
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
M.A.M College of Pharmacy .
Lacosamide (LCM) is a novel agent that has been developed as an antiepileptic drug. In vitro studies suggest that LCM modulates voltage-gated sodium channels by enhancing their slow inactivation. In addition, LCM seems to interact with collapsin-response mediator protein 2 and thus may mediate neuronal plasticity. LCM has an elimination half-life of 13 hours, no relevant protein binding, and does not induce or inhibit enzymes of the cytochrome P450 system. No clinically significant drug–drug interactions have been discovered as yet. Experimental data suggest anticonvulsant as well as analgesic effects. Large clinical studies have demonstrated its efficacy for treatment of patients with partial seizures. LCM is well tolerated, and the most common adverse events are unspecific central nervous system and gastrointestinal effects such as dizziness, vertigo, nausea, and headache. LCM is approved for treatment of partial seizures with or without secondary generalization in the India. Oral tablets (50mg,100mg,150mg,200mg),oral syrups/solutions(10-15mg/ml),and intravenous(IV)formulations available
Epilepsy is a frequent neurological disorder that is defined as the “… enduring predisposition of the brain to generate epileptic seizures …”. Usually, this definition is operationalized as the occurrence of two or more unprovoked seizures. Epidemiologic studies have shown that approximately 0.5% to 1% of the general population suffer from epilepsy,2,3 with annual incidence rates of approximately 30 to 50 per 100,000 per year, in total, over 10million to 12 million people currently live with the disorder nation wide. Epilepsy is not a distinct disease entity, but a common final pathway of a large variety of different etiologies. It can be described as the repetitive occurrence of abnormal bioelectrical synchronization of a large number of neurons leading to temporary dysfunction of one or more brain areas.
Epilepsy is classified primarily by where seizures begin in the brain. The four basic types are Focal (starts in one area)1, Generalized (affects both sides immediately)2, Combined Generalized & Focal3, and Unknown Onset4.
ANTIEPILEPTIC AGENTS:
Antiepileptic drugs (or antiseizure medications) manage epilepsy by restoring the balance between neuronal excitation and inhibition in the brain. They achieve this by suppressing abnormal, synchronous electrical discharges through three primary physiological mechanisms.
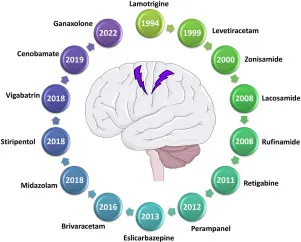
Fig:01Graphical presentation of antiepileptic drugs
Normal physiology of antiepileptics:
A seizure is the clinical manifestation of a hyperexcitable neuronal network, in which the electrical balance underlying normal neuronal activity is pathologically altered—excitation predominates over inhibition (see Basic Mechanisms syllabus). Effective seizure treatment generally augments inhibitory processes or opposes excitatory processes. Since the normal resting neuronal membrane potential is intracellularly negative, inhibitory processes make the neuron more electrically negative, hyperpolarizing the membrane, while excitatory processes make the intracellular potential less negative or more positive, depolarizing the cell. On an ionic level, inhibition is typically mediated by inward chloride or outward potassium currents, and excitation by inward sodium or calcium currents. Drugs can directly affect specific ion channels or indirectly influence synthesis, metabolism, or function of neurotransmitters or receptors that control channel opening and closing. The most important central nervous system inhibitory neurotransmitter is gamma-amino-butyric acid (GABA). The most important excitatory neurotransmitter is glutamate, acting through several receptors.
modulating voltage-gated ion channels1,
enhancing inhibitory GABAergic transmission2,
dampening excitatory glutamatergic transmission3,
modulating synaptic release machinery4
The applications of antiepileptic drugs (AEDs) is the mainstay of treatment for most patients. Although almost 50% of the patients become seizure free with the first AED regardless of the agent, a substantial proportion of patients still have inadequate seizure control in spite of treatment with currently available AEDs. Therefore, there is still a need for new AED with enhanced effectiveness, tolerability, and/or pharmacokinetic properties.
LACOSAMIDE (LCM):
Lacosamide is a “third-generation” antiepileptic(anticonvulsant) medication primarily used to treat focal (partial) seizures and primary generalized tonic-clonic seizures. It works by stabilizing electrically overactive nerves in the brain and is available as oral tablets, a liquid solution, and an intravenous (IV) injection. It is a functionalized amino acid derivative (N-acyl-alpha amino acid) that acts by selectively enhancing the slow inactivation of voltage-gated sodium channels in the brain. It stabilizes hyperexcitable neuronal membranes and prevents the spread of seizure activity through a unique dual
Lacosamide (LCM) is a novel AED that has recently been licensed for adjunctive therapy of partial or secondary generalized seizures in the India as well as many Asian countries. This review summarizes the available pharmacological and clinical data regarding this new agent.
MECHANISM ACTION OF LACOSAMIDE (LCM):
Lacosamide stabilizes hyperexcitable neuronal membranes and prevents the spread of seizure activity through a unique dual mechanism.
1.Enhancement of Slow Sodium Channel Inactivation: Unlike traditional sodium channel blockers that target fast inactivation, lacosamide selectively targets the slow inactivation state of voltage-gated sodium channels. By shifting the slow inactivation curve, it reduces the number of channels available to fire, thereby inhibiting repetitive neuronal firing without impairing normal physiological function.
2.Modulation of CRMP-2: Lacosamide binds to collapsin response mediator protein-2 (CRMP-2). While not fully understood, this interaction modulates neurotrophic and axonal growth signals, potentially contributing to neuronal plasticity and long-term seizure control.
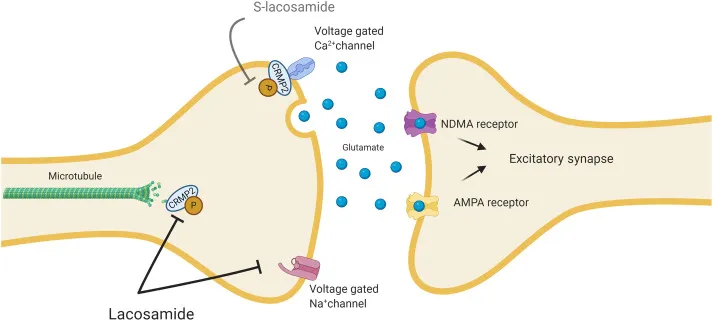
Fig 02. MECHANISAM OF LACOSAMIDE
CURRENTLY AVALIBLE ANTIEPILEPTIC DRUGS
The antiepileptic drugs (AEDs), now more commonly referred to as antiseizure medications (ASMs), work by stabilizing electrical activity in the brain to prevent seizures. They are broadly categorized into first-generation (older) and second/third-generation (newer) drugs, each tailored to specific seizure types and patient profilesThe anti-epileptic drugs that are in use are: levetiracetam, carbamazepine, ethosuximide, phenytoin, valproate.
Dosage of lacosamide
Monotherapy (used alone)
Initial dose: 100 mg twice daily,
Maintenance dose: 150–200 mg twice daily,
Maximum dose: 400 mg/day.
Adjunctive therapy (with other antiepileptic drugs)
Initial dose: 50 mg twice daily,
Maintenance dose: 100–200 mg twice daily,
Maximum dose: 400 mg/day.
Loading dose (if rapid seizure control needed)
200 mg once
After 12 hours: 100 mg twice daily.
PHARMACOKINETICS OF LACOSAMIDE:
It is available in both oral (tablet/oral solution) and intravenous (IV) formulations. The pharmacokinetic properties of both formulations are very similar, allowing easy conversion between routes.
1. Absorption:
Oral Lacosamide:
Rapidly and completely absorbed after oral administration.
Oral bioavailability is approximately 100%.
Peak plasma concentration (Tmax) occurs within 1–4 hours after dosing.
Food does not significantly affect absorption.
Exhibits negligible first-pass metabolism.
IV Lacosamide:
Directly enters systemic circulation, giving immediate availability.
Peak plasma concentration is reached at the end of infusion.
IV infusions over 30 or 60 minutes are bioequivalent to oral tablets.
IV formulation is commonly used when oral administration is temporarily not feasible.
2. Distribution:
Volume of distribution: approximately 0.6 L/kg.
Plasma protein binding is very low (<15%).
Crosses the blood–brain barrier effectively.
Low protein binding reduces clinically significant drug interactions.
3. Metabolism:
Undergoes limited hepatic metabolism.
Major metabolite:
O-desmethyl lacosamide (inactive metabolite).
Metabolism mainly involves:
CYP2C19
Minor roles of CYP3A4 and CYP2C9.
Minimal cytochrome P450 interaction contributes to a low interaction profile.
4. Elimination:
Eliminated mainly through kidneys.
About:
40% excreted unchanged in urine.
30% excreted as O-desmethyl metabolite.
Elimination half-life:
Approximately 12–13 hours.
Steady-state concentration achieved within about 3 days of twice-daily dosing.
ADVERSE EFFECTS OF LACOSAMIDE:
Common adverse effects
Dizziness, headache, vertigo, nausea and vomiting.
Cardiovascular adverse effects
Increased risk of “PR” interval prolongation, Bradycardia, Av block, Hypotension.
Neuro-psychiatric effects
Confusion, Depression.
Gastrointestinal effects
Dyspepsia, diarrhea.
DRUG INTERACTIONS OF LACOSAMIDE:
LACOSAMIDE WITH OTHER CARDIAC MEDICATIONS: If taking lacosamide along-side with cardiac medications like beta blockers, calcium channel blockers, anti-arrhythmia drugs, other sodium or potassium channel blockers. It can cause pr interval prolongation (a change in the heart`s electrical rhythm).
LACOSAMIDE & OTHER ANTI-EPILEPTICS: Taking lacosamide with phenytoin
&carbamazepine increases neurotoxic side effects like double vision &drowsiness.
ALCOHOL: Daily or excessive alcohol consumption while on lacosamide therapy which can cause excessive, dangerous levels of drowsiness &dizziness.
Natural Products & Grapefruit: Grapefruit and grapefruit products can block the enzymes that metabolize lacosamide, increasing drug levels in your body.
CLINICAL TRAILS OF LACOSAMIDE
Landmark lacosamide trails establish its critical role in medicine----shaping guidelines for epilepsy prevention,
Lacosamide (LCM) is an established anti-seizure medication (ASM) commonly used to treat partial-onset seizures, generalized tonic-clonic seizures, and status epilepticus. Its clinical efficacy, safety, and pharmacokinetics are extensively documented across multiple phase II and phase III randomized, double-blind, placebo-controlled trials. [1, 2, 3, 4]
Key clinical trials for Lacosamide can be categorized by the specific indication or study focus:
1. Pivotal Trials for Partial-Onset Seizures (Adults)
Landmark Phase II/III trials (SP667, SP754, SP755) established lacosamide's efficacy as an adjunctive treatment for focal seizures, supporting its regulatory approvals. [1, 2, 3]
2. Primary Generalized Tonic-Clonic Seizures (PGTCS)
Phase III trial (SP0982) demonstrated efficacy for primary generalized tonic-clonic seizures in patients 4 years and older. [1, 2]
3. Pediatric and Monotherapy Studies
4. Status Epilepticus and Nonconvulsive Seizures
5. Pooled Analyses and Systematic Reviews
AFTER ALL THIS TRAILS THE LACOSAMIDE SIGNFICANTLY STOPPED THE RISK OF SEIZURES.
MAJOR SAFETY RISK OF LACOSAMIDE:
CRITERIA OF AN IDEAL ANTIEPILEPTIC DRUG
An ideal antiepileptic drug (AED) for the Indian context must effectively control seizures while addressing India's unique socioeconomic and demographic realities. While no single drug perfectly meets every criterion, the ideal pharmacological profile balances high clinical efficacy with practical accessibility, affordability, and safety.
Broad-spectrum efficacy: Capable of controlling multiple seizure types (both focal and generalized) with a single medication, simplifying long-term management.
High seizure-freedom rate: Capable of rendering the patient seizure-free at tolerated doses.
Minimal cognitive and behavioral side effects: The drug should not cause sedation, memory impairment, or mood changes, allowing children to stay in school and adults to maintain employment.
Favorable pharmacokinetic profile: A long half-life to allow once- or twice-daily dosing, which drastically improves patient adherence.
Low teratogenicity: A safe profile for women of childbearing age, as the teratogenic (birth defect) risk is a major clinical concern.
No requirement for routine blood monitoring: It should not require frequent therapeutic drug monitoring (TDM), which reduces the financial burden on patients
High affordability: Low out-of-pocket costs, considering many patients in India payfor medication without medical insurance.
High availability and generic access: Wide availability in both urban and rural settings across India, ideally with generic options.
Low interaction with other drugs: Favorable interaction profile, which is critical given the high prevalence of concurrent conditions (like diabetes or hypertension) and the frequent use of complementary or alternative medicines.
Heat stability: The medication's chemical structure should remain stable in India’s varying and often high-temperature climates.
CONCLUSION
Lacosamide is approved for adjunctive treatment of partial-onset seizures in adult patients and is being investigated for treatment of pediatric patients and as monotherapy. It is being clinically evaluated for treatment of acute seizures. It has a unique sodium channel mechanism that appears to differentiate it from traditional AEDs such as oxcarbazepine and phenytoin. Pharmacodynamic interactions, however, often require that other sodium channel AEDs be reduced while titrating lacosamide to effective doses. Additional experience in large treatment populations is needed to verify the favorable safety profile of lacosamide. Lacosamide's safety during pregnancy also remains to be evaluated; optimal doses and titration schedules need also to be explored objectively in trials which do not require fixed doses of previous AEDs.
REFERENCES
Villanueva V, López-González FJ, Mauri JA, et al. Long-term safety and efficacy of lacosamide in patients with epilepsy. Acta Neurologica Scandinavica. 2014;130(6):403-411.

Dr. M. Prasada Rao, Dr. Y. Narasimha Rao, Dr. S. Rajini, G. Sampath, A Clinical Review on Role of Lacosimide as An Antiepileptic Agent , Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 5357-5263, https://doi.org/10.5281/zenodo.20772787
 10.5281/zenodo.20772787
10.5281/zenodo.20772787