Smt. Sharadchandra Suresh Patil College of Pharmacy Chopda.
Now a day’s cancer is the most prevalent life-threatening disease spreading .cancer is cell due to uncontrolled growth which can be cured .Various kinds of immunotherapy treatment for cancer are either public to the available or this process of clinical trials. Immunotherapy is a treatment that uses specific components of a persons immune system to fight disease. Cancer immunotherapy is the types of cancer treatment that helps the immune system fight cancer . cancer immunotherapy represents a standing example of precision medicine ; immune checkpoint inhibitors target the checkpoint ; tumor infiltrating lymphocytes ,TCR T cell ,and CAR T cell precisely kill cancer cells through tumor antigen recognition and , cancer vaccines are made from patient – derived dendritic cells ,tumor cell DNA ,or RNA ,or oncolytic viruses , thus offering a type of personalized medicine . Immunotherapy treatment have potential to treat cancer with significantly less toxicity than chemotherapy and radiation treatment .It discusses the effectiveness of these therapies in improve the immune system’s ability to detect and destroy cancer cells. cancer is screened by different screening test and a number of treatments are now available these days such as gene therapy ,chemotherapy , surgery, radiation therapy ,immunotherapy etc. . In future up on 2030 around 22.2 million cases are expected to be diagnosed for cancer.
Recent FDA approval of immune checkpoint inhibitors and T lymphocytes expressing chimeric antigen receptors (CART) for cancer therapy signifies to success in cancer immunotherapy .cancer immunotherapy would not have reached such a milestone without advances in the area of cancer immunology .During tumor development ,the immune system constantly engages with tumor cells, which undergo three: elimination, equilibrium .T cells specific for tumor antigen predicted by cutting edge tumor genome sequence have been detected in patient with melanoma .[1] cancer arises from growth of abnormal cells due to normal alterations in gene expression , disrupting the balance between cell proliferation and cell death. ,these leads to changes the development of population of cell capable of invading surrounding tissues and spreading to distant sites, a process known as metastasis .this procedure can result in considerable illness and. if not addressed may ultimately lead to the death of affected individual .[2] There can be cancer response to develop in balance of immune system called cancer immune editing. This is a dynamic process where the immune system regulates cancer in three different phases. These phases include elimination , equilibrium ,and escape.The elimination phase is where the cancer or through the skin in biological cells are detected by the immune surveillance and essentially .[3] Innate immune response is an important factor in controlling the spread of cancer . The innate response involves the use of natural killer cells, macrophages, dendritic cells (DC), and Dc/T cell response . killer cells include CD3-, CD16+ and have the potential to recognize and eliminate tumor via perforin / granzyme, and can induce apoptosis in a variety of cells lines .Macrophages in particular M1 macrophages, have to kill tumor cells by secreting inflammatory cytokines which can exert cytotoxic activity in addition to tumor –destructive reaction .[4]
Mechanisms of cancer immune evasion
T cells need to recognize tumor antigen to kill tumor cell. Thus ,one important mechanism of tumor immune evasion is that tumor cells their antigen processing /presentation machinery ,such as the major histocompatibility complex (MHC)I ,proteosome subunit latent membrane protein (LMP)2 and LMP7, transported associated with antigen processing (TAP)protein ,and tapasin ,preventing them from being recognized by T cell . it is well known that IFN- induced signaling promotes antigen present in tumor cells,and recently,IFN signaling has been positively regulated show to by Aplnr and regulated negative by Ptpn2 and CDK4/6.(5)
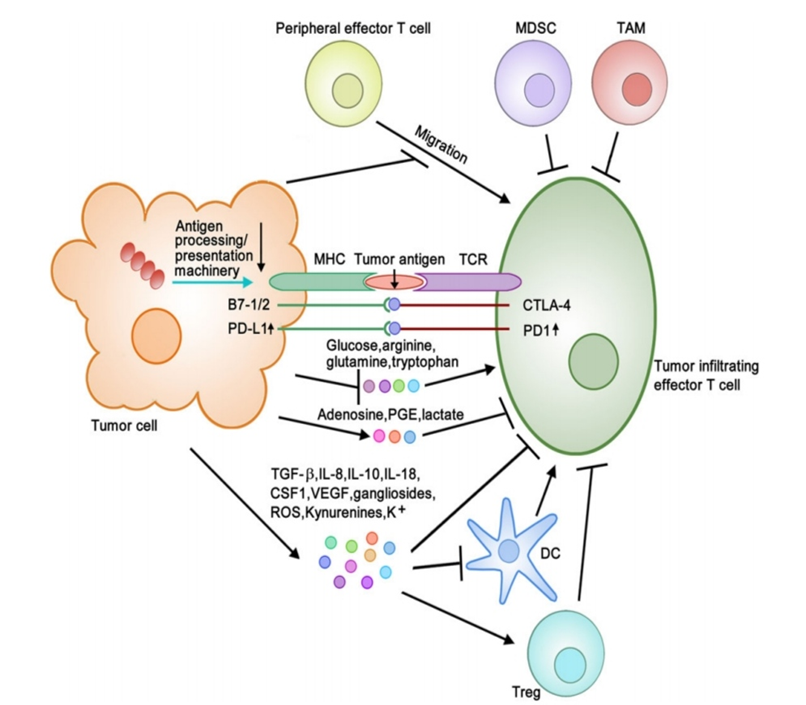
Fig. 1:-Diagram Of Mechanism of Tumor Immune Evasion
Cancer cells can directly cause T cell exhaustion by facilitating their PD-L1 and B7-1/2 binding to immune checkpoint proteins PD-1 and CTLA-4 , represent ,on T cells . moreover ,cancer cells may cause cell exhaustion by increasing PD-L1 and PD-1 expression . As PD-L1 expression is positively regulated by inflammatory signaling (e.g. IFN, LPS, TNF –a ) . Another mechanism of cancer immune evasion is immune suppression modulators of secretion (e.g. TGF-B,IL-18,CSF1, VEGF, gamgliosides, ROS, Kynurenines , k+) into the tumor microenvironment (TME) by tumor cells. (6)
Immune checkpoint
Specialized biological pathways have been adopted by cancer cells growth to promote the tumor microenvironment [7] immune system checkpoint s play a role in autoimmunity and reducing collateral tissue damage caused by immune reactions through the regulation and inhibitory signaling pathways [8] immune checkpoint inhibitors being derived from malignant cells express immune system visible the cancer cell to make foreign antigen (immunogenic ) . Numerous vaccines combined patient antigen presenting cells (APC ,commonly dendritic cells ), cancer antigens can such as a cytokine to activate CTL response . In the dramatic success of immune checkpoint blocked, even in advanced melanoma , non-small cell lung cancer spontaneously immunogenic ,but the response of immune system is inhibited by factors in the tumor microenvironment .(9) Immune checkpoints are negative defense that play critical roles in maintaining self –tolerance , prevent autoimmunity ,and protecting tissues from immune collateral damage .(10) These immune checkpoints are often enhanced by cancers that allow them immune system to avoid antitumor . A promising approach for activating antitumor immunity them checkpoint block immune system(11)
Types of cancer :-
On the Basis of tissue effected: -
- Carcinomas are characterized by cells that cover internal and external parts of the body such as lung, breast and colon cancer .
- sarcomas are characterized by cells that are located in bone, cartilage ,fat ,connective tissue, muscle and other supportive tissues.
- Lymphomas are cancers that lymph nodes and immune system tissues.
-Leukemia’s are cancers that bone marrow and often accumulate in the bloodstream.
-Adenomas are cancers that arise in the thyroid , the pituitary gland ,the adrenal gland and other glandular tissues.(12)
Symptoms :-
Cancer symptoms are depended on the type and location of the cancer .For example, lung cancer can cause coughing ,shortness of breath ,or chest pain. Colon cancer often causes diarrhea ,constipation and blood .
The following symptoms can occur with most cancers:
Genetically modified Dendritic cells
There are several reasons why the immune systems protect against cancer is challenging. This including antigens associated tumor. Immune system are regulators in Dendritic cells as well as inhibitors or stimulators of T cells and B cells. Dendritic cells to recognize and cancer cell to support an immunological response and change tumor intercellular response associate antigens and signal to T cells and B cell. Dendritic cells are used to present in with new genes that alter the intercellular pathway associated with creating robust immune system. (14)
NKTS Stem cell Immunotherapy
Immunotherapy through use of stem cells remains in its infancy and has become focused as other forms of immunotherapy. Some stem cell therapies includes stem cell inducing to produce dendritic cells, natural killer cells, and antigen specific T cells . The dendritic cells were functional but had cross limited ability for presentation of antigens to CD8+ T cells MHC . Differentiation of ES cells to form antigens specific naïve T -cells has been produced by a combination of transcription factors and the introduction of fetal thymus organ culture in order in to provide an environment conductive for the formation of diverse CD+4 and CD+8. These have also been reports of successfully differentiated induced pluripotent stem cells to form antigens specific T-cells that can recognize the epitope of melanoma antigens antigen MART-1. Natural killer cell have been derived from induced pluripotent stem cells in a two stage culture system. (15)
Natural killer Cell immunotherapy
Natural killer (NK) cells, also known as CD56+ and CD3+, are lymphocytes with cytotoxic potential against anti-self cells. NK cells can be activated and inhibited via several receptor-ligand interactions depending on whether the cells encounter self or anti-self MHC antigens. Licensing via KIR receptor is an important step with regard to how NK cells recognize anti-self cells before they can be fully activated. NK cells have anti-cancer characteristics but also be attenuated by either molecules secreted by cancer cells or the cancer micro-environment acidity can paralyze the cells. (16)
Natural killer T cells Immunotherapy
Natural killer T (NKT) cells are able to bridge the gap between the innate adaptive immunity by establishing memory responses in addition to improving protective immune response. The NKT cell is activated by the glucosylceramide (GalCer) ligand which results in the expansion of NKT cells which in turn inhibit the growth of metastasis and liver metastasis in melanoma in vivo mouse model. Mice with induced liver metastasis and treated with alpha GalCer/DCs resulted in complete remission of liver metastasis a week after treatment. (17)
Role of Dendritic Cells in Cancer Immunotherapy
Dendritic cells (DCs), sometimes called “nature's adjuvant,” are induced in the course of immunizations with cancer vaccines, but are potentially subject to the same immunoregulatory mechanisms that have restrained vaccination as discussed in relation to T cells. The development of approaches to generate DCs sex vivo has circumvented issues relating to the dysfunction of endogenous DCs in patients with cancer, allowing controlled loading of DCs with antigens to ensure delivery of the proper signals required for effective immunization. (18)
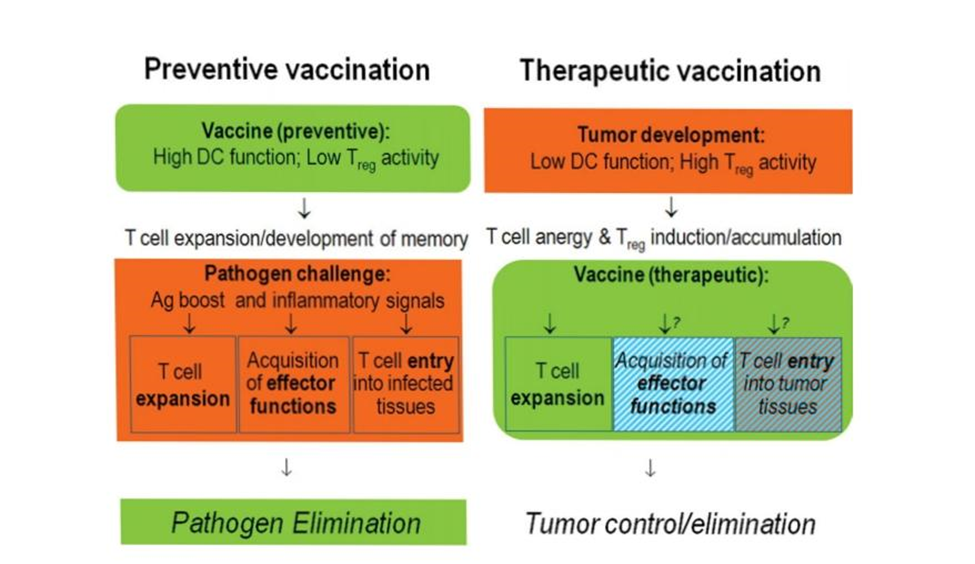
Fig. 2: - Different Tasks of Preventive Versus Therapeutic Vaccines. Therapeutic vaccines need to function despite tumor-induced dysfunction of endogenous dendritic cells (DCs) and in the presence of tumor-induced suppressive cells such as regulatory T cells (Treg). Their roles go beyond the induction of long-lived memory cells, because cancer is a poor source of proinflammatory alarm signals capable of inducing effector functions and peripheral homing potential in antigen (Ag)-specific T cells.
These signals required for effective immunization are, initiatily, , antigens uptake and T -cell (signal1) ,which determine the specificity of T-cells response, and costimulatory molecule-mediated expansion (signal2), which determines the magnitude of response of the selected tumor-specific T cells. Ex. Vivo production of DCs also allows the imprinting of additional features critical for DCs to induce effective cancer immunity, such as preferential interaction with selected subsets of effector immune cells , and imprinting of desirable effector mechanisms in CD4+and CD8+ T cells to selectively enhance Th1(Th1) -, CTL-, and NK cell-mediated type 1 immunity and (polarizing signal 3, which determines effector function and immunity type [Th1 or Th2]. (19) The DCs expressed levels of constimulatory molecules, at least when assessed directly after removal from culture, and constituted weaker immunogens than the mature DCs used in “second- generation “DC vaccines. They showed limited ability to induce objective clinical response as Assesed by response Evaluation Critical in solid Tumor (RECIST) or World Health Organization (WHO) criteria, but 2 recent phase 3 trials of “first generation “ DC-based of patients with advanced hormone -refractory prostate cancer . (20)
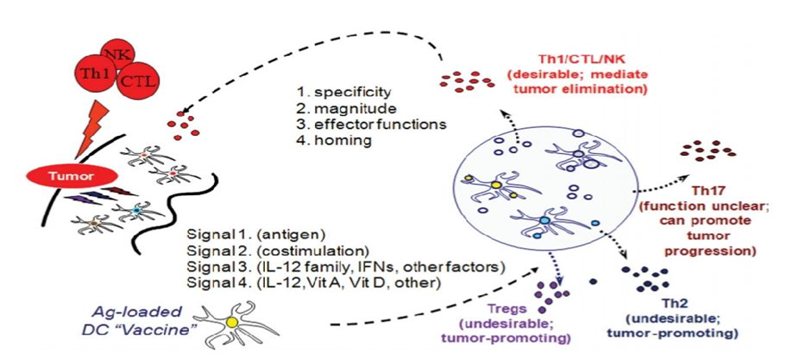
Fig.3 :- Dendritic cells provide different types of information to tumor specific T cells. DC provide T cell with antigenic “signal 1”costimulatory “signal 2”
Immune Checkpoint blocked therapy
Immune Checkpoints refer to immunosuppressive molecules. Physiologically, immune tolerance regulating immune responses and preventing tissue damage. The high expression of Checkpoints can mediate tumor immune evasion by inhibiting immune cell function, in the development and activation of tumor. (21)
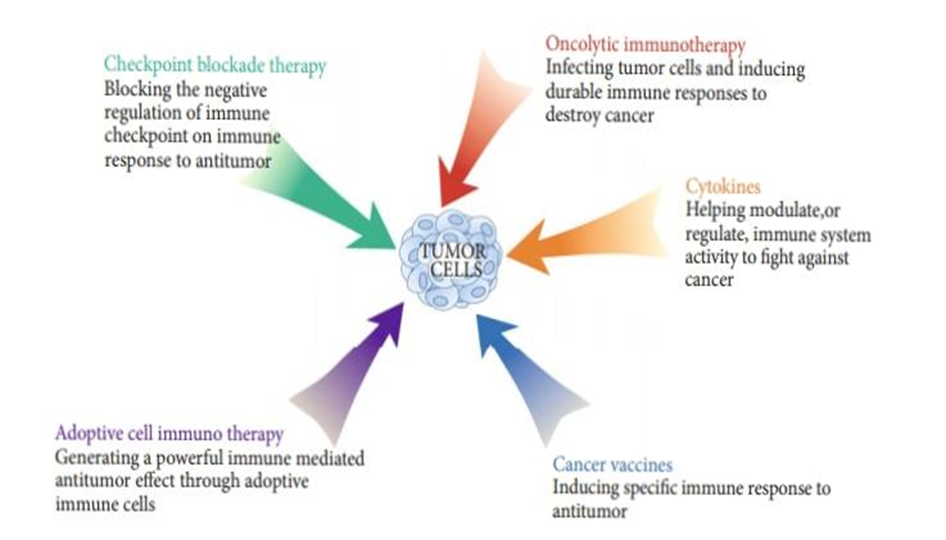
Fig 4:-mechanisms of cancer immunotherapy
Checkpoint inhibitors
Tumor directed monoclonal antibodies
These mAbs can bind specific tumor antigens, stay on the surface and activate antibody /complement-dependent cytotoxicity, or affect downstream signals. Monoclonal antibodies promote tumor killing by induction of apoptosis, receptor blocked or agonist activity, delivery of cytotoxic agents, radiation, immune -mediated cell killing, or through specific effects on tumor vasculature and stroma. (22)
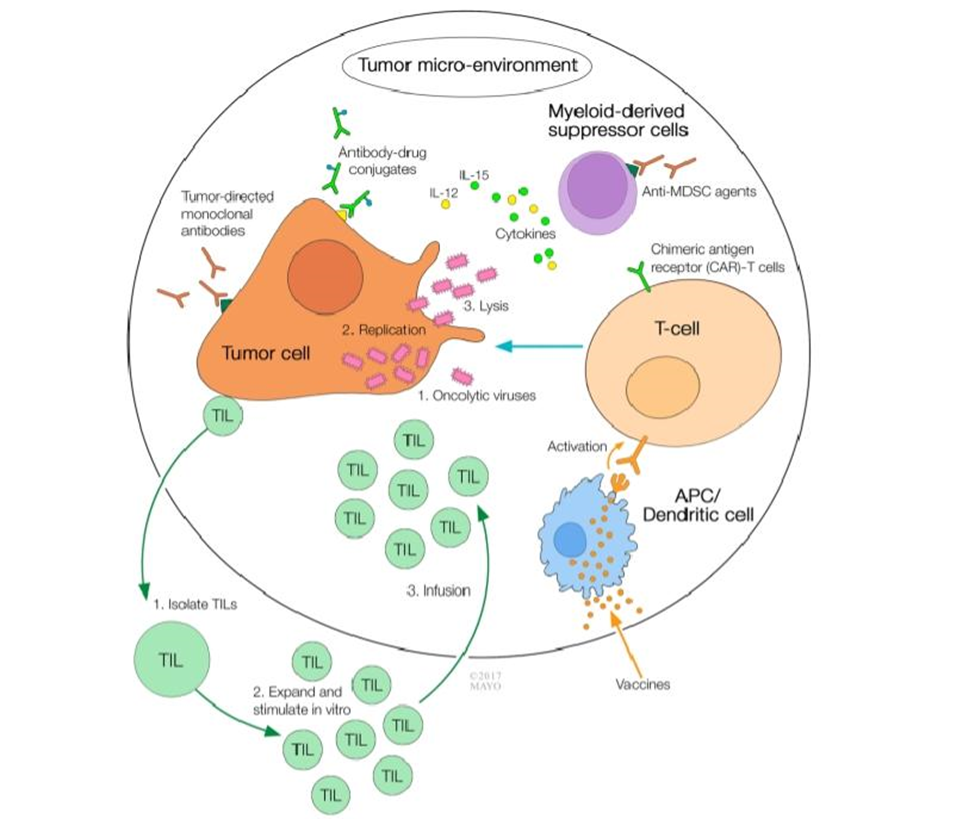
Fig 5:- Multi-modality cancer immunotherapy approach
Cytokines Therapy
Cytokines serve a molecular messenger facilitating communication among immune system cells, enabling them to mount a coordinated, robust, yet self-limited response to a specific antigen . These proteins, whether secreted or membrane-bound , act as mediators of intercellular signaling, there by regulating the immune systems homeostasis. Produced by both innate and adaptive immune cells, cytokines are elicited in response to microbial pathogens as well as tumor antigens. Two cytokines that are currently approved by the FDA for clinical use are Interferon alpha (IFN) and interleukin-2 (IL-2) .(23)
Table 1. Summery of different immunotherapy on cancer.
|
Immunotherapy |
Agent |
Indication |
Immune Checkpoint Therapy
|
Anti-CTLA-4 Therapy |
Ipilimumab |
Melanoma, renal cell carcinoma prostate cancer, ovarian cancer |
|
Anti-PD-1/PD-L1Thrapy |
Nivolumab |
Metastatic melanoma, non-small cell lung carcinoma |
|
LAG-3 or CD223 |
Immuntep (IMP321) |
Melanoma, prostate cancer, metastatic breast |
|
TIM-3 |
MBG453 |
Advanced malignancies |
Adoptive Cell therapy
|
TILs |
Novartis's tisagenlecleucel-T |
Melanoma, Pancreatic cancers |
|
CAR-T |
Kite/Gilead's |
Refractory adult large B-cell lymphoma. |
Monoclonal antibodies Therapy
|
Naked mAbs |
Transtuzumab (Herceptin) |
Breast cancer. |
|
Naked mAbs |
Cetuximab |
HNSCC Patients. |
|
Bispecific Monoclonal Antibodies |
Blinatumomab |
Relapsed or refractory acute lymphoblastic leukemia |
Cancer vaccines
|
Prophylactic vaccines |
Gardasil |
Cervical cancer |
|
Therapeutic cancer vaccines |
Bacillus calmette -Guerin (BCG) |
Early -stages bladder cancer
|
|
Therapeutic cancer vaccines |
Sipuleucel -T (proverge®?) |
Prostate cancer |
Cytokines Therapy
|
Interferon alpha |
Intron-A |
Melanoma, renal and kidney cancer, hairy cell leukemia |
|
Interleukin-2 |
Proleukin (aldesleukin) |
Renal and kidney cancer |
Harnessing Antitumor Antibodies for Cancer Therapy
The development of the hybridoma technology in the 1970s overcomes past difficulties. Hybridoma technology enabled the production of highly specific antibodies against human TAs in quantities sufficient for Therapy, and with a reliability that would allow it’s application by multiple investigators for the production of mouse mAbs to many human TAs. Some, such as the carcinoembryonic antigens (CEA), were known TAs that had been already extensively characterized others such as chondroitin sulfate proteoglycan 4(CSPG4), we’re newly identified TAs. (24) .
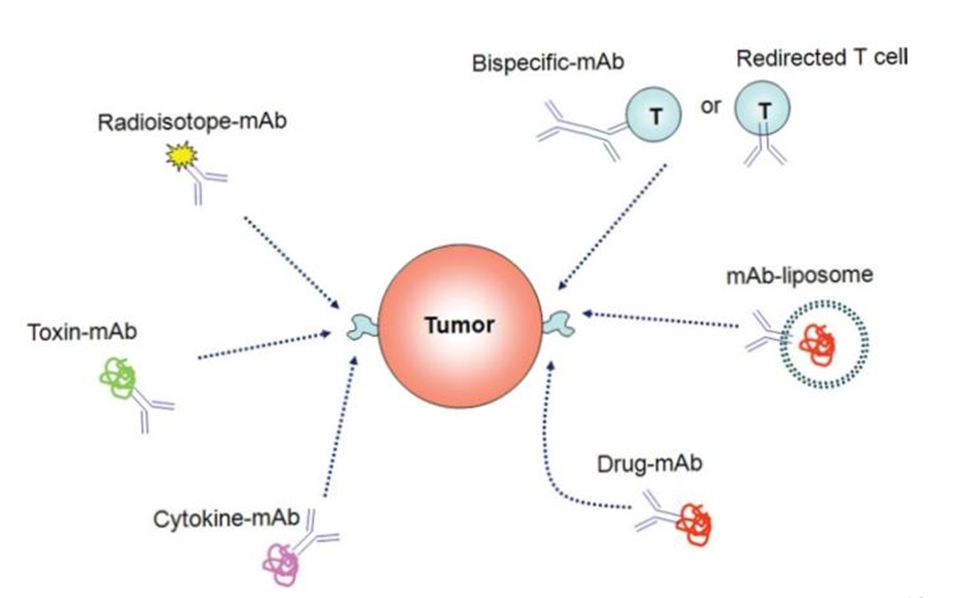
Figure 6:- Mechanisms Used by Monoclonal Antibodies to mediate Antitumor Effects. Multiple roles of monoclonal Antibodies (mAbs) in cancer therapy are shown.
Genetic strategies for cancer immunotherapy
Many approaches for the genetic immunization of solid tumors have been investigated. Early work attempted to directly inject tumors with plasmid DNA and vectors encoding cytokines and allogenic MHC molecules, designed to promote an immune response to the tumor but resulting in minimal effeciency( generally only affecting the injected tumor) and minimal (systemic) immunologic impact. Another genetic approach is to use plasmid and /or viral vector DNA to systemically immunize subjects. This approach is inexpensive, simple, and allows for Immunization with multiple genes (fig.7)
Naked DNA Immunizations:
Plasmid-based DNA Immunization is a powerful method of Immunization against microbial and viral antigens, capable of generating both antibody and cellular responses, particularly in mice. Uptake of Protein antigens produced by locally transfected cells, generally muscle, sub-sequently taken up by the patient’s endogenous APCs, (“cross-presentation”) is thought to be the main mechanism ofgenerating T cell immunity, although direct gene transfer to local APIs has demonstrate similar T cells immunity. (25)
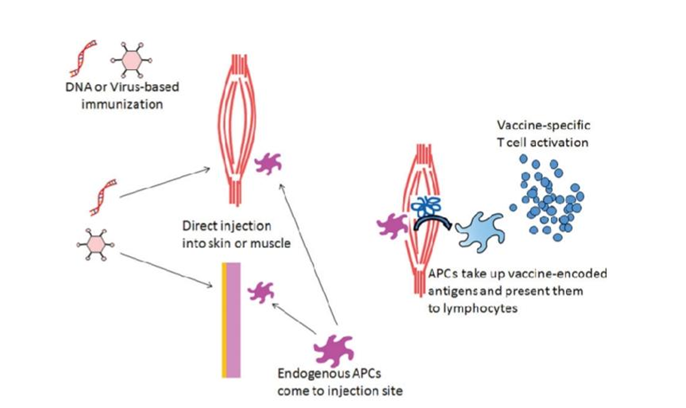
Fig. 7:-Genetic Immunizations. Plasmid DNA and viral vector can be utilized for vaccination by direct injection, often into muscle or skin. While direct transfection /transaction of antigen-presenting cells (APIs) at the injection site can occur, the transfected tissue serves as a source of vaccine protein that can be taken up as cross-presented by host APCs to activate antitumor immunity.
REFERENCES

Unnatibai Bhadane*, Amruta Patil, Yogesh Chaudhari, Immunotherapy of Cancer, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 1309-1320 https://doi.org/10.5281/zenodo.17568277
 10.5281/zenodo.17568277
10.5281/zenodo.17568277
