
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Senior Consultant Dermato - Venereologist, Department of Skin, STDs & Leprosy, KMCH Speciality Hospital Erode, Tamilnadu
Pyogenic granuloma, a misnomer now renamed as lobular capillary hemangioma is a common acquired benign vascular tumor of skin and mucosa. It can arise de novo or after trauma. PG occurs at any age, although it is seen more often in children and young adults. It is characterized by rapid growth and friable surface. Granuloma pyogenicum though not an infection can occur after use of drugs (oral / topical) which can be successfully treated with minimal recurrence. Surgical treatment is usually required because PG rarely resolves spontaneously and often bleeds repeatedly and profusely. Here we first describe a 38-year-old woman on treatment for skin ageing, hypothyroidism and hirsutism who developed pyogenic granuloma over face. Lesion was successfully removed using radiofrequency cautery. Recurrence was not noticed on 3 month follow up. Second case was a physician getting treated for obesity, acanthosis nigricans and impaired glucose tolerance developed granuloma pyogenicum over nape. It was removed using ablative Co2 laser with no recurrence for past 12 weeks.
Pyogenic granuloma, is a common, acquired, benign vascular tumor of skin and mucous membranes. It is now a days renamed as benign lobular capillary hemangioma (BLCH). Pyogenic granuloma (PG) occurs in patients of all ages, with a peak incidence in the second and third decades of life.1,2 Cause is still unknown. May be associated with keratinous cysts. Clinically it starts as a single erythematous pedunculated papule that is very friable and bleeds profusely on manipulation. Rarely it can occur as a solitary plaque. It grows rapidly and often undergoes surface ulceration. Most common site is in the oral cavity especially during pregnancy. Also seen over other sites. Various factors are implicated as etiopathogenesis but exact cause is unknown. Most theories on pathogenesis revolve around PG as a hyperplastic, neovascular response to an angiogenic stimulus with imbalance of promoters and inhibitors. Often reported in literature in association with drugs like oral contraceptive pills, oral or topical retinoids, levothyroxine. Here we describe two cases which we came across recently, first a 38-year-old woman on treatment for skin ageing, hypothyroidism and hirsutism who developed pyogenic granuloma over face and secondly a 32-year-old male physician on treatment for obesity, acanthosis nigricans and impaired glucose tolerance who developed granuloma pyogenicum over neck.
Case History
Case No 1
A 38-year-old house wife presented to our OPD with complaints of red sessile elevated lesion over cheek of 2 weeks duration. She was a known case of hypothyroidism on 100 mcgm of levo thyroxine along with oral contraceptive pills for hirsutism and irregular menstrual cycles. She is regularly using topical physical sunscreens and retinoic acid creams at night (thrice a week) as antiaging measures. Local examination showed fleshy red nodule of size 1.5 cm on the left cheek which readily bled profusely on manipulation. (Figure No1) It was excised by radio frequency cautery under local anesthesia. Excised specimen was sent for histopathological analysis which revealed under H & E stain lobular arrangement of capillary blood vessels and proliferating endothelial cells delineated by fibrous septae. (Figure No 2) Lesion was successfully removed using radiofrequency cautery. Recurrence was not noticed on 3 month follow up.
Case No 2
A 32-year-old physician presented with complaints of pink pedunculated lesion over nape for past 3 weeks which bleeds on manipulation. He was previously treated with topical timolol eye drops with no improvement. He was under treatment for obesity, acanthosis nigricans (12% ammonium lactate cream in morning and topical retinoic acid .05% cream / glycolic acid cream at night) and impaired glucose tolerance with drugs (Tab. Metformin 500 mgm B.D) and diet. Local cutaneous examination revealed non tender sessile dull pink nodule of size 1 cm over the nape of neck. (Figure No 3) It was removed by ablative Co2 laser under EMLA cream and the specimen was sent for pathological examination which revealed capillary hemangioma covered by squamous epithelium along with stromal edema and scattered inflammatory cells consistent with BLCH. (Figure No 4) Neither local recurrence nor nearby satellite lesions was observed even after 16 weeks of clinical follow up.
DISCUSSION
Granuloma pyogenicum or BLCH is commonly seen in second and third decades of life with female preponderance.3,4 Apart from trauma and irritation, drugs are implicated in gingival growth especially after the use of calcium channel blockers, calcineurin inhibitors, antiseizure medications or targeted anticancer medications (e.g. TNF alpha antagonists, BRAF inhibitors, tyrosine kinase inhibitors, epidermal growth factor receptor inhibitors, mTOR inhibitors, taxanes, pyrimidine analogs).5 There are reports of OCP causing pyogenic granuloma in the literature.6 Other medications also implicated include oral retinoids, HIV protease inhibitors like indinavir and immunosuppression. In our first case, patient was using thyroid replacement therapy, contraceptive pills, and topical retinoids all of which were implicated in the causation of this benign fleshy cutaneous tumor. Anti-cancer drugs like 5 Fluoracil or mitoxantrone are also implicated. Other multiple non drug precipitants including infectious organisms, eczematous dermatitis, penetrating or chronic injury have also been reported. Differential diagnosis clinically includes amelanotic melanoma, squamous cell carcinoma, angiosarcoma, Kaposi sarcoma, hemangioma, bacillary angiomatosis, metastatic visceral malignancies, and granulation tissue based on history and location. 7 Histopathology is often classical with small capillaries with variable luminal diameters in an oedematous stroma with scattered inflammatory cells. In our first case, topical retinoids and in our second case, topical retinoids could be one of the perpetuating reason apart from others like minimal irritation from hair cut / shaving and tulsi mala around the neck (friction from beads in a sweat retention area)which the person started using during recent times. Trauma, irritation, and drugs can be the collective reasons for the occurrence of this vascular neoplasm. No recurrence was noted in both cases till date.
CONCLUSION
Despite its name, a pyogenic granuloma is not a true granuloma, nor is it pyogenic, in that it does not produce pus. This benign vascular neoplasm appearing as papulonodular lesions over face, trunk and extremities is often indistinguishable from true hemangiomas microscopically. The clinical diagnosis can be quite difficult, as they can mimic more serious lesions, such as malignancies.

Figure No 1 : Pyogenic granuloma bleeding on manipulation over left cheek
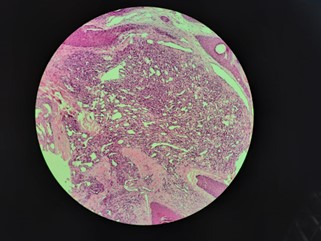
Figure No 2 : HPE / H& E stain depicting lobular arrangement of capillary blood vessels and proliferating endothelial cells delineated by fibrous septa

Figure No 3: Pyogenic granuloma over nape of neck decorated with tulsi mala
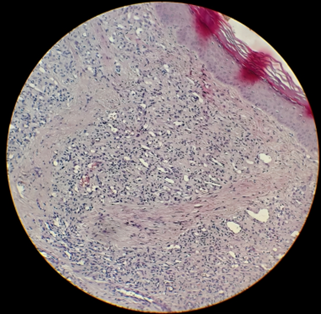
Figure No 4 : HPE / H& E stain showing capillary hemangioma covered by squamous epithelium along with stromal edema and scattered inflammatory cells
DECLARATION OF PATIENT CONSENT
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
FINANCIAL SUPPORT AND SPONSORSHIP
Nil
CONFLICTS OF INTEREST
There are no conflicts of interest
REFERENCES

Rajesh Rajagopalan, Drug Induced Lobular Capillary Hemangioma-Uncommon Presentation (Site) Of A Common Disease - Case Series, Int. J. of Pharm. Sci., 2024, Vol 2, Issue 4, 843-847. https://doi.org/10.5281/zenodo.11000354
 10.5281/zenodo.11000354
10.5281/zenodo.11000354