they help address differences in drug responses between species (Scheer N, et al. 2016). These models use immunodeficient animals with a reduced number of native liver cells, enabling the successful transplantation of human liver cells. This process creates liver tissue that closely resembles human liver function. Examples of commonly used models include uPA-SCID mice, which are useful for studying acute hepatotoxicity, and FRG mice, which are employed for chronic hepatotoxicity research. Another model, the TK-NOG mouse, is designed to specifically remove mouse liver cells, allowing for a high level of human hepatocyte engraftment. These mice also support the maintenance of essential liver functions such as drug metabolism and bile secretion (Ohshita H, et al. 2017). While animal models are useful for examining complex interactions that occur within a living organism and for predicting clinical outcomes, their interpretation is constrained by differences in anatomy, physiology, and metabolic processes between species. For example, a drug that is safe for humans may be harmful to mice. Additional challenges include ethical issues, the high cost of these models, the time required to conduct studies, and variability caused by stress. These factors make the use of animal models complicated. As a result, although animal models continue to play an important role in hepatotoxicity research, depending solely on them may not be enough. This highlights the need for alternative approaches, such as organoid-based testing (Hasegawa M, et al. 2011).
5] Herb induced liver injury (HILI)
Herbal hepatotoxicity, also known as herb-induced liver injury (HILI), is a condition that occurs when natural products consumed by humans cause damage to the liver. Herbs contain a variety of chemical compounds that can be beneficial when taken in the right amounts, but these same compounds may become harmful if consumed in large quantities. Many plants that contain these compounds have a strong, bitter, or unpleasant taste, which usually discourages herbivorous animals from eating them. However, humans often gather these plants for use in herbal remedies. Herbs can be used in their natural form, such as in teas or as food additives, or they can be processed into various products like herbal drugs and dietary supplements. While herbs and herbal products have traditionally been viewed as safe, recent studies show that they can lead to a range of adverse effects, some of which can affect multiple organs, including the liver (Woo SM, et al. 2021).
6] Chemical induce Hepatotoxicity
Xenobiotics are substances that are not typically produced or naturally found within the human body. People are frequently exposed to these compounds, and some have the ability to damage the liver. The most common way people come into contact with xenobiotics is by swallowing them, and the body absorbs them through the digestive system. Injury to the liver caused by chemicals often happens when a xenobiotic becomes activated in the body or when there is an imbalance between the processes that turn harmful substances into toxins and those that remove them. Breathing in or absorbing these harmful substances through the skin can also lead to liver damage (Hochstein C, et al. 2007).
Some liver-damaging substances are naturally found in foods or certain fruits, while others are created during food processing. Examples include fungal toxins like aflatoxin B1, which are often present in contaminated grains and nuts and can have serious effects on liver health (Williams DP, et al. 2002). One of the main causes of liver damage from chemicals is the dysfunction of mitochondria. When cells experience stress, a structure called the mitochondrial permeability transition pore (MPTP) can open, which rapidly increases the permeability of the inner mitochondrial membrane. Depending on how severe this change is, the membrane can allow harmful substances to escape, triggering programmed cell death (apoptosis) by releasing cytochrome c and activating caspases in the cell's fluid. In more severe cases, the mitochondrial membranes may completely break down, resulting in a loss of energy (ATP) and cell death through a process called necrosis. As a result, issues with mitochondria are a key factor in the development of liver damage caused by xenobiotics (Pessayre D, et al 2010).
Invitro model
The application of in vitro model systems in toxicity testing provides multiple benefits. These include a decrease in the number of animals needed, reduced costs for maintenance and care, the use of smaller amounts of chemicals, shorter time required for experiments, and a higher capacity to evaluate several chemicals and their metabolites.
In vitro systems also allow for the study of how chemicals are processed in the body, the exploration of how toxicity occurs, the measurement of enzyme activity, and the analysis of how the effect of a substance change with different doses. Moreover, these approaches help in understanding how cells react and how toxicity pathways work, identifying how chemicals cause harm, supporting large-scale testing, improving the accuracy of dose-response analysis, and enabling the testing of a broader range of chemical concentrations than is possible in live animals. These systems also make it possible to use exposure levels that are relevant to human health, assist in the development of models that predict how chemicals move through the body and how they affect it, and support research into how genetic factors influence toxic effects.
To overcome the shortcomings of traditional in vivo testing, the National Research Council suggested four main criteria for a new approach to toxicity testing. These involve expanding research to include a greater variety of chemicals, mixtures, health outcomes, and stages of life; reducing the time and financial resources needed for risk evaluation by making the process more efficient and adaptable; decreasing the number of animals used and the discomfort they experience; and improving understanding of the underlying processes and dosing effects to provide more detailed information for risk assessment organizations. High-throughput in vitro liver models are an important tool that can help achieve this change and encourage the wider adoption of alternative methods for toxicity testing.
1] Liver Slices
Liver tissue slices are a useful in vitro model because they retain the structural features of the liver, include all the types of cells found in the body, and closely resemble how the liver processes foreign substances in living organisms (Lerche-Langrand C, et al. 2000). These slices also preserve the specific enzyme activities found in different regions of the liver, enabling research into both general and regional toxic effects. In most studies, liver tissue slices are cultured for periods ranging from 30 minutes up to five days (Boess F, et al. 2003). To support the survival of cells and reduce harmful changes during this time, various factors such as oxygen levels, nutrient content, added substances, and the type of culture setup—like shaken flasks, multiwell plates, or stirred wells—have been carefully adjusted and improved.
Most available immortalized liver-derived cell lines do not fully represent the characteristics of normal liver tissue (Yu LJ, et al.2001). Commonly used immortalized hepatic cell lines include Fa2N-4, HepG2, Hep3B, PLC/PRF/5, Huh7, HBG, and HepaRG (Guguen-Guillouzo C, et al. 2010). Among these, the more recently developed human hepatoma cell line HepaRG maintains many liver-specific functions, such as the expression of several cytochrome P450 enzymes, nuclear receptors, membrane transporters, and Phase II enzymes. HepaRG cells have a stable karyotype, can differentiate into either hepatocyte or biliary cell types, and show a high capacity for proliferation. Additionally, they produce consistent and reliable data across different experiments, making them useful for studying hepatic toxicity (Aninat C, et al. 2006).
3] Three-dimensional Culture Systems
Three-dimensional hepatocyte culture is designed to mimic the liver's natural environment in the body, helping hepatocytes stay alive and perform their metabolic functions for a longer time compared to traditional two-dimensional methods. In standard 2D cultures, hepatocytes lose their ability to metabolize drugs within 24 to 48 hours (Meng Q, et al. 2010). Early three-dimensional spheroid models showed better development and kept cytochrome P450 expression higher, especially when there was enough oxygen available. To improve these models further, researchers developed gel-based systems using materials like alginate or agarose, and scaffold-based systems made from nanofibers or hollow fibres. These systems offer better support for cell structure and help maintain essential liver functions (Wu FJ, et al. 1996). Now, the focus is on making more sophisticated 3D liver models that closely copy interactions with the extracellular matrix and microcirculation. The aim is to create long-lasting functional models for use in toxicology and drug research, as well as for possible applications in bioartificial liver technology (Kim SS, et al. 1996)
|
|
|
4] Co-culture Systems
Hepatocyte co-cultures, which include hepatocytes alongside other liver or non-liver cell types, more effectively mimic the functions of the liver in living organisms compared to hepatocytes grown alone. When hepatocytes are co-cultured with fibroblasts, endothelial cells, or non-parenchymal cells such as Kupffer cells, stellate cells, and sinusoidal endothelial cells, their structural features, production of albumin and urea, cytochrome P450 (CYP) activity, and ability to metabolize drugs are significantly improved (Karam WG, et al. 1997). This enhancement results from both direct physical contact between cells and the release of soluble factors from the supporting cells. More sophisticated 3D co-culture systems, such as hepatocytes grown on micropatterned feeder layers, support long-term maintenance of liver-specific functions. These systems also allow for responses to inflammatory or chemical signals and offer more realistic models for assessing hepatotoxicity and studying drug metabolism (Talamini MA, et al. 1993).
Pharmacotherapy:
There is no single treatment that works for all cases of drug-induced liver injury (DILI) or DILI-related acute liver failure (ALF). The main approach is supportive care, focusing on managing complications like encephalopathy, coagulopathy, hypoglycaemia, infections, and kidney failure. Liver transplantation may be considered early in severe cases. N-acetylcysteine may help improve outcomes in cases of acetaminophen-induced ALF and some other non-acetaminophen-related ALF, but it is not always effective (Tujios SR, et al. 2018). Symptomatic treatments, such as bile acid sequestrants for cholestasis and antihistamines for itching, can offer relief. Hospitalization is necessary for patients whose liver injury is getting worse. It is important to report suspected cases to regulatory authorities to track drug safety and assist in possible regulatory decisions (Francis P, et al, 2025). For individuals experiencing hepatitis-like symptoms, all suspected drugs, chemicals, or toxins should be stopped, and liver function tests should be closely monitored. Treatment should be paused if levels of AST, ALT, or bilirubin are three times or higher than the upper limit of normal (ULN) and can only be resumed once these levels drop below this threshold. Mild symptoms with liver function tests (LFTs) should be carefully managed.
Hepatoprotective plants:
|
Sr.No |
Plant (Scientific / Common name) |
Part of Plant |
Family |
|
|
Silybum marianum (Milk thistle) |
Seeds |
Asteraceae |
|
|
Phyllanthus amarus |
Whole plant |
Phyllanthaceae |
|
|
Picrorhiza kurroa (Kutki) |
Rhizome |
Plantaginaceae |
|
|
Tinospora cordifolia (Giloy) |
Stem |
Menispermaceae |
|
|
Glycyrrhiza glabra (Licorice) |
Root |
Fabaceae |
|
|
Andrographis paniculata |
Leaves |
Acanthaceae |
|
|
Eclipta alba (Bhringaraj) |
Whole plant |
Asteraceae |
|
|
Azadirachta indica (Neem) |
Leaves / Bark |
Meliaceae |
|
|
Andrographis lineata |
Leaves |
Acanthaceae |
|
|
Careya arborea |
Bark |
Lecythidaceae |
|
|
Cassia fistula (Amaltas) |
Leaves |
Fabaceae |
|
|
Cleome viscosa |
Whole plant |
Cleomaceae |
|
|
Wedelia calendulacea |
Leaves |
Asteraceae |
|
|
Ixora coccinea |
Flowers / Leaves |
Rubiaceae |
|
|
Solanum nigrum (Black nightshade) |
Leaves / Berries |
Solanaceae |
|
|
Ginkgo biloba |
Leaves |
Ginkgoaceae |
|
|
Woodfordia fruticosa |
Flowers |
Lythraceae |
|
|
Thymus quinquecostatus |
Leaves |
Lamiaceae |
|
|
Terminalia arjuna |
Bark |
Combretaceae |
|
|
Trapa natans (Water chestnut) |
Fruit peel |
Lythraceae |
|
|
Vitex negundo |
Leaves |
Lamiaceae |
|
|
Ziziphus mauritiana |
Fruit / Leaves |
Rhamnaceae |
|
|
Ziziphus oenoplia |
Root |
Rhamnaceae |
|
|
Operculina turpethum |
Root / Whole plant |
Convolvulaceae |
|
|
Mimosa pudica |
Whole plant |
Fabaceae |
|
|
Lawsonia inermis |
Leaves |
Lythraceae |
|
|
Cajanus cajan |
Seeds / Leaves |
Fabaceae |
|
|
Ecbolium viride |
Root |
Acanthaceae |
|
|
Wissadula periplocifolia |
Whole plant |
Malvaceae |
|
|
Boerhaavia diffusa (Punarnava) |
Whole plant / Root |
Nyctaginaceae |
|
|
Curcuma longa (Turmeric) |
Rhizome |
Zingiberaceae |
|
|
Berberis aristata (Daruharidra) |
Root / Stem bark |
Berberidaceae |
|
|
Emblica officinalis (Amla) |
Fruit |
Phyllanthaceae |
|
|
Swertia chirayita (Chirayata) |
Whole plant |
Gentianaceae |
|
|
Aloe vera |
Leaves (gel / latex) |
Asphodelaceae |
|
|
Tephrosia purpurea (Sharpunkha) |
Whole plant |
Fabaceae |
|
|
Fumaria indica |
Whole plant |
Papaveraceae |
|
|
Ocimum sanctum (Tulsi) |
Leaves |
Lamiaceae |
|
|
Solanum xanthocarpum |
Whole plant / Fruit |
Solanaceae |
|
|
Butea monosperma (Palash) |
Flowers / Bark |
Fabaceae |
CONCLUSION:
Hepatotoxicity remains a major global health issue because it has many different causes, such as medications, chemicals, environmental toxins, alcohol, and herbal or dietary supplements. Drug-induced liver injury (DILI) is the most thoroughly studied cause of hepatotoxicity. Although it is uncommon, it is a major cause of acute liver failure, hospital admissions, and the withdrawal of medications from the market. Exposure to industrial chemicals, heavy metals, mycotoxins, and environmental toxins also leads to liver damage. These factors are especially significant in workplaces and in countries with less developed healthcare systems. The occurrence of liver toxicity varies depending on factors like region, age, sex, genetic background, and existing health conditions. Older adults and people who already have liver disease are more likely to experience liver damage. Detecting liver toxicity early through biomarkers, regularly monitoring high-risk groups, and improving reporting systems are essential to lower the number of serious health problems and deaths. Recent progress in laboratory and animal models has improved our understanding of how liver toxicity works and helps in creating safer medicines. In general, liver toxicity is a complex challenge for both doctors and public health officials, highlighting the importance of ongoing research, tracking, and prevention efforts to address this issue on a global scale.
REFERENCES



Saba Shaikh, Mahesh Manke, Madhuri Shinde, Smita Shirale, Padmaja Giram, Hepatotoxicity: Comprehensive Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 3634-3659. https://doi.org/10.5281/zenodo.20702148
 10.5281/zenodo.20702148
10.5281/zenodo.20702148