
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmacy practice, Srinivas College of Pharmacy, Mangaluru, Karnataka-574143.
Gestational diabetes mellitus (GDM) poses a significant risk during pregnancy, necessitating strict adherence to prescribed medications to mitigate complications for both mother and child. This prospective interventional study spanned 6 months to assess the impact of a pharmaceutical care plan on managing diabetes in pregnant women. Medication adherence was analyzed by using the Morisky medication adherence scale -8 (MMAS-8). Data was collected from the patients; intervention was provided after 3 month and results were analyzed using Microsoft excel. Fifty participants with high adherence were eliminated out of a total of 100. The remaining 50 were divided equally between the intervention and control groups. The intervention group received Patient Information Leaflets (PIL) as part of their care regimen. While the control group showed no improvement, high adherence increased from 0% to 80?ter patient counseling and a leaflet were given to the intervention group. This study demonstrated the significant improvement in medication adherence among patients who received the intervention compared to those in the control group. Thus, the above result suggested the positive impact of clinical pharmacist intervention on GDM patients.
Pregnancy is the dynamic state in which women undergo number of adaptive changes (physiological and hormonal) that are necessary for the proper growth and development of the fetus. Various complications may arise during pregnancy among which most important complications are GDM and PIH. [1]
One of the most prevalent medical conditions that complicate pregnancy is gestational diabetes mellitus (GDM), and its prevalence among women in the reproductive age range is rising worldwide.[2] Insulin resistance in pregnant women is mainly due to hormonal changes, it happens due to an imbalance between levels of certain insulin or glucose affecting hormones in the body during pregnancy. [3]
In the past years, a number of studies have concluded that ‘tight’ glycaemia control throughout pregnancy in gestational diabetes mellitus (GDM) patients significantly reduces both foetal and maternal risk. [4]
Pharmaceutical care has been defined as the responsible provision of drug therapy for the purpose of achieving definite outcomes that enhance the patient’s quality of life It includes coordination between medical professionals, including a clinical pharmacist, and the patient to develop, carry out, and review a treatment plan. It also includes educating the patient on the disease diagnosis and prescription regimen. Pharmaceutical care requires pharmacist services to be “patient-centered” to detect actual drug problems, to resolve issues with inappropriate medications that have been prescribed, and to ultimately enhance patient outcomes. [5]
Nonadherence during pregnancy can raise the risk of hospitalization, increase healthcare costs, and create obstacles for both the mother and the fetus. Women tend to overestimate the teratogenic risk of medication, resulting in reluctance to use medication during pregnancy due to these concerns.
Patients’ adherence to medication is largely affected by their beliefs about medications, which in turn may be influenced by knowledge of drugs and their safety. On the other hand, poor knowledge of medication safety and restriction in pregnancy would lead to self-medication, poor drug use, and associated adverse effects, including foetal deformation, loss of wanted pregnancy, maternal bleeding, and even death. A high proportion of pregnant women use one or more drugs during pregnancy, including supplements and herbal medications the lack of understanding and adherence to medication restrictions can lead to negative health outcomes for both the mother and the baby. [6]
A multidisciplinary team must provide extra care for pregnant women with GDM. This includes constant education about GDM, treatment and, above all, continuing health education, aiming the self-care. Providing quality information and education during pregnancy is recommended to ensure health care for pregnant women and may help to reduce maternal morbidity and mortality. [7] A major part of managing GDM involves selective use of insulin therapy, educating the patient about diet, exercise, self-monitoring of blood glucose and insulin self-administration. Previous research has shown that patient education adds value to diabetes management and that specific interventions aimed at improving patient knowledge can enhance diabetes control and pregnancy outcomes.
2.0 OBJECTIVES OF THE STUDY
3.0 REVIEW OF LITERATURE
4.0 METHODOLOGY
MATERIALS AND METHODS
Study design: A hospital-based intervention study to identify medication adherence in pregnant women with gestational diabetes.
Study site: Srinivas Institute of Medical Science and Research Centre (SIMS & RC), Mukka-574146.
Sample Size: 100
Study duration: 6 months
Ethical Clearance: The study protocol was approved by the Institutional Ethics Committee (IEC) of Srinivas Institute of Medical Science, Mukka, Mangaluru. In addition, written informed consent was obtained from all the participants in this study. (Ref. No.: SIEC/SIMS & RC/53/03/2024)
Inclusion Criteria:
Exclusion Criteria:
Source of data collection:
4.1 THE STUDY PERIOD WAS DIVIDED INTO 3 PHASES
1) Phase 1: Preparation for the study:\
Data collection form: Included the patient’s demographic details, co-morbid diseases, laboratory details, treatment chart.
Assessment tools:
Morisky medication adherence scale-8 (MMAS-8)
Morisky medication adherence scale is a validated assessment tool which is used to check the adherence in the population. It consists of 8 questions with respective scores and as the score increases adherence and the maximum score that can be acquired is 8. It is divided into high adherence (=8), medium adherence (6-8) and low adherence (<6).
Patient were segregated based on inclusion and exclusion criteria
Informed consent form was obtained from the selected patient in English and Kannada.
Of 100 screened patients, 50 were excluded due to high adherence >8. The remaining 50 were randomized into:
DATA ANALYSIS
Statistical analysis involved collecting and scrutinizing every data sample in a set of items from which samples can be drawn and a suitable statistical test was applied to analyse the data. The collected data will be analyzed using Microsoft Excel.
5.0 RESULTS
ADHERENCE TO THE THERAPY AMONG PREGNANT WOMEN
Medication adherence of each study subject was recorded using Morisky medication adherence scale-8 (MMAS-8) with the information obtained from the patients. Morisky medication adherence scale is a validated assessment tool which is used to check the adherence in the population. It consists of 8 questions with respective scores and as the score increases adherence and the maximum score that can be acquired is 8. It is divided into high adherence (=8), medium adherence (6<8) and low adherence (<6). On assessing the baseline adherence of the study population, out of 100 GDM patients, 33% subjects had low adherence,17% subjects had medium adherence and 50% subjects had high adherence respectively.
Table 1. Adherence to the therapy among pregnant women
|
MMAS-8 |
N=100 |
|
Low adherence (<6 scores) |
33 (33%) |
|
Medium adherence (6-8 scores) |
17 (17%) |
|
High adherence (8 score) |
50 (50%) |

Figure 1: Adherence to the therapy in 100 subjects
MORISKY MEDICATION ADHERENCE SCALE -8
Among 100 subjects, 50 individuals were excluded who demonstrated high adherence to medication. With 50 subjects remaining, was further divided into control group and an intervention group. The control group did not receive any specific intervention and will serve as a baseline for comparison. Meanwhile, the intervention group received targeted intervention in the form of PIL and patient counseling designed to enhance medication adherence. Among 25 subjects in each group during the pre-test both groups had no high adherent subjects, 8 subjects had medium adherence in control group,9 subjects in the intervention group during the pre- test and 17 subjects had low adherence in control group, 16 subjects in the intervention group during the pre-test. After the intervention phase when comparing the control and intervention groups, it's evident that the intervention had a notable impact on adherence levels. In the intervention group, there was a marked increase in high adherence post-test 20 subjects, 3 subjects with the medium adherence and 2 subjects with the low adherence. Whereas the control group remained unchanged. Additionally, the intervention group showed more participants achieving high adherence in the post-test compared to the control group, indicating the effectiveness of the intervention in promoting better adherence outcomes. This observation was found significant with the help of unpaired t-test where p value was less than 0.05.
Table 2. Morisky medication adherence scale-8
|
|
|
Intervention group (n=25) |
Control group (n=25) |
||||||
|
|
|
PRE |
POST |
PRE |
POST |
||||
|
NO |
QUESTION |
YES |
NO |
YES |
NO |
YES |
NO |
YES |
NO |
|
1. |
Do you sometimes forget to take your medications? |
21 (84%) |
4 (16%) |
3 (12%) |
22 (88%) |
17 (68%) |
8 (32%) |
14 (56%) |
11 (44%) |
|
2. |
In the past 2 weeks, were there any days when you did not take your medications? |
18 (72%) |
7 (28%) |
5 (20%) |
20 (80%) |
18 (72%) |
7 (28%) |
5 (20%) |
20 (80%) |
|
3. |
Have you ever stopped your medications without telling your doctor, because you felt worse when you took it? |
15 (60%) |
10 (40%) |
2 (8%) |
23 (92%) |
14 (56%) |
11 (44%) |
14 (56%) |
11 (44%) |
|
4. |
When you travel or leave home, do you sometimes forget to bring along your medication? |
23 (92%) |
2 (8%) |
4 (16%) |
21 (84%) |
21 (84%) |
4 (16%) |
21 (84%) |
4 (16%) |
|
5. |
Did you take your medication yesterday? |
14 (56%) |
11 (44%) |
23 (22%) |
2 (8%) |
17 (68%) |
8 (32%) |
10 (40%) |
15 (60%) |
|
6. |
When your health condition is under control, do you sometimes stop taking your medications? |
17 (68%) |
8 (32%) |
2 (8%) |
23 (92%) |
20 (80%) |
5 (20%) |
20 (80%) |
5 (20%) |
|
7. |
Do you feel hassled about sticking to your treatment plan? |
17 (68%) |
8 (32%) |
4 (16%) |
21 (84%) |
19 (76%) |
6 (24%) |
5 (20%) |
20 (80%) |
|
8. |
How often do you have difficulty in remembering to take all your medication? |
||||||||
|
|
a) Never/Rarely (1) |
21 (84%) |
4 (16%) |
6 (24%) |
19 (76%) |
19 (76%) |
5 (20%) |
19 (76%) |
5 (20%) |
|
|
b) Once in a while (0.75) |
16 (64%) |
9 (36%) |
4 (16%) |
21 (84%) |
14 (56%) |
11 (44%) |
14 (56%) |
11 (44%) |
|
|
c)Sometimes (0.75) |
18 (72%) |
7 (28%) |
3 (12%) |
22 (88%) |
12 (48%) |
13 (52%) |
12 (48%) |
13 (48%) |
|
|
d) usually (0.25) |
11 (44%) |
14 (56%) |
2 (8%) |
24 (94%) |
8 (32%) |
17 (68%) |
8 (32%) |
17 (68%) |
|
|
e) All the time (0) |
12 (48%) |
13 (52%) |
1 (4%) |
24 (94%) |
6 (24%) |
19 (76%) |
6 (24%) |
19 (76%) |
Table 3. Adherence to the therapy in control group and Intervention group
|
Medication adherence level |
Intervention group |
Control group |
p Value |
||
|
|
Pre |
Post |
Pre |
Post |
|
|
Low adherence <6 |
16 |
2 |
17 |
14 |
< 0.05 |
|
Medium adherence 6-8 |
9 |
3 |
8 |
10 |
< 0.05 |
|
High adherence ≥8 |
0 |
20 |
0 |
1 |
<0.05 |

Figure 2: Adherence to the therapy in intervention group
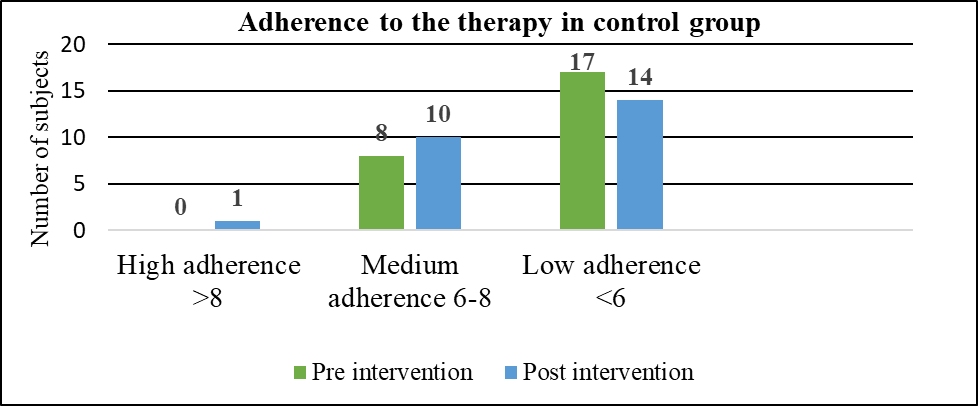
Figure 3: Adherence to the therapy in control group
REASONS FOR NON- ADHERENCE

Figure 4: Reasons for non-adherence among the study subjects
6.0 DISCUSSION
The study was carried out on 100 pregnant women with gestational diabetes mellitus in tertiary care hospitals.
On assessing the baseline adherence out of 100 patients, more than half of the pregnant women had good adherence (50%), A study by Lash KA et al., showed that (53%) of pregnant women have high medication adherence. [9] 15% of the patients had medium adherence and 35% patients had low adherence respectively. the subjects with medium adherence (33%) and low adherence (17%) were further randomly divided. At the end of the study showed a significant change in improving medication adherence i.e the control group showed no improvement however there was a drastic improvement in the intervention group patients that is 20 patients (80%) with high adherence,3 patients (12%) with medium adherence, and 2 patients (8%) with low adherence, which was similar to a study conducted by Cani CG, Lopes LD, et al., Diabetes-related quality of life significantly improved in the intervention group but worsened significantly in the control group. [6] It was found that the most common reason for low adherence was forgetfulness of any type, cost of the drug, and unavailability of a particular brand, which was similar to a study conducted by Asiedu-Danso et al., Adherence to anti-diabetic medications among women with gestational diabetes [13]. This study concludes that pharmacists play a crucial role in enhancing patient outcomes through targeted pharmaceutical care interventions. By focusing on education, medication management, and personalized patient counseling, pharmacists significantly improve health outcomes across various patient populations.
Thus, the impact of counseling on the management of gestational diabetes in pregnant women is substantial and multifaceted. Patient education interventions effectively improve quality of life by reducing the burden of diabetes symptoms and treatment, enhance adherence to prescribed therapies, empower women with knowledge and positive health behaviors, and minimize drug-related complications. Overall, patient education emerges as a critical component in achieving better maternal and fetal health outcomes during pregnancy, emphasizing the importance of comprehensive support and education in gestational diabetes care.
7.0 CONCLUSION
The study also highlights the potential benefits of interventions aimed at improving medication adherence among pregnant women. By promoting medication adherence during pregnancy, healthcare providers can help optimize maternal and fetal health outcomes and improve the overall quality of care. Through patient education, pharmacists can ensure that pregnant women have a clear understanding of their medication regimen, including the importance of adherence and potential risks and benefits. Pharmacists can also provide education to address concerns or misconceptions about medication safety during pregnancy, helping to alleviate fears and promote confidence in medication use. Thus, the above result shows the positive impact of clinical pharmacist intervention on GDM patients. A Patient Information Leaflet (PIL) serves as an educational tool designed to impart essential information to patients about their specific disease, medications prescribed, and necessary lifestyle modifications. PIL was found to be adequate in improving the quality of life in diabetes at the altered level. The results of the study demonstrated that the patients who were provided with PIL during the intervention phase reported overall excellent diabetes -related quality of life.
ACKNOWLEDGEMENTS:
I sincerely thank Dr. Krishnananda Kamath K, my guide, and Dr. Blessy Fernandes, my co-guide, for their invaluable guidance, support, and encouragement throughout this research work. I express my deep gratitude to Dr. A. R. Shabaraya, Principal, for providing the necessary resources and constant motivation to carry out this study. I extend my heartfelt thanks to Srinivas College of Pharmacy and SIMS & RC for providing the opportunity and facilities essential for this research. I am also grateful to all the faculty members, staff, parents, friends, and study participants for their constant support and contribution, which made this work possible.
REFERENCES


Shynia Neola Dsouza, Krishnananda Kamath K, Blessy Fernandes, A.R. Shabaraya, A Hospital-Based Intervention Study to Identify Medication Adherence in Pregnant Women with Gestational Diabetes, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 1352-1361. https://doi.org/10.5281/zenodo.17571109
 10.5281/zenodo.17571109
10.5281/zenodo.17571109