
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of pharmaceutical chemistry, Kamalakshi Pandurangan college of pharmacy, Ayyampalayam, Tiruvannamalai, Tamilnadu, India 606603.
Cancer remains one of the most significant global health challenges, with high mortality rates and limited treatment success for advanced stages. Since the approval of cisplatin, metal-based drugs have played a central role in chemotherapy. However, the severe toxicity, drug resistance, and poor selectivity of platinum-based agents have driven the exploration of next-generation metal complexes with novel structures, mechanisms, and delivery strategies. This review integrates recent advances in the design of non-platinum metal complexes—including ruthenium, gold, copper, titanium, and emerging metals—linking their structure–activity relationships (SAR) to mechanistic pathways such as redox modulation, enzyme inhibition, photodynamic activation, and epigenetic regulation. We highlight strategies to improve efficacy and selectivity through ligand modification, prodrug activation, nanocarrier systems, and tumor microenvironment targeting. Clinical trial updates are discussed alongside future perspectives for translational research. This comprehensive analysis aims to bridge the gap between laboratory innovation and clinical application, underscoring the potential of mechanism-driven design to redefine metal-based chemotherapy.
1.1 Global cancer burden
Cancer is a leading cause of morbidity and mortality worldwide, responsible for an estimated 10 million deaths annually [1]. Incidence rates continue to rise due to aging populations and lifestyle factors; projections indicate a significant increase in global cancer cases over the next two decades [2]. Although early detection and targeted therapies have improved outcomes for certain tumor types, systemic chemotherapies remain indispensable in the management of many solid and hematological malignancies.
1.2 Evolution of metallodrugs
The discovery of cisplatin in the 1960s marked a watershed in medicinal chemistry, demonstrating that simple coordination complexes can exert profound biological effects [3]. Subsequent development of carboplatin and oxaliplatin sought to retain antitumor efficacy while reducing side effects. Nevertheless, platinum drugs primarily operate via DNA crosslinking and encounter limitations in selectivity and resistance.
Figure 1: Overview of non-platinum metal complexes in anticancer therapy.
1.3 Limitations of platinum-based chemotherapy
Platinum therapeutics incur dose-limiting toxicities such as nephrotoxicity, peripheral neuropathy, and myelosuppression, which restrict optimal dosing [4]. Tumor resistance emerges through multiple mechanisms: enhanced DNA repair (nucleotide excision repair), increased drug efflux (ATP-binding cassette transporters), detoxification via glutathione conjugation, and inhibition of apoptotic signaling [5]. These clinical challenges underpin the ongoing search for alternative metal-based therapeutics with distinct mechanisms and improved therapeutic windows.
1.4 Rationale for next-generation metal complexes
Non-platinum metals (ruthenium, gold, copper, titanium, palladium, iridium, etc.) present rich coordination chemistry, multiple accessible oxidation states, and varied ligand architectures. These properties enable modes of action not limited to DNA crosslinking — e.g., redox modulation, enzyme inhibition, photochemical activation, and epigenetic regulation — which can address resistance and selectivity shortcomings of platinum compounds [6].
1.5 Scope and novelty of this review
This review focuses on mechanism-driven design of next-generation metal complexes and their translation from laboratory discovery to clinical testing. We place particular emphasis on structure–activity relationships (SAR), delivery strategies, and representative clinical advances to give a cohesive view bridging chemistry and medicine.
2. Classification Of Non-Platinum Metal-Based Anticancer Agents
This section groups representative non-platinum complexes by metal and highlights key ligand types, mechanisms, and current translational status. For each compound listed in Table 1.
Table 1 – Representative of Next-Generation Metal Complexes with Mechanism and Clinical status
|
Sr.no: |
Metal |
Example Compounds (structure below each name) |
Ligands Used / Typical Donor Types |
Key Mechanism(s) |
Clinical Status |
|
1 |
Ruthenium |
NAMI-A |
Imidazole, indazole, polypyridyl |
Redox activation, metastasis inhibition, DNA interactions |
Phase I/II (varies by compound) |
|
2 |
Gold |
Auranofin |
Phosphine, N-heterocyclic carbenes (NHC), porphyrin cores |
Thioredoxin reductase inhibition, protein targeting |
Clinical evaluation (Auranofin in various trials) |
|
3 |
Copper |
Casiopeínas |
Phenanthroline, Schiff bases, mixed N,O donors |
ROS generation, proteasome inhibition, redox cycling |
Preclinical / early translational |
|
4 |
Titanium |
Titanocene dichloride |
Cyclopentadienyl (Cp), alkyl/halide ligands |
DNA interaction, hydrolytic activation |
Early-phase clinical studies historically |
|
5 |
Palladium |
Pd-salen |
Salen, polypyridyl ligands |
DNA intercalation, enzyme inhibition |
Preclinical |
2.1 Ruthenium complexes
Ruthenium complexes have attracted attention because of their kinetic stability, multiple oxidation states (Ru(II)/Ru(III)), and favorable ligand exchange chemistry that can be tuned for activation in biological milieus. Notable examples include NAMI-A (imidazole-containing, metastasis-inhibiting), KP1019 (indazole-based, antitumor), and NKP-1339 (a Na-derivative with improved solubility and pharmacokinetics). Mechanistically, ruthenium complexes can act via DNA binding, inhibition of metastasis pathways, and redox-mediated cytotoxicity; some are designed as prodrugs activated by reduction in the tumor microenvironment [7-9].
NAMI-A (imidazolium trans-[tetrachloro(dimethyl sulfoxide)(imidazole)ruthenate(III)])

Figure 1.2: Chemical structure of NAMI-A. imidazolium trans-[tetrachloro (dimethyl sulfoxide) (imidazole) ruthenate (III)] complex.
KP1019 (indazolium trans-[tetrachlorobis(indazole)ruthenate(III)])
Figure 1.3: Chemical structure of KP1019, an indazolium trans-[tetrachlorobis(indazole)ruthenate(III)] complex.
NKP-1339 (sodium trans-[tetrachlorobis(1H-indazole)ruthenate(III)])
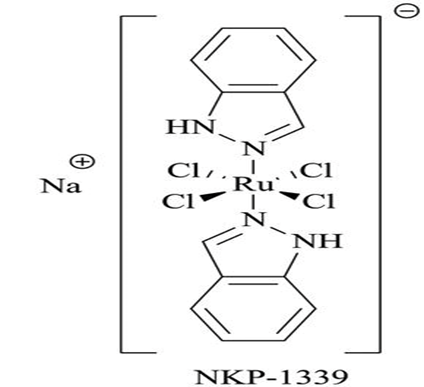
Figure 1.4: Chemical structure of NKP-1339, a sodium trans-[tetrachlorobis(1H-indazole)ruthenate(III)] complex.
SAR Note – Ligand Electronics & Geometry Effects in Ruthenium Complexes
Electron-donating ligands (e.g., alkyl-substituted amines, methoxy-aryl) raise the Ru(III)/Ru(II) redox potential, facilitating easier reduction under hypoxic tumor conditions → ↑ activation in cancer cells[39]. Electron-withdrawing ligands (e.g., halogens, nitro-aryl) lower the redox potential, stabilizing the Ru(III) oxidation state → ↓ premature activation, ↑ stability in plasma.
2.2 Gold complexes
Gold(I/III) complexes (e.g., Auranofin) show potent inhibition of thioredoxin reductase (TrxR) and related selenoenzymes, disrupting redox homeostasis and inducing apoptosis particularly in drug-resistant and hematological malignancies. Auranofin’s repurposing potential has been explored in several clinical settings, and Au(III)-porphyrin complexes add photophysical handles for combined photodynamic/chemical cytotoxicity [11-12].
Au(III)-Porphyrin

Figure 2: Chemical structure of a gold(III) complex with a tetradentate N-heterocyclic macrocyclic ligand coordinated to a chloride ligand.
2.3 Copper complexes
Copper-based agents (Casiopeínas, Cu-phenanthroline derivatives) leverage copper’s redox cycling ability to catalyze Fenton-like reactions in cells, raising ROS to cytotoxic levels selectively in cancer cells with already elevated oxidative stress. Additionally, copper complexes have been reported to inhibit proteasome activity and modulate signaling pathways [13-15].
Casiopeina III-ia (Cu(4,7-dimethyl-1,10-phenanthroline) (acetylacetonate))

Figure 3: Chemical structure of a copper(II) complex containing 2,9-dimethyl-1,10-phenanthroline and an amino acid-derived ligand, coordinated with a water molecule and nitrate counterion.

Figure 3.1: Chemical structures of copper(II) complexes with various substituted phenanthroline ligands, showing different methyl, phenyl, chloro, and nitro substitutions that influence electronic properties and biological activity.
2.4 Titanium complexes
Organotitanium complexes such as titanocene derivatives exhibit unique DNA binding modes and lower nephrotoxicity relative to cisplatin. Their clinical evaluation faced formulation and stability challenges, but they remain of mechanistic interest due to different cellular processing and activation pathways [14].
Titanocene Dichloride (Cp?TiCl?)
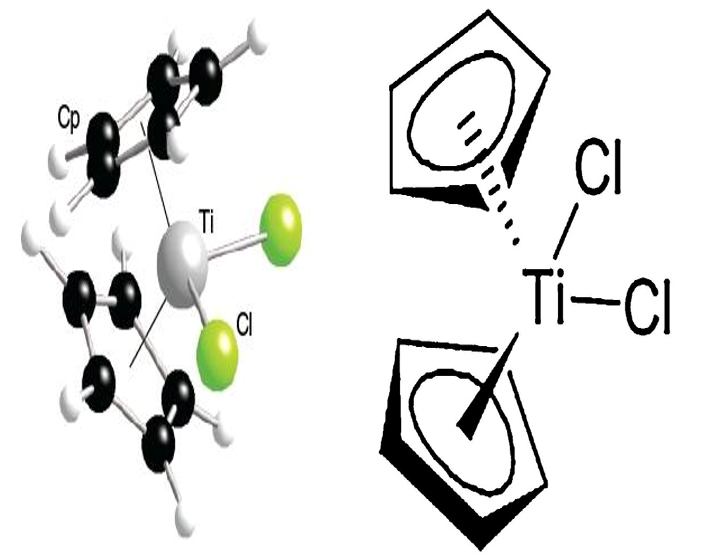
Figure 4: Chemical structure of titanocene dichloride, a metallocene titanium(IV) complex featuring two cyclopentadienyl ligands and two chloride ligands.
2.5 Palladium Complexes
Palladium complexes, especially with extended aromatic ligands (dppz), can intercalate DNA and disrupt enzyme function. Iridium and osmium complexes are emerging for photodynamic/photocatalytic therapies owing to their strong luminescence and ability to produce singlet oxygen [17-19].
Pd(II)-Salen Complex

Figure 5: ORTEP diagram of a palladium(II) complex showing the coordination of bidentate N,O-donor ligands to the central Pd atom, with thermal ellipsoids depicted at the 50% probability level.
2.6 Iridium Complexes
Ir(III)-Cyclometalated Complexes

Figure 6: Chemical structures of a series of iridium(III) polypyridyl complexes (1–5) featuring varied ancillary ligands, illustrating structural modifications aimed at tuning their photophysical and biological properties.
2.7 Osmium Complexes
Os(II)-Polypyridyl Complexes
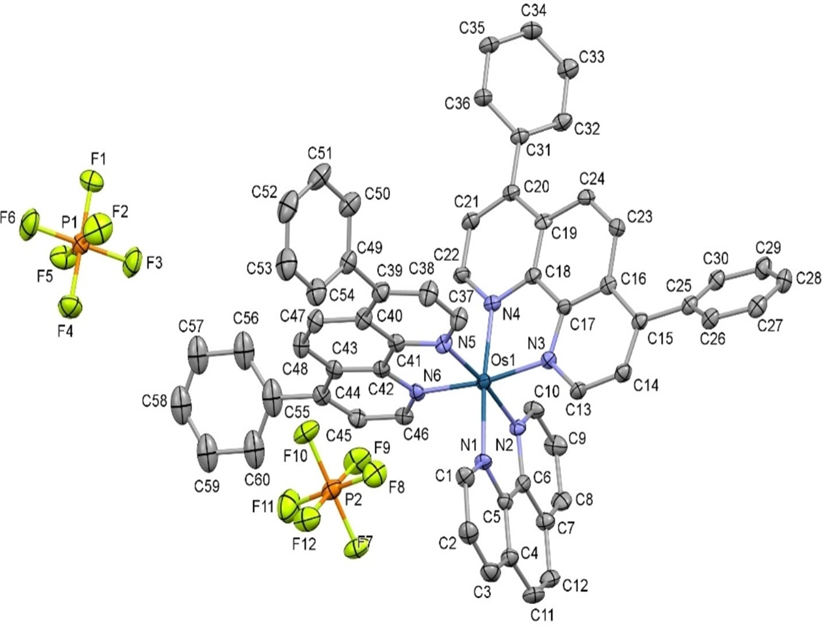
Figure 7: ORTEP representation of an osmium (II) polypyridyl complex with coordinated aromatic ligands and hexafluorophosphate counterions, showing the atomic labeling scheme and thermal ellipsoids.
3. Mechanisms Of Action
Non-platinum metal complexes exert anticancer effects through multiple, often overlapping, pathways. The diversity in metal coordination chemistry allows targeting of DNA, enzymes, redox systems, and specific signaling pathways.
3.1 DNA Damage and Crosslinking
3.2 Enzyme Inhibition
3.3 Reactive Oxygen Species (ROS) Generation
3.4 Photodynamic Effects
3.5 Apoptotic Pathway Activation
4. Advantages And Limitations
The design of non-platinum complexes aims to overcome platinum-based drug drawbacks such as nephrotoxicity, ototoxicity, and acquired resistance. However, limitations remain.
5. Clinical Progress and Trials
Several non-platinum complexes have entered various stages of clinical evaluation
Table 2: Advantages and Limitations of Non-Platinum Metal Complexes
|
Sr no: |
Metal Complex Type |
Advantages |
Limitations
|
|
1 |
Ruthenium (III/II) complexes |
Lower toxicity than cisplatin, activity in hypoxic tumors, redox activation potential |
Limited oral bioavailability, possible off-target protein binding |
|
2 |
Gold(I/III) complexes |
Strong TrxR inhibition, potent against resistant lines |
Risk of systemic oxidative stress, stability issues in vivo |
|
3 |
Copper (II) complexes |
ROS-mediated DNA/protein damage, inexpensive and abundant |
Non-selective ROS generation may harm healthy tissue |
|
4 |
Titanium (IV) complexes |
Different binding target (DNA phosphates), potential immunomodulation |
Hydrolysis instability, limited clinical efficacy so far |
|
5 |
Palladium (II) complexes |
Rapid ligand exchange, tunable activity via ligand modification |
Instability in biological media, non-specific DNA damage |
|
6 |
Iridium (III) complexes |
Theranostic potential, photodynamic therapy capability |
Requires light activation, tissue penetration limits |
Table 3: Clinical Trials Overview
|
Sr no: |
Compound |
Metal |
Indication |
Trial Phase |
Key Findings |
|
1 |
NAMI-A |
Ru(III) |
Non-small cell lung cancer, melanoma |
Phase II |
Anti-metastatic effect with minimal tumor shrinkage |
|
2 |
KP1019 |
Ru(III) |
Gastrointestinal cancers |
Phase I |
Well tolerated, disease stabilization in some patients |
|
3 |
KP1339 |
Ru(III) |
Advanced solid tumors |
Phase I/II |
Improved pharmacokinetics, early signs of efficacy |
|
4 |
Auranofin |
Au(I) |
Ovarian cancer, leukemia |
Phase II |
Targets TrxR, manageable toxicity |
|
5 |
Titanocene dichloride |
Ti(IV) |
Renal cell carcinoma |
Phase II |
Limited efficacy, short plasma half-life |
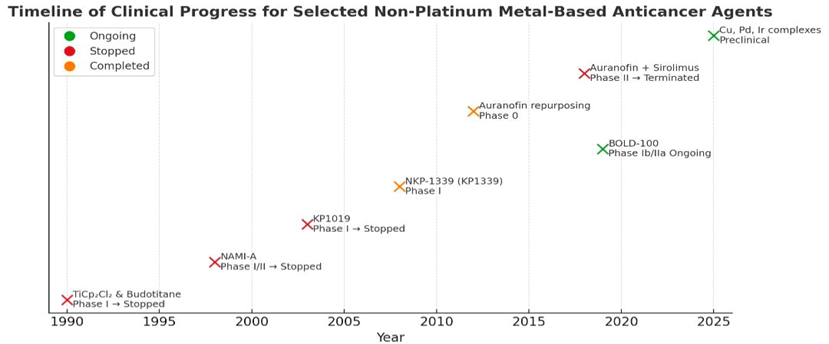
Figure 8: Timeline of clinical progress for selected non-platinum metal-based anticancer agents
6. Strategies To Improve Efficacy and Selectivity
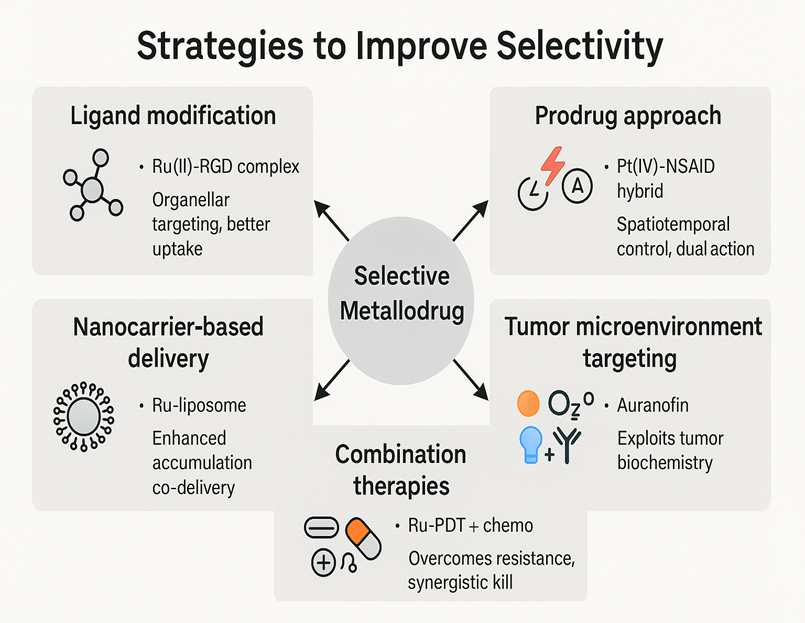
Figure 9: Schematic representation of strategies to improve the selectivity of metal-based anticancer drugs.
7. CONCLUSION AND FUTURE PERSPECTIVES
Non-platinum complexes represent a promising expansion of the metallodrug field, with tunable structures for multi-targeted approaches. Combining therapeutic and diagnostic capabilities (theranostics) may revolutionize personalized cancer treatment. Advances in nanotechnology, ligand chemistry, and bioinorganic design will likely lead to next-generation metal complexes with improved selectivity and safety profiles. Non-platinum metal complexes offer mechanistic diversity, tumor selectivity, and activity against resistant cancers. Yet, clinical adoption has been hindered by stability, pharmacokinetic, and efficacy challenges. Future research should prioritize:
REFERENCES





V. Srivarshan*, A. Arun Mozhi Varman, M. Chanduru, K. Bakkiyaraj, Dr. D. Rajalingam, Next-Generation Metal Complexes in Anticancer Therapy: From Mechanism-Driven Design to Clinical Translation, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 8, 2436-2451 https://doi.org/10.5281/zenodo.16931001
 10.5281/zenodo.16931001
10.5281/zenodo.16931001