
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1 SBS College of Pharmacy, Patti, Punjab, India.
2 Department of Pharmacy Practice, Sri Indu Institute of pharmacy, Sheriguda, Ibrahimpatnam(M)R.R. 501510.
3,4 Maharaja Jitendra Narayan Medical College and Hospital, Coochbehar-736101, West Bengal, India.
5 Annai Veilankanni's College of Pharmacy, Chennai-15, India.
6 Department of Radiology, Mahatma Gandhi Medical College, Jaipur, India.
Neurodegenerative and neurological diseases represent a significant and growing global health burden, which is largely due to the demographic (population age) and lack of disease-modifying treatment. The traditional oral neuroprotective drugs are often limited by the low permeability of the blood-brain barrier, first-pass metabolism, systemic side effects, and polypharmacy and pill burden, especially in the geriatric population. These shortcomings underscore the necessity of different, patient-friendly methods of drug delivery, which may be used to promote central nervous system targeting with reduced systemic exposure. Nose-to-brain intranasal delivery has become an encouraging non-invasive method that permits direct delivery of therapeutic agents into the brain by taking olfactory and trigeminal neural routes, avoiding the blood-brain barrier. This is a critical review on the anatomical and physiological basis of nasal drug delivery, the mechanism behind neuronal and extra-cellular delivery as well as more advanced formulation technology such as mucoadhesive system, in situ gel and nanotechnology based carriers. Its use in significant neurological diseases, such as Alzheimer disease, brain tumors, Multiple sclerosis, Parkinson disease, epilepsy, stroke, and epilepsy, is also discussed as a basis of translational relevance. There are also contemporary issues of mucocillar clearance, dosing volume, enzyme degradation and control that are discussed. Together, intranasal delivery is a disruptive approach that can help decrease the pill burden, increase adherence to patients, and increase targeted therapy in neuroprotection. Further interdisciplinary studies and clinical confirmation are necessary to fully achieve its effect in modern CNS pharmacotherapy.
Neurodegenerative diseases are heterogeneous chronic progressive disorders with the selective destruction of structure and function of neurons of the central and peripheral nervous systems. These are characterized by progressive neuronal impairment, synaptic dysfunction and eventual cell death which causes an irreversible loss of cognitive, movement, behavioral and autonomic functions. In contrast to acute neurological injuries, neurodegenerative diseases progress in a years or decades, which indicates complex and multifactorial pathogenic processes rather than one-factor affective events. Some of the most common forms of neurodegenerative disorders are the Alzheimer and the Parkinson disease that both are more common in the older adults [1]. Alzheimer disease is clinically presented as progressive memory loss, executive dysfunction, and behavioral disturbance and pathologically manifested through extracellular deposition of amyloid-b plaques and intracellular neurofibrillary tangles formed by hyperphosphorylated tau protein [2]. Parkinson disease, conversely, is characterized by greater involvement of motor functioning and is related to the destruction of dopaminergic neurons in the substantia nigra pars compacta and the deposition of a-synuclein-containing Lewy bodies. Other major neurodegenerative diseases are the Amyotrophic lateral sclerosis, which causes progressive muscle weakness as a result of motor neuron degeneration, Huntington disease, a hereditary disease that is associated with choreiform movements and psychiatric symptoms, and Multiple sclerosis, a combination of inflammatory demyelination and neuroaxonal loss. Despite the differences in the clinical manifestation and anatomical location, these disorders have a number of common molecular and cellular processes [3]. Protein misfolding and aggregation are major pathogenic aspects in most neurodegenerative diseases. Protein accumulation abnormalities in proteins include amyloid-b, tau, a-synuclein, and mutant huntingtin that interfere with cellular homeostasis, impairs proteasomal and autophagic degradation, and stimulate neuroinflammation. Another typical hallmark is oxidative stress, which is caused by an overproduction of reactive oxygen species and a malfunctioning antioxidant defense mechanism. Mitochondrial impairment is an additional risk factor that contributes to the susceptibility of neurons through disturbing energy breakdown and successful induction of apoptotic cascades [4-6]. A chronic neuroinflammation is also relevant in the development of the disease. Pro-inflammatory cytokines, chemokines, and reactive nitrogen species are released by activated microglia and astrocytes and facilitate the dysfunction of synapses and neuronal damage. Although acute inflammation can have a protective effect, chronic activation of the microenvironment produces an adverse environment that enhances neurodegeneration [7]. Also, excitotoxicity through the overstimulation of glutamate produces calcium overload, enzymatic activation and cell death. Different disorders have a varied contribution of genetic and environmental factors. Some of the conditions, including Huntington disease, are clearly autosomal dominant in their pattern of inheritance, and most incidences of Alzheimer and Parkinson diseases are sporadic, with complicated interactions of the genetic susceptibility loci with environmental exposures. The greatest risk factor is aging, which indicates a cumulative molecular damage, a degradation of proteostatic processes, and a deterioration of the cellular repair systems with age [8]. Neurodegenerative diseases have a progressive symptomology in their clinical presentation. The initial symptoms can be minor, such as mild cognitive impairment, slight shakes, or mood swings. The progression of neuronal loss results in a decrease in functional independence and the need to provide long-term medical and supportive care. Notably, neurodegeneration is not usually reversible; neurons of the adult central nervous system possess a limited regenerative ability, which explains the relevance of early diagnosis and neuroprotective approaches. Diagnosis is commonly based on clinical examination with the help of neuroimaging, cerebrospinal fluid biomarkers, and genetic testing in the appropriate cases [9]. The improved development of molecular imaging and finding of biomarkers has enhanced the detection and monitoring of the disease at an early stage but has yet to provide silver bullets. The existing treatment methods are rather symptomatic. An example of such is the cholinesterase inhibitors and NMDA receptor antagonists that are used in the treatment of Alzheimer disease to temporarily improve the cognitive ability, and the dopaminergic therapies that are used in the treatment of Parkinson disease to treat motor symptoms [10]. Treatments that are disease-modifying in order to prevent or reverse neuronal loss are highly researched but have so far not been so successful. Neurodegenerative diseases are a global burden that is becoming more and more dramatic as a result of the demographic aging. These conditions have far reaching socioeconomic implications such as direct healthcare spending, institutional care cost, burden on the caretaker, and productivity loss. Outside of economic factors, the emotional and psychological burden on patients and families is massive, as it influences the quality of life and well-being in the society [11-13].
1.1. Global burden of neurodegenerative disorders
Neurodegenerative diseases are an ever-growing health issue in the world that is mainly caused by ageing of the population and longer lives. Progressive neuronal dysfunction and neural tissue irreversible loss are noted to characterize these conditions and result in cognitive, motor, and behavioral impairments. The most common of them are Alzheimer and Parkinson diseases which together contribute a significant percentage of the global neurological disability [14]. Alzheimer disease is the most common cause of dementia and it leads to most cases of dementia worldwide and the second most prevalent neurodegenerative disease is Parkinson disease which is on the increase in both developed and developing countries. It is estimated that the epidemiological burden of these diseases will be tremendous in the next several decades. The most important risk factor is aging, and demographic shifts to the aged have increased prevalence rates in all continents [15]. African countries, both low and middle-income, are already witnessing a significant increase in the number of affected people, which they have not been able to accompany by expansion of health facilities capable of caring with chronic neurological conditions. As a result, the issues of inequalities in the diagnosis, access to treatment, and the provision of long-term support are becoming more apparent. In addition to prevalence, the social economic impact of neurodegenerative disorders is tremendous. Direct medical expenses comprise pharmacotherapy over a long period, hospitalization, diagnostic assessment, rehabilitation care and institutional care. Indirect costs like the loss of productivity, absenteeism of the care givers and early deaths of the individuals are usually greater than the direct healthcare expenses [16-18]. Family members taking care of a patient often play a major but often underestimated role in the economic burden, and the emotional and psychological implications may be significant. The effect of neurodegenerative diseases is more than just a financial aspect. Behavioral disturbances, motor impairment and progressive cognitive decline significantly decrease quality of life and functional independence. The patients often need the help in their activities of everyday living, which contributes to higher levels of dependency and social isolation. There are high stress, depression, and burnouts among caregivers which deteriorate the societal bearing [19]. In addition, neurodegenerative diseases are related to the high morbidity and mortality rates. There are complications like aspiration pneumonia, falls, infections and cardiovascular comorbidities that result in higher rates of hospitalization and mortality. Because the therapeutic treatments are mostly palliative as opposed to curative, progression of the disease goes on despite therapeutic measures. To conclude, neurodegenerative diseases create a growing international burden that includes both medical, financial, and psychosocial aspects. The coming together of the aging populations and the low disease-modifying therapeutics have highlighted the significance of newer approaches in prevention and early diagnosis and targeted delivery of therapies to reduce the increasing burden on the populations and health care systems across the globe [20-22].
1.2. Limitations of conventional oral neuroprotective therapies
The traditional oral neuroprotective interventions have been the dominant treatment of most neurodegenerative conditions but its use is limited in clinical settings by various pharmacokinetic, pharmacodynamic, and patient factors. Poor and erratic bioavailability is one of the major challenges [23]. Upon oral delivery, the drug has to be dissolved in the gastrointestinal tract, absorbed across the intestinal epithelial cell layer, and subsequently pass through hepatic first-pass metabolism, before entering into the general circulation. The solubility of many neuroprotective agents in aqueous fluids is low or the intestinal permeability is low, leading to unpredictable plasma levels. Moreover, a high amount of hepatic metabolism may decrease considerably the proportion of active drug available to produce central effects. A more severe constraint in the case of central nervous system (CNS) diseases is the availability of blood-brain barrier (BBB) [24]. The BBB is an extremely discriminative physiological interface, which is made up of tight junctions, efflux transporters, and metabolic enzymes limiting the access of the majority of therapeutic molecules into the brain. As a result, only a low percentage of the orally delivered neuroprotective drugs get into the target site at therapeutically significant concentrations. Greater systemic dose is necessary to compensate, and more risky is peripheral adverse effects including gastrointestinal disturbances, cardiovascular complications and hepatotoxicity [25]. The side effects are often a reason to either change the dose or stop the treatment. Alzheimer disease and Parkinson disease are chronic forms of neurodegeneration, which normally involve long-term or lifelong pharmacotherapy. Oral prolonged administration may result in accumulative toxicity and pharmacokinetic variability especially in older patients who are often characterised by variations in the gastric pH, hepatic metabolism and renal clearance [26]. Also, polypharmacy increases the occurrence of drug-drug interactions because most of the patients are taking of drugs simultaneously since they have comorbid conditions like hypertension, diabetes, and depression. Delay in onset of action is another issue of concern. Oral preparations rely on absorption of the gastrointestinal tract, which is affected by the food intake, guntric emptying period, and the motility of the intestines [27]. This inconsistency restricts their applicability in situations where there is need to provide neuroprotection or control acute symptoms in a short time. In addition, biologic therapeutics including peptides, proteins, and nucleic acid-based therapeutics are not suitable to oral delivery because they are highly enzyme-sensitive and do not have high membrane permeability.
1.3. Anatomy and physiology of the nasal cavity relevant to brain targeting
The nasal cavity is a distinct anatomy of the interface between the outside world and the central nervous system (CNS), which provides a non-invasive pathway of direct drug delivery to the brain. Its structural organization, vascularization and neural connectivity give it a scientific basis on why nose-to-brain targeting delivery systems are designed. The rational design of neurotherapeutic formulations therefore requires knowledge of the anatomical and physiological nature of the nasal cavity [28]. The nasal cavity can be sub-subdivided into three primary parts, including the vestibular region, the respiratory one, and the olfactory region, which are functionally separated by the nasal septum, which divides two symmetrical chambers of the nasal cavity. Regions vary in terms of epithelial structure, surface area, blood supply, and functional purpose of absorption and transportation of drugs. The vestibular area, which is right behind the nostrils, is purely protective in nature. It is lined with stratified squamous epithelial and it has vibrissae (nasal hairs), sebaceous glands, and cells that produce mucus. Even though this area does not contribute much to the systemic absorption of drugs because of its comparatively low surface area and the presence of keratinized epithelium, it determines the formulation deposition and retention when drugs are delivered intranasally [29]. The respiratory region forms the biggest part of the nasal cavity with almost 70-80 percent of total surface area. It is coated with pseudostratified columnar ciliated epithelium mixed with goblet cells which secrete a mucus. The lamina propria is very vascularized, and there is a wide range of blood vessels that allows drugs to be absorbed readily into the system. Tight junctions also control paracellular permeability through respiratory epithelium. Although this area is the main contributor to the overall uptake of drugs, it also aids in the process of brain targeting by allowing the trigeminal nerve pathways to be accessed. This area has a specialised olfactory epithelium which constitutes olfactory receptor neurons, sustentacular (supporting) cells, basal cells, and Bowmans glands. The olfactory epithelium has direct neuronal connections with the brain through the olfactory bulb unlike other epithelial tissues. The axons of olfactory neurons cross the cribriform plate to connect in the olfactory bulb forming a direct anatomical connection between the nasal cavity and the CNS [30]. This special route enables the therapeutic agents to by-pass the blood-brain barrier (BBB) and target central structures via intracellular axonal transport or extracellular diffusion through perineural pathways. The other route of CNS access is through the olfactory pathway besides the trigeminal nerve. The trigeminal nerve has branches that serve the respiratory/olfactory areas and send to the brainstem and other central areas. Drugs in nasal cavity can take advantage of these circuits and access more profound brain circuits increasing the scope of the distribution beyond the olfactory bulb. Physiologically, the nasal cavity also plays critical roles such as air filtration, humidification and temperature control. They are aided by mucociliary clearance, which is a defense mechanism whereby mucus sticks to the inhaled particles and coordinated ciliary motion is used to propel the mucus layer to the nasopharynx where they are eliminated [31]. Although defensive, mucociliary clearance presents a challenge to the delivery of intranasal drugs; it reduces the residence time and diminishes the absorption rate. Mucoadhesive polymers and agents that increase viscosity tends to be used as formulation strategies to increase the time of nasal retention and uptake of drug. This is due to the fact that, nasal mucosa is relatively permeable to other epithelial tissues, with its thin lining of the epithelial barrier and extensive vascularity. The presence of proteases as well as other metabolic enzymes in the nasal cavity together with the presence of enzymatic activity can affect the stability of some therapeutic molecules especially those that are peptides and proteins. Nonetheless, nasal enzymatic degradation is not as extensive as gastrointestinal or hepatic metabolism and thus, certain classes of drugs are better bioavailable [32]. The other physiological issue of concern is the small volume of administration which is normally limited to 100-200 uL per nostril in adults. Operating with excess could create a runoff, swallowing or lower deposition efficiency. Thus, effective nose-to-brain delivery preferably is done by highly potent drugs or concentrated formulations.
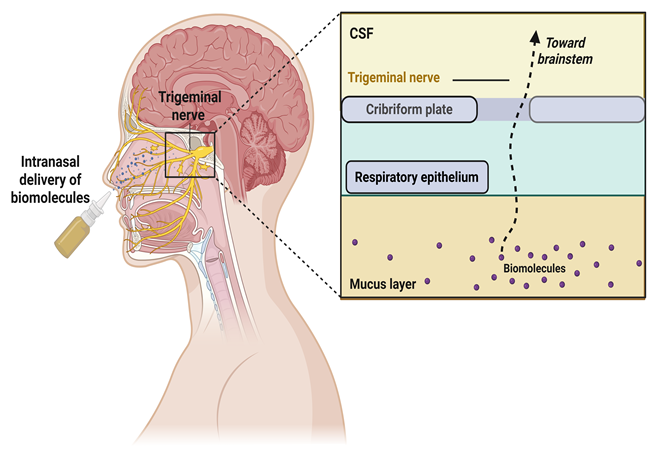
Fig.1: Intranasal delivery of biomolecules via the trigeminal nerve
2. Mechanisms of nose-to-brain transport
Nose-to-brain delivery is a unique and non-invasive route of delivering therapeutic agents to the central nervous system (CNS) bypassing blood-brain barrier (BBB). The processes that govern this transport are complicated and comprise of a complex of neuronal, extracellular, vascular, and lymphatic processes [33]. After an intranasal route, the drug molecules that have accumulated in the nasal tract, especially in the olfactory and respiratory areas, have the opportunity to reach the brain via anatomically coupled neurons, mainly olfactory and trigeminal nerves. These vascular connections allow direct contact between the nasal mucosa and different parts of the brain, allowing fast central delivery without a large systemic circulation. Intracellular neuronal transport is one of the major processes of nose-to-brain transportation [34]. In this pathway, the drug molecules are taken into the olfactory receptor neurons via endocytosis followed by transportation via axons through axonal transport systems. These neurons have their axons run through the cribriform plate into the olfactory bulb so that the substances can get directly into the central structures. The axonal transportation may be through slow or fast transport system according to the molecular properties of the therapeutic agent. Intracellular transport, though rather slow in comparison with extracellular diffusion, allows delivering the specified part of the brain and could be especially applicable to macromolecules, including peptides, proteins, and some nanoparticles. Along with the intracellular transport, extracellular or paracellular diffusion is important [35]. Intranasal deposition of drugs leads to the diffusion of the drug through the intercellular spaces of the olfactory epithelium to the lamina propria. There they can take the possible pathways of the perineural routes of olfactory nerve bundles into the subarachnoid space and cerebrospinal fluid (CSF). Such extracellular pathway is usually much more rapid than axonal transport and is said to be a significant factor in the onset of action seen with certain intrinasally delivered agents. This pathway can be used by lipophilic molecules and small hydrophilic compounds based on their physicochemical properties and formulation attributes [36].
3. Advantages of intranasal delivery in neuroprotection
Intranasal delivery has also become a promising approach in neuroprotection because of the ability to get direct access to the central nervous system (CNS) with a low systemic exposure. The biggest benefit of this pathway is that it bypasses the blood-brain barrier (BBB), which is an extremely selective physiological interface that limits the uptake of the majority of therapeutic agents into the brain. Under traditional systemic delivery, especially orally, a very low percentage of the dose administered usually attains the CNS, which demands increased systemic levels potentially causing peripheral side effects. Contrastingly, intranasal delivery enables the access of the drugs in the brain through olfactory and trigeminal neural routes and results in increased bioavailability in the central nervous system without necessitating a high dosing. The fast action is also another major benefit [37]. Intranasally delivered drugs reach the brain in just under minutes via extra-cellular diffusion and perineural transport systems. This fast pharmacokinetic data is especially useful when it comes to acute neurological events like seizure attacks, ischemic stroke, or even spontaneous progression of neurodegenerative symptoms where neuroprotection is paramount. The direct transport routes relieve the use of the systemic circulation and offer a rapid therapeutic intervention in comparison to the oral or even some parenteral paths [38]. There is also intranasal delivery, which is not degraded in the gastrointestinal tract or metabolised in the liver. Most neuroprotective substances, particularly peptides, proteins and some small molecules are also unstable in the gastrointestinal tract because of enzyme degradation as well as because of acidic environments. Also, there is a possibility that hepatic metabolism may decrease the bioavailable fraction of orally administered drugs to a significant degree. These barriers can be overcome by intranasal administration to enhance the stability of drugs and the percentage of active compound getting to the target site. This attribute is especially beneficial to up-coming biologic therapies, such as neurotrophic factors and RNA based therapies, which can not be administered orally. Another significant advantage is diminished exposure of the system [39]. Due to the ability of intranasal delivery to attain therapeutic concentrations in the brain of lower total doses overall risk of systemic side effects is reduced. This is particularly applicable among the elderly groups with neurodegenerative diseases like the Alzheimer disease and the Parkinson disease who in most cases have multiple comorbidities and are prone to adverse drug reactions. Systemic distribution minimization can not only improve the safety but also decrease that possibility of drug-drug interactions in patients with polypharmacy [40]. Other benefits of the intranasal route include patient compliance and convenience. Long-term therapy with neuroprotective drugs is often chronic, and oral doses can be taken with several doses per day. Naresal preparations, especially sustained-release or retention preparations, could lower the frequency of dosing and the overall pill burden. This is especially useful by those who are cognitively impaired, dysphagic, or motorically disabled so that swallowing of tablets may be difficult. Painless self administration without need of invasive procedures also enhances better patient acceptance and could lead to higher compliance of the given regimens.
The vascularization of the nose is rather high and the permeability is quite big, which helps to absorb drugs easily. Intranasal delivery has a greater surface area of absorption and greater anatomical accessibility to the brain, relative to transdermal or any other non-invasive route. Further improvements in formulation technologies (mucoadhesive polymers, nano-carriers and in situ gelling systems) increase the nasal residence time and permeability to overcome physiological barriers to diffusion, like mucociliary clearance. Through these technological advances, it is possible to deliver therapeutic intervention in a controlled and targeted manner to maximize therapeutic results. The other factor to be considered is versatility of intranasal delivery systems. Numerous therapeutic agents, such as small molecules, peptides, proteins, vaccines, and nanoparticles, can be modified to be delivered by nose with proper formulation plans. This flexibility underpins the translation research towards disease-modifying therapy of complicated neurodegenerative diseases. With the development of knowledge regarding CNS pathophysiology, intranasal delivery systems offer scalability and flexibility to administration of next-generation therapeutics [41].
4. Formulation strategies for nose-to-brain delivery
The rational formulation design is a cornerstone to the successful translation of nose-to-brain drug delivery systems into clinical practice. Although the nasal cavity provides anatomical routes directly to the central nervous system (CNS), physiological restrictions like mucociliary clearance, dose volume limitation, enzyme degradation, and unpredictable permeability demand maximum efficacy pharmaceutical approaches. The formulation methods should thus increase the drug solubility, extend the nasal residence time, ease the epithelial permeation process, shield labile molecules and targeted delivery to CNS. Designing the efficient intranasal systems incorporates the concepts of pharmaceutics, nanotechnology, polymer science and molecular targeting. The main formulation strategies used in nose-to-brain delivery are described as follows.
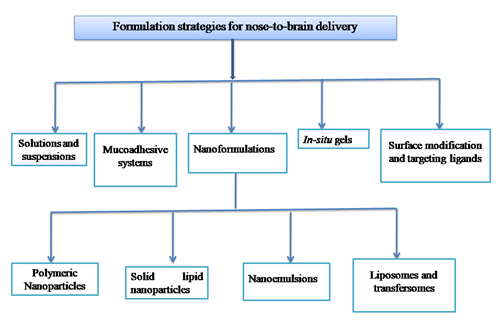
Fig.2: Formulation strategies for nose-to-brain delivery
4.1. Solutions and suspensions
Simplest and commonest type of formulation used in the intranasal drug delivery is nasal solutions. These systems include drugs suspended as a solution in aqueous or hydroalcoholic vehicles which are usually buffered to physiological pH and physiological isotonicity to reduce mucosal irritation. Some of the benefits associated with solutions are that they are easy to manufacture, uniform in their dosing, quick in their effect, and that they are highly acceptable by patients. Due to the dissolved state of the drug, it may be absorbed instantly upon contact with the nasal epithelium, and may be transported quickly through the olfactory and trigeminal routes. Naresal solutions are, however, constrained by short residence time owing to clearance by the mucocilia which have the ability of clearing the deposited drug in 15-30 minutes. This limitation usually creates partial absorption and low bioavailability. Moreover, drugs with low solubility in water may have formulation problems, and solubilising agents, co-solvents, cyclodextrins or surfactants will need use. One should take care to make sure that the excipients do not affect the epithelial integrity or result in irritations. The nasal suspensions are used where the active pharmaceutical ingredient is a compound with a low aqueous solubility. Under such systems, micronized or nanosized particles of drugs are suspended in an appropriate vehicle. Suspensions can offer long-term dissolution and mucosal contact as opposed to solutions. The size of the particle is also important, the smaller it is, the more surface area and the higher the rate of dissolution, the better the absorption. However, other significant formulation concerns include sedimentation, dose uniformity, and the stability of the physical formulation. Even though the solutions and suspensions are comparatively straightforward systems, the targeting of the brain can be greatly improved by the addition of absorption enhancers or mucoadhesive agents to the system [42].
4.2. Mucoadhesive systems
Mucoadhesive formulations are formulated to increase the residence time of drugs in the nasal cavity by increasing adhesion to the nasal mucosal surface. This method is used as a counter to one of the main weaknesses of intranasal delivery rapid mucociliary clearance. Mucoadhesive systems increase the amount of time that the formulation is in touch with the epithelial membrane to increase drug absorption and improve the efficacy of nose-to-brain delivery. Mucoadhesion is realized with the help of polymers that are able to establish non-covalent interactions with mucin glycoproteins in the mucus layer, i.e., hydrogen bonding, electrostatic attraction, or van der Waals forces. Popular mucoadhesive polymers are chitosan, carbopol, hyaluronic acid, hydroxypropyl methylcellulose (HPMC) and sodium alginate. Chitosan is of particular interest because it has both mucoadhesive and permeation enhancing properties and can transiently open tight junctions to enable paracellular transport. Mucoadhesive systems may be structured in form of a gel, powder, microspheres or nanoparticle coating. They decrease the loss of drugs by draining or swallowing, thereby enhancing bioavailability and can allow a reduction in dose. Nonetheless, very high viscosity could affect sprayability and comfort to patients. Formulation optimization consequently involves the necessity to balance between mucoadhesion and ease of administration and tolerance to mucosal [43].
4.3. In situ gels
In situ gelling systems are a novel way of nasal formulation, in which a low-viscosity liquid is gelled on exposure to physiological stimuli in the nasal cavity. These stimuli can be temperature, pH and ionic composition. Thermosensitive polymers e.g. poloxamers (e.g. Poloxamer 407) exist as liquids at room temperature, but as semi-solid gels at nasal temperature (32-34degC). Likewise, pH-sensitive polymers and ion-activated systems (e.g. gellan gum) can also undergo sol-gel transitions when in contact with nasal mucosa. The main benefit of in situ gels is that they allow them to combine easy administration and lasting retention. Accurate dosing and uniform distribution is possible with the first liquid state, and then the formation of gel decreases mucociliary clearance and maintains drug release. This method improves bioavailability and possibly controlled or gradual delivery into the brain. The in situ gels are especially useful in the delivery of peptides, proteins and nano-carriers, because the gel structure is able to protect the labile molecules against enzyme degradation. In addition, the use of mucoadhesive polymers in in situ systems, adds on mucosal interaction. Although they possess such benefits, gel strength, rheological behavior and reversibility should be critically evaluated to provide patient comfort and predictable release profile of the drug [44].
4.4. Nanoformulations
Nanotechnology-based systems have revolutionized nose-to-brain delivery by enabling improved solubility, stability, permeability, and targeting efficiency. Nanoformulations typically range from 10 to 500 nm in size and can traverse biological barriers more effectively than conventional formulations. They protect encapsulated drugs from enzymatic degradation, enhance epithelial penetration, and allow surface functionalization for targeted delivery.
4.4.1. Polymeric Nanoparticles
Colloidal carriers made of biodegradable polymer (poly(lactic-co-glycolic acid) (PLGA), chitosan, or polycaprolactone are known as polymeric nanoparticles. Drugs can be incorporated in the polymer matrix (nanospheres) onto a central location with a polymer surrounding it (nanocapsules). The systems have the benefits of controlled-drug release, degradation protection, and uptake improvement through endocytosis. Nanoparticles made of chitosan are especially beneficial in intranasal delivery because of their mucoadhesive and permeability-increasing characteristics. The nanoparticles can be designed as polymeric nanoparticles to control size, surface charge and hydrophobicity and hence their interaction with the nasal epithelium and neuronal pathways. Polymeric matrix release controlled by the neuroprotective effect promotes continuous action at reduced dosing rate [45].
4.4.2. Solid lipid nanoparticles
Solid lipid nanoparticles (SLNs) are biocompatible lipids in the solid physiologic temperature, which are stabilized by surfactants. These carriers have the benefit of polymeric nanoparticles off-set by enhanced biocompatibility and decreased cytotoxicity. SLNs offer protection against degradation, high drug loading when working with lipophilic compounds and controlled release. SLNs increase permeability in nose-to-brain delivery and could be used to achieve transcellular delivery across epithelial membranes. They have a lipid composition that allows them to interact with biological membranes and could enhance neuronal uptake. Nevertheless, issues like expulsion of the drugs during the storage period and high loading capacity of hydrophilic drugs necessitate optimization of the formulation [46].
4.4.3. Nanoemulsions
Nanoemulsions are kinetically stable or thermodynamically stable colloidal dispensations of oil and water that is stabilized by surfactants and whose droplet sizes are generally less than 200 nm. These systems improve solubilization of lipophilic drugs and result in quick absorption because of the small droplet size and a large surface area. When used as intranasal agent delivery vehicles, nanoemulsions enhance mucosal delivery and have the potential to enhance the diffusion of drug through epithelial membranes. They are also scalable easily and comparably easy to manufacture as compared to other nanocarriers. Nevertheless, the concentration of the surfactant should be thoroughly regulated so that the mucosal irritation should not occur [47].
4.4.4. Liposomes and transfersomes
Liposomes are vesicles, which consist of phospholipids bilayers, which contain aqueous cores. They can also hold hydrophilic and lipophilic drugs and they are highly biocompatible. In obstetric membranes, liposomes encourage biolysis of entrapped agents, and have the ability to merge with biological membranes. Transfersomes are very deformable vesicles that have edge activators that increase flexibility of the membranes. They are deformable and can penetrate through small intercellular spaces thus enhancing the efficiency of penetration. Liposomes and transfersomes can be targeted with ligands in order to make them brain-specific. However, the problem of stability, scalability, as well as cost, leaves much to be desired in wide-scale clinical application [48].
4.5. Surface modification and targeting ligands
The strategies of surface modification are directed at increasing the specificity and effectiveness of nose-to-brain delivery systems. Neuronal uptake and receptor-mediated endocytosis can be facilitated by targeting nanoparticles with targeting ligands, including peptides, antibodies, lectins, or transferrin. These ligands bind with receptors on the epithelial cells of the nose or on the neurons on the membranes where they bind selective transportation. PEGylation (polyethylene glycol coating) is usually employed to enhance stability, aggregation, and retention by the mucosa. Also, lectin-functionalized systems may take advantage of carbohydrate-binding of the mucosal surfaces, which increases adhesion and delivery. Targeted nano-carriers are a complex form of precision neurotherapeutics, which allows delivering a carrier to a particular brain area or pathology. Although small-scale studies have been encouraging, preclinical trials are faced by translational issues, such as immunogenicity, scale production, and regulatory aspects [49].
5. Neuroprotective agents explored via intranasal route
The use of intranasal delivery has been widely studied with regards to a wide range of neuroprotective agents to achieve an improvement in the bioavailability of the central nervous system (CNS) with decreased systemic exposure. Biologics and small-molecule drugs have shown potential promise in translation by using the nose-to-brain route. Within the neurodegenerative diseases like Alzheimer's disease and Parkinson, some categories of therapeutic agents have been researched in an effort to control underlying processes including oxidative stress, neuroinflammation, excitotoxicity, mitochondrial dysfunction, and protein aggregation. One of the most significant groups of neuroprotective agents delivered by way of inhalation is represented by peptides and proteins. Insulin nasally has been investigated as a cognitive-enhancing and neuroprotective agent, especially in Alzheimer disease because of the ability to regulate synaptic plasticity and neuronal survival pathways. On the same note, neurotrophic factors, including nerve growth factor (NGF) and brain-derived neurotrophic factor (BDNF), have also been tested as being able to assist in neuronal regeneration and decrease in apoptosis. Since these biologics are prone to enzymatic degradation and have low blood-brain barrier permeability in a systemic route, an alternative non-invasive route is intranasal. There has also been extensive research on small-molecule therapeutics. Dopamine and dopamine agonists have been developed as intranasally administered preparations in the treatment of Parkinsonism as a way to enhance brain delivery directly and minimize peripheral adverse events of oral administration. Curcumin, resveratrol, and quercetin are the antioxidants that were studied regarding their ability to reduce oxidative stress and neuroinflammation. Equally, anti-inflammatory drugs and glutamate receptor modulators have also been investigated to lessen the excitotoxic injury in stroke and epilepsy, among others. Plant-derived compounds and phytoconstituents have received interest because they possess multimodal neuroprotective activity. The objective of intranasal herbal extracts/ bioactive phytochemicals formulations is to maximize their antioxidant and anti-inflammatory properties by addressing the issues of low oral bioavailability. Also, new categories of therapeutics are coming up in terms of gene-based therapy and RNA-based therapy using siRNA and plasmid DNA delivery, which are aimed at regulating the expression of pathogenic proteins. Intranasal delivery of these genetic materials using nanocarriers has shown good preclinical results in the targeting of certain molecular pathways associated with neurodegeneration [50].
6. Applications in neurological disorders
Intranasal drug delivery has gained significant attention as a non-invasive strategy for targeting therapeutic agents directly to the central nervous system. By bypassing the blood–brain barrier and reducing systemic exposure, nose-to-brain delivery offers promising clinical applications across a range of neurological disorders. Its translational relevance is particularly evident in chronic neurodegenerative conditions and acute neurological injuries where rapid and efficient CNS targeting is essential.
Alzheimer’s disease
Amyloid-β plaque deposition, tau hyperphosphorylation, synaptic dysfunction and neuroinflammation are progressive cognitive impairments that are typical of the Alzheimer disease. Traditional oral treatment, cholinesterase inhibitor and NMDA receptor antagonist, are mainly associated with symptomatic treatment and are confined with low CNS bioavailability and systemic adverse reactions. Delivery by intranasal route has been explored as a way to increase concentrations in the central parts of the body whilst reducing peripheral toxicity. Insulin nasally has shown the possibility to enhance memory and cognitive functions through alteration of neuronal metabolism and synaptic plasticity. On the same note, intranasal delivery of neurotrophic factors, anti-inflammatory drugs, and anti-oxidant compounds have been promising in preclinical models by decreasing amyloid load and mitigating oxidative stress. Formulations based on nanotechnology technologically increase the brain targeting and prevent the degradation of labile biomolecules. All in all, intranasal delivery is a practical disease-modifying intervention approach in Alzheimer disease [51].
Parkinson’s disease
Parkinson disease is a motor degeneration disease where motor signs are caused by the death of dopaminergic neurons in the substantia nigra which causes tremor, rigidity and bradykinesia. Oral dopaminergic therapy is the mainstay of treatment, but its efficacy is constrained by variability of plasma concentrations, prolonged latency and peripheral adverse effects. The administration of dopamine and dopamine agonist intranasally provides a direct access to the brain and may enhance treatment output and lessen complications throughout the system. Moreover, intranasally administered antioxidant and anti-inflammatory compounds exhibit neuroprotective properties in animal models by attenuating mitochondrial dysfunction and oxidative stress. Polymeric nanoparticles and lipid-based carriers are nanoformulations that help to increase the stability of the drug and achieve a sustained release. Intranasal delivery is also non-invasive and thus overcomes issues of dysphagia and medication adherence that is very high in patients with Parkinson [52].
Stroke and ischemic injury
The acute ischemic stroke is caused by the lack of cerebral blood flow, which causes neuronal death through excitotoxicity, oxidative stress and through inflammatory cascades. Therapeutic intervention early is essential to contain the size of infarcts and preserve brain functioning. Neuroprotective agents can be rapidly delivered to the brain by intranasal delivery, bypassing the systemic circulation, making it possible to intervene in a timely manner. Intranasal delivery of antioxidants, anti-inflammatory agents, neurotrophic factors, and exosomes produced by stem cells have been studied as experimental studies in minimizing ischemic injury. Hematopoietic perfusion is impaired, and the direct nose-to-brain route permits therapy concentrations to be attained despite this. Also, intranasal thrombolytic adjuncts and anti-apoptotic agents are studied to improve functional recovery. Intranasal approaches are promising to be an addition to traditional reperfusion therapies despite the fact that clinical translation is still in progress [53].
Epilepsy
Epilepsy is a persistent neurological condition which is to be defined by periodic, unprovoked seizures caused by hyperexcitability of neurons. The promptness of seizures is crucial to avoid neuronal damage and chronic complications. Anticonvulsants by intranasal route deliver a fast and non-invasive alternative to rectal or intravenous delivery in an emergency department. Intranasal drugs can be used, which reach therapeutic CNS concentrations in seconds and allow timely seizures. Also, there are sustained intranasal delivery systems under investigation to be used as long-term seizure prophylaxis, especially in patients who do not adhere to oral therapy. Nano-carrier system can be used to increase brain penetration and minimize systemic side effects which is normally coupled with the use of conventional antiepileptic drugs. The convenience with which the caregivers can administer it also contributes to the increased practical value of intranasal formulations in pediatric and adult populations [54].
Brain tumors
The BBB is restrictive and systemic toxicity of high dose chemotherapy makes primary and metastatic brain tumors difficult to treat. The intranasal delivery is the direct route to deliver chemotherapeutic agents, targeted therapy, and gene-based therapy to the intracranial tumors. Preclinical experiments have also shown greater brain concentration of anticancer agents when they are administered intranasally as compared to systemic administration. Ligand-mediated uptake of nanoparticle-based carriers by specific tumor cells can be designed to enhance specific targeting of treatment to the tumor and reduce the effects of normal tissue. Nares administration also facilitates the administration of immunotherapeutic agent and RNA-based therapy to suppress oncogenic pathways. This strategy has promise to enhance the outcome in the management of brain tumor though additional clinical validation is needed [55].
Multiple sclerosis
Multiple sclerosis is an immune mediated disease that is marked by demyelination, neuroinflammation and progressive neuroaxonal destruction. The existing treatments are mainly focused on immune modulation and are normally delivered on the systemic level, which comes with adverse effects. Anti-inflammatory agent, neuroprotective and immunomodulatory peptide intranasal delivery has been considered to obtain local CNS actions with minimal effects on systemic immunosuppression. Inflammatory cytokine production, demyelination and remyelination have been shown to be attenuated, reduced and promoted respectively by intranasally delivered agents in experimental models. Additionally, nano-carrier systems improve stability as well as delivery targeting of inflamed neural tissues. Intranasal strategies can be used to reduce systemic toxicity and potentially to enhance the existing disease-modifying therapies in multiple sclerosis because they can be used to achieve direct CNS access [56].
CHALLENGES AND LIMITATIONS
The nose-to-brain drug delivery has a great potential in terms of therapeutic benefits, however, a variety of scientific, physiological, and translational difficulties can potentially restrict its extensive use in clinical settings. The main limitation is that the dosing volume of the nasal cavity is limited, and normally is limited to about 100-200 uL per nostril in adults. Surpassing this volume may result in overflow into the nasopharynx, ingestion of the formulation and loss in targeting. Therefore, it can only use very strong drugs or strong preparations effectively by intranasal administration, limiting the number of candidate molecules. Another important physiological block is the mucociliary clearance. The nasal epithelium is endowed with ciliated cells and goblet cells that produce mucus which serves as a defense mechanism since it traps foreign particles and removes them. Although this clearance reduces the residence time and absorption, although it is necessary in respiratory health, it rapidly eliminates administered formulations. Though mucoadhesive polymers and in situ gelling systems have shown a capability to increase mucosal contact period, it is difficult to balance between adhesion and patient comfort. Enzymatic breakdown in the mucosa of the nose is also a limitation, especially on the use of peptides/protein-based therapeutic. Drug stability might be diminished by proteases and other enzymes of the metabolic system before sufficient absorption has taken place. Moreover, the nasal physiological variability of people, i.e., the differences in the mucosal thickness, the composition of the mucus, the inflammation presence or the pathological conditions like rhinitis, may result in different drug absorption and the different outcomes of the therapy. The other issue is associated with the tight junction integrity and epithelial permeability. Whereas some permeation enhancers will enhance paracellular transport, the use of excessive permeation enhancer can lead to disruption of the integrity of epithelium and irritation or permanent mucosal damage. The safety and tolerability is of paramount importance particularly in chronic use in neurodegenerative diseases like Alzheimer disease and Parkinson disease where long term treatment is needed. Stability, scalability, and reproducibility are other challenges in terms of formulation. Nanoformulations and ligand-targeted system though very promising may be associated with complicated manufacturing procedures and expensive production. New intranasal nanocarrier regulatory routes can also be rigorous necessitating full safety and toxicology assessments. All of these issues highlight the necessity of future research to streamline formulation approaches, improve reproducibility and define long-term safety profiles. These limitations need to be addressed to make the translation of the intranasal nose-to-brain delivery systems to the routine clinical practice successful.
CONCLUSION
To sum up, nose-to-brain drug delivery is an innovative and scientifically sound approach to solving the problematic issues in neurotherapeutics of the past. The increased rate of neurodegenerative and neurological diseases worldwide requires novel strategies that can increase central nervous system (CNS) target but reduce the systemic toxicity and drug complication. The traditional oral and parenteral therapies are frequently limited by low blood-brain barrier permeability, first-pass metabolism, pharmacokinetic variability, polypharmacy and pill burden. The intranasal delivery provides an alternative compelling option because it provides direct anatomical access to the brain through olfactory and trigeminal neural access, thus bypassing the blood-brain barrier and acting rapidly. The use of formulation science has increased the viability and effectiveness of intranasal neuroprotective therapy by developing mucoadhesive systems, in situ gels, nano-carriers and surface-modified targeting platforms. These technologies help to stabilize drugs, extend the residence time of the drug in the nose, and allow controlled or targeted release in the CNS. The generalizability of the strategy is highlighted by its application in disorders like the Alzheimer disease, Parkinson disease, stroke, epilepsy, brain tumors, and Multiple sclerosis. However, issues of small dosing volume, mucociliary clearance, enzymatic destruction, inter-individual dispersion, and regulatory concerns need to be dealt with keenly to achieve safe and reproducible clinical results. Long-term interdisciplinary studies, combining neuroscience, pharmaceutics, nanotechnology and clinical pharmacology, will be necessary in order to optimize the delivery systems and long-term safety. Altogether, nasal nose-to-brain delivery has a considerable potential to decrease the pill burden, increase patient compliance and therapeutic accuracy in neuroprotection. This method can transform the future of CNS drug delivery and disease management with the principle of continued innovation and strict clinical testing.
REFERENCES

Prabhjeet Kaur, Rohit Kumar, Anish Banerjee, Manjima Mitra, Prabhuroshan S. M, Vibhu Bansal, From Nose to Brain: Unlocking Nasal Delivery to Reduce Pill Burden in Neuroprotective Therapies, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 168-186. https://doi.org/10.5281/zenodo.18856579
 10.5281/zenodo.18856579
10.5281/zenodo.18856579