
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Doctor Of Pharmacy, Met’s Institute Of Pharmacy Adgaon, Nashik.
Background: Pyelonephritis is a common and potentially serious bacterial infection of the renal parenchyma and pelvis that can lead to significant morbidity if not diagnosed and treated promptly. The disease is frequently associated with risk factors such as urinary tract obstruction, catheterization, recurrent urinary tract infections, and renal calculi. Understanding the clinical presentation, risk factors, complications, and treatment patterns is essential for improving patient outcomes.Objective: To evaluate the demographic characteristics, clinical manifestations, risk factors, complications, and antibiotic treatment patterns among patients diagnosed with pyelonephritis in a tertiary care hospital setting. Methodology: A prospective observational study was conducted at NAMCO Hospital, Nashik, over a period of six months (November 2024–April 2025). A total of 160 patients aged 20 years and above with confirmed pyelonephritis were included in the study. Patient demographic data, clinical symptoms, risk factors, complications, and treatment details were collected using a structured data collection form and analyzed using descriptive statistics. Results: The mean age of the study population was 51.01 ± 18.98 years, with females constituting 58.75% of the cases. The most common clinical presentation was uni/bilateral loin pain (41.25%), followed by increased urinary frequency (36.88%), pedal edema (35.63%), hematuria (34.38%), fever (33.75%), flank pain (33.75%), vomiting (33.75%), dysuria (33.13%), nausea (33.13%), and burning micturition (32.50%). Major risk factors identified were catheterization (44.38%), kidney stones (39.38%), chronic urinary tract infection (34.38%), and prostate enlargement (33.13%). Most patients (60%) experienced no complications; however, sepsis (15.63%), kidney scarring (13.13%), kidney abscess (7.50%), and renal failure (3.75%) were observed. Ciprofloxacin (26.92%) was the most commonly prescribed single antibiotic, while the combination of gentamicin and meropenem (21.78%) was the most frequently used combination therapy. Conclusion: Pyelonephritis predominantly affected middle-aged adults and females in this study. Catheterization and renal calculi were the most significant risk factors. Although most patients recovered without complications, sepsis remained a notable adverse outcome. The findings emphasize the importance of early diagnosis, appropriate antibiotic selection, risk factor management, and antimicrobial stewardship to improve clinical outcomes and reduce complications associated with pyelonephritis
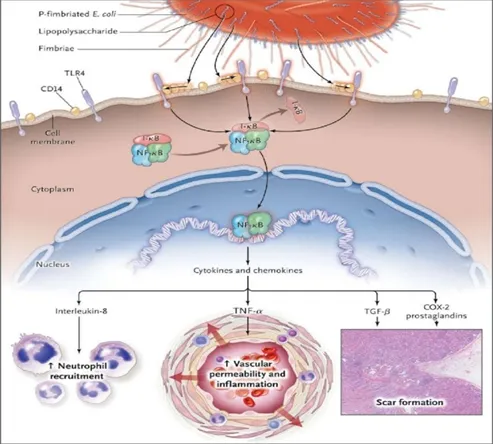
Pyelonephritis is a bacterial infection of the kidneys characterized by inflammation of the renal parenchyma and renal pelvis. It is one of the most serious forms of urinary tract infection (UTI) and commonly occurs when microorganisms ascend from the lower urinary tract to the kidneys. Acute pyelonephritis is a significant cause of morbidity worldwide and may lead to severe complications such as sepsis, renal abscess, renal scarring, and renal failure if not diagnosed and treated promptly. Women are affected more frequently than men due to anatomical factors, including a shorter urethra and the close proximity of the urethral opening to the perianal region, which facilitates bacterial colonization and ascent.
The most common causative organism of pyelonephritis is Escherichia coli, accounting for the majority of community-acquired infections. Other pathogens such as Klebsiella pneumoniae, Proteus mirabilis, Pseudomonas aeruginosa, and Enterococcus species may also be responsible, particularly in complicated cases or healthcare-associated infections. The disease typically presents with symptoms including fever, flank pain, loin pain, nausea, vomiting, dysuria, urinary frequency, hematuria, and general malaise. Early recognition of these symptoms is essential for timely intervention and prevention of complications.
Several risk factors contribute to the development of pyelonephritis. These include urinary tract obstruction, kidney stones, vesicoureteral reflux, urinary catheterization, recurrent urinary tract infections, diabetes mellitus, immunosuppression, and structural abnormalities of the urinary tract. Catheter-associated urinary tract infections are particularly important in hospitalized patients and significantly increase the risk of ascending kidney infections. In addition, the growing prevalence of antimicrobial resistance among common uropathogens has become a major challenge in the management of pyelonephritis.
Diagnosis of pyelonephritis is based on clinical presentation, laboratory investigations, urine culture and sensitivity testing, and imaging studies when indicated. Prompt initiation of appropriate antimicrobial therapy remains the cornerstone of treatment. However, increasing resistance to commonly used antibiotics such as fluoroquinolones and cephalosporins necessitates careful antibiotic selection based on local susceptibility patterns and culture reports.
Despite advances in diagnosis and treatment, pyelonephritis continues to pose a significant healthcare burden due to its recurrence, complications, and rising antimicrobial resistance. Therefore, understanding the demographic characteristics, clinical manifestations, risk factors, complications, and treatment outcomes of pyelonephritis is essential for improving patient care. This study was conducted to evaluate these factors among patients diagnosed with pyelonephritis in a tertiary care hospital setting and to contribute to evidence-based management strategies for better clinical outcomes.
AIM AND OBJECTIVES
AIM: To evaluate the clinical presentations of patients diagnosed with pyelonephritis and Identify variations in treatment in a hospital.
OBJECTIVES:
• To assess the effectiveness of current treatment approaches and Identify Risk Factors.
• To analyze key risk factors, including gender, age, comorbidities.
NEED OF STUDY
NEED FOR THE STUDY
In resource-limited settings like India, it is crucial to identify cost-effective and evidence-based approaches for the prevention, diagnosis, and management of pyelonephritis. Conducting an observational study can guide the formulation of region-specific clinical guidelines and optimize the use of limited healthcare resources.
By identifying modifiable risk factors and assessing the effectiveness of current treatment protocols, this study aims to contribute toward reducing the incidence and severity of pyelonephritis cases. Ultimately, this will alleviate the burden on already overstretched healthcare systems and improve patient outcomes.
Pyelonephritis contributes to increased hospital admissions, extended duration of treatments, and a substantial rise in overall healthcare costs. Understanding the risk factors and current management strategies can help in streamlining care and reducing unnecessary healthcare expenditures.
METHODOLOGY
MATERIALS AND METHODS
Study Design: Prospective observational study
Site: NAMCO Hospital, Nashik
Study Duration: 6 Months (November 2024 – April 2025)
Inclusion Criteria:
1. Age: Patients aged 20 years or older.
2. Diagnosis: Patients with a confirmed diagnosis of pyelonephritis, based on laboratory reports.
3. Symptoms: Patients presenting with symptoms consistent with pyelonephritis.
4. Imaging studies: Patients with imaging studies consistent with pyelonephritis, such as ultrasound or computed tomography scans showing evidence of kidney infection.
Exclusion Criteria:
1. Age: Patients under 20 years old.
2. Pregnancy: Pregnant women, as the diagnosis and management of pyelonephritis may differ in this population.
3. Immunocompromised status: Patients with immunocompromised status, such as those with HIV/AIDS or undergoing chemotherapy, as they may be at increased risk of complications.
4. Chronic kidney disease: Patients with chronic kidney disease, as the diagnosis and management of pyelonephritis may differ in this population.
Sample Size: n=160
METHODOLOGY
Study Tools:
• Data Collection: Patients’ data including demographic, past medical and medication history, present medication and other parameters that are available will be collected in a structured data collection from.
• The subjects will be included in the study only after obtaining the inform consent form (ICF).
Statistical Analysis of Results:
? The collected data was be cleaned, validated, coded and entered in Microsoft Excel sheet.
? Descriptive analysis of Age, Height, BMI, and Lab parameters were done using mean, SD, Median and Frequency and percentage.
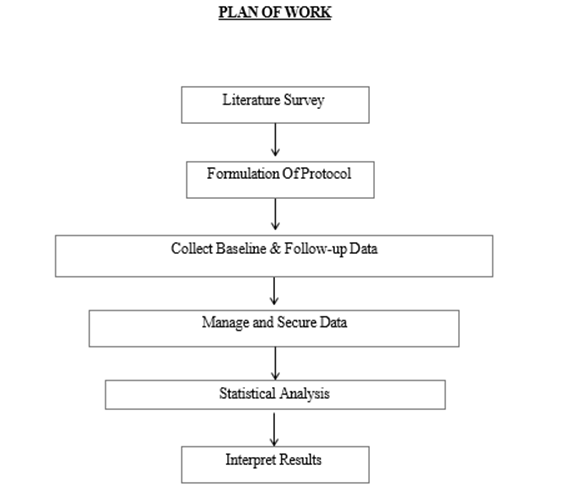
PLAN OF WORK
RESULTS
Table 1. Descriptive analysis.
|
Descriptive Statistics |
N |
Mean |
Std. Deviation |
|
Age |
160 |
51.01 |
18.98 |
The descriptive statistics indicate that the study population consisted of 160 individuals, with a mean age of 51.01 years and a standard deviation of 18.98 years (Table 1.).
Table 2. Distribution of the patients according to gender.
|
Gender |
Frequency |
Percent |
|
Male |
66 |
41.25 |
|
female |
94 |
58.75 |
Out of the total 160 participants, 66 were male (41.25%) and 94 were female (58.75%) (Table 2.).
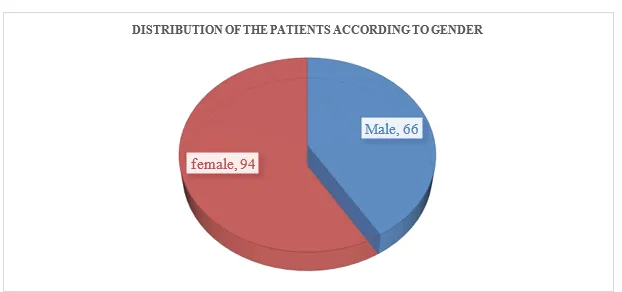
Graph 1. Distribution of the patients according to gender
Table 3. Distribution of the patients according to symptoms.
|
Symptoms |
Frequency |
Percentage |
|
Fever |
54 |
33.75 |
|
Flank Pain |
54 |
33.75 |
|
Uni/Bilateral Loin pain |
66 |
41.25 |
|
Nausea |
53 |
33.13 |
|
Vomiting |
54 |
33.75 |
|
Burning Micturation |
52 |
32.50 |
|
Increase Urine Frequency |
59 |
36.88 |
|
Dysuria |
53 |
33.13 |
|
Hematuria |
55 |
34.38 |
|
Pedal Edema |
57 |
35.63 |
Among the 160 participants, the most commonly reported symptom was uni/bilateral loin pain, observed in 66 individuals (41.25%). Increased urinary frequency was reported by 59 participants (36.88%), followed by pedal edema in 57 (35.63%) and hematuria in 55 (34.38%). Fever, flank pain, and vomiting were each reported by 54 participants (33.75%), while dysuria and nausea were present
in 53 individuals each (33.13%). Burning micturition was noted in 52 participants (32.50%) (Table 3.).
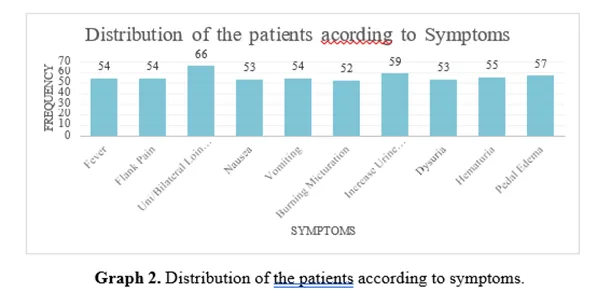
Table 4. Assessment of risk factors.
|
Risk Factors |
Frequency |
Percent |
|
Chronic UTI |
55 |
34.38 |
|
Kidney Stone |
63 |
39.38 |
|
Catheterization |
71 |
44.38 |
|
Prostate Enlargement |
53 |
33.13 |
Assessment of the risk factors in our study, the most frequently observed risk factor was catheterization, reported in 71 individuals (44.38%). This was followed by the presence of kidney stones in 63 participants (39.38%) and a history of chronic urinary tract infection (UTI) in 55 (34.38%). Prostate enlargement was identified in 53 participants (33.13%) (Table 4.).
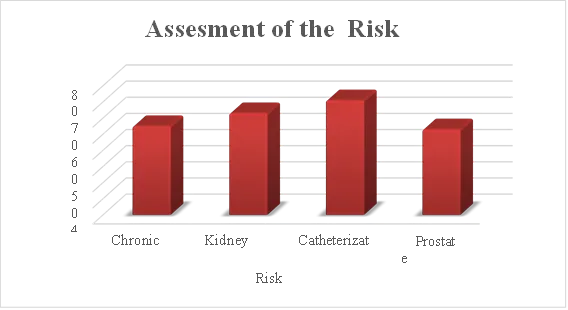
Graph 3. Assessment of risk factors.
Table 5. Analysis of the complications.
|
Complications |
Frequency |
Percent |
|
Kidney abscess |
12 |
7.50 |
|
Kidney scarring |
21 |
13.13 |
|
Renal Failure |
6 |
3.75 |
|
Sepsis |
25 |
15.63 |
|
None |
96 |
60.00 |
Analysis of the complications in our study population (Table 5.), 96 individuals (60.00%) did not develop any complications. However, sepsis was the most commonly reported complication, observed in 25 participants (15.63%), followed by kidney scarring in 21 (13.13%) and kidney abscess in 12 (7.50%). Renal failure was noted in 6 participants (3.75%).
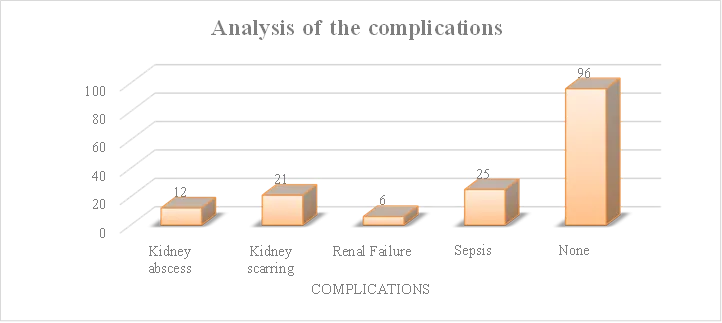
Graph 4. Analysis of the complications.
Table 6. Evaluation of the single antibiotic therapy.
|
Single Therapy |
Frequency |
Percent |
|
Amoxicillin-clavulanate |
9 |
11.54 |
|
Ceftriaxone |
10 |
12.82 |
|
Ciprofloxacin |
21 |
26.92 |
|
Gentamicin |
10 |
12.82 |
|
Meropenem |
17 |
21.79 |
|
Piperacillin-tazobactam |
11 |
14.10 |
|
Total |
78 |
100.00 |
Out of total prescriptions received, the 78 prescriptions who received single antibiotic therapy, ciprofloxacin was the most frequently administered agent, prescribed to 21 individuals (26.92%). This was followed by meropenem in 17 participants (21.79%) and piperacillin-tazobactam in 11 (14.10%). Ceftriaxone and gentamicin were each used in 10 participants (12.82%), while amoxicillin-clavulanate was given to 9 individuals (11.54%) (Table 6.).
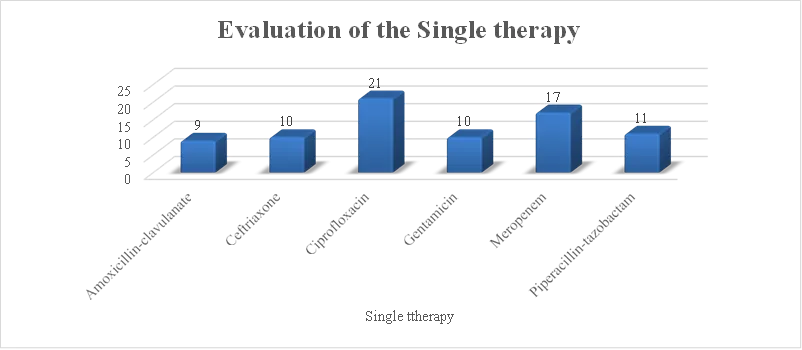
Graph 5. Evaluation of the single antibiotic therapy.
Table 7. Evaluation of combined antibiotic therapy
|
Combination Therpay |
Frequency |
Percent |
|
Amoxicillin-clavulanate, Ceftriaxone |
1 |
0.99 |
|
Amoxicillin-clavulanate, Ciprofloxacin |
7 |
6.93 |
|
Amoxicillin-clavulanate, Gentamicin |
4 |
3.96 |
|
Amoxicillin-clavulanate, Piperacillin-tazobactam |
8 |
7.92 |
|
Ceftriaxone, Ciprofloxacin |
6 |
5.94 |
|
Ceftriaxone, Gentamicin |
8 |
7.92 |
|
Ceftriaxone, Meropenem |
6 |
5.94 |
|
Ceftriaxone, Piperacillin-tazobactam |
8 |
7.92 |
|
Ciprofloxacin, Gentamicin |
6 |
5.94 |
|
Ciprofloxacin, Meropenem |
3 |
2.97 |
|
Ciprofloxacin, Piperacillin-tazobactam |
5 |
4.95 |
|
Gentamicin, Meropenem |
22 |
21.78 |
|
Gentamicin, Piperacillin-tazobactam |
7 |
6.93 |
|
Meropenem, Amoxicillin-clavulanate |
6 |
5.94 |
|
Meropenem, Piperacillin-tazobactam |
4 |
3.96 |
|
Total |
101 |
100.00 |
The 101 prescriptions who received combination antibiotic therapy, the most frequently used regimen was gentamicin with meropenem, administered to 22 individuals (21.78%). This was followed by combinations of amoxicillin-clavulanate with piperacillin-tazobactam, ceftriaxone with gentamicin, and ceftriaxone with piperacillin-tazobactam—each given to 8 participants (7.92%). Amoxicillin-clavulanate with ciprofloxacin and gentamicin with piperacillin-tazobactam were each used in 7 participants (6.93%). Several other combinations, such as ceftriaxone with ciprofloxacin, ciprofloxacin with gentamicin, and meropenem with amoxicillin-clavulanate, were employed less frequently (Table 6.).
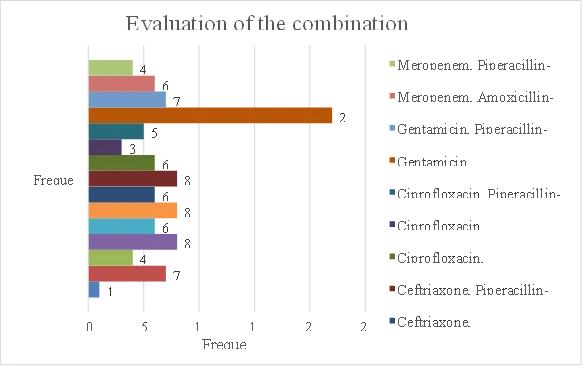
Graph 6. Evaluation of the combination antibiotic therapy.
DISCUSSION
Pyelonephritis is a bacterial infection causing inflammation of the kidneys. This condition frequently develops as a complication of urinary tract infections that ascend to the kidneys. Pyelonephritis presents in both acute and complicated forms, with complicated pyelonephritis specifically defined to include patients with conditions such as immunosuppression, diabetes mellitus, acute or chronic kidney failure, or hospital-acquired conditions, among others. It is important to differentiate complicated from uncomplicated pyelonephritis, as patient management approaches depend on this distinction. Acute pyelonephritis is a common cause for hospital admission and can lead to bacterial resistance, making treatment challenging (1). This prospective observational study was undertaken to evaluate the clinical characteristics, treatment, and prognosis in patients diagnosed with complicated pyelonephritis. Conducted in the Nephrology unit of a tertiary care hospital, the study found that the majority of patients fell into the 41-50 age group, with females potentially more susceptible due to a shorter urethral length (1,8). Acute Kidney Injury was identified as a significant complication in the patient cohort. Furthermore, most patients presented with multiple symptoms, including the most commonly observed triad of fever, nausea/vomiting, and decreased urine output.
The mean age of patients in our study was found to be 51.01 ± 18.98 years (Table 1.). This demographic profile is consistent with several other studies on
pyelonephritis in adult populations. For instance, Hase et al. (2021) (6) reported a similar mean age of 50.33 ± 13.9 years in their prospective observational study of predominantly complicated acute pyelonephritis in North India. A cross-sectional study on acute pyelonephritis by Shafi PKM and Rosh P. (2020) (3) also noted a comparable mean age of 52.16 ± 17.81 years, with the age groups of 40-49 and 50-59 years being the most frequently represented. Similarly, Bosch-Nicolau et al. (2017) (2) found a mean age of 53.9 ± 23.5 years in their cohort of acute pyelonephritis patients. While some studies, such as the large prospective study by Buonaiuto et al. (2014) (4) focusing on complicated pyelonephritis, reported a higher median age of 63 years, the mean age observed in the current cohort falls within the range reported by other recent investigations into the clinical and epidemiological characteristics of pyelonephritis.
In our study, females constituted the majority of the patient cohort, accounting for 94 out of 160 patients (58.75%), while males comprised 66 patients (41.25%) (Table 2.). This distribution is consistent with several other investigations into the epidemiology of pyelonephritis. For instance, a cross-sectional study by Shafi PKM and Rosh P. (2020) (3) similarly reported a female majority, with 60% of their 100 acute pyelonephritis patients being female. Eby Mathew et al. (2024)
(7) also found a slightly higher proportion of females (53.9%) in their cohort of acute pyelonephritis patients. While Bosch-Nicolau et al. (2017) (2) observed a more pronounced female predominance (85.3%) in their overall study of acute
pyelonephritis, they noted that the proportion of males was significantly higher in healthcare-associated cases compared to community-acquired cases, potentially due to factors like prostatic obstructive uropathy. Conversely, Hase et al. (2021) (6) reported a male predominance (61.8%) in their North Indian cohort, which predominantly included patients with complicated acute pyelonephritis. However, a large prospective study specifically on complicated pyelonephritis by Buonaiuto et al. (2014) (4) found a more balanced sex distribution, with men accounting for 52% and women 48% of their 1325 patients, noting that pyelonephritis in men is generally considered complicated.
In our study findings, various symptoms were reported with differing frequencies. Uni/bilateral loin pain was observed in 41.25% of patients, while fever, flank pain, and vomiting were each present in 33.75% of cases. Nausea and dysuria were noted in 33.13%, burning micturition in 32.50%, increased urine frequency in 36.88%, haematuria in 34.38%, and pedal oedema in 35.63%. While loin pain was the most frequent symptom in this study, other investigations have reported higher prevalences for symptoms such as fever and flank pain (Table 3.). For example, Hase et al. (2021) (6) found fever in 90% and flank pain/renal angle tenderness in 71.91% of their acute pyelonephritis cohort, which included a large proportion of complicated cases. Similarly, Eby Mathew et al. (2024) (7) noted loin pain in 80% and fever in 58%. Lower urinary tract symptoms (LUTS) are also commonly associated with pyelonephritis. Shafi PKM and Rosh P. (2020)
(3) reported dysuria in 82% and increased frequency in 65% of their acute pyelonephritis patients, figures considerably higher than the rates observed in the current study (dysuria 33.13%, increased frequency 36.88%). Burning micturition was also less frequent in this cohort (32.50%) compared to the high dysuria rate reported by Shafi PKM and Rosh P. (2020) (3). The presence of symptoms like nausea and vomiting (33.13% and 33.75% respectively) aligns with their identification as components of a commonly seen triad alongside fever in the present studys source document, although the classic triad of fever, flank pain, and dysuria was reported less frequently (30.33%) in the study by Hase et al. (2021) (6). Other symptoms such as haematuria (34.38%) and pedal oedema (35.63%) were also present in a notable proportion of the current cohort. Haematuria was observed in 10% of patients by Shafi PKM and Rosh P. (2020) (3), which is lower than the 34.38% noted in the current study.
Several known risk factors for pyelonephritis were prevalent in our study. Catheterization was the most frequently reported risk factor, affecting 71 patients (44.38%), followed by kidney stones in 63 patients (39.38%). Chronic UTI was present in 55 patients (34.38%), and prostate enlargement in 53 patients (33.13%) (Table 4.). The observed frequency of catheterization (44.38%) in this study is notably higher than the 14% reported by Shafi PKM and Rosh P. (2020) (3) in their acute pyelonephritis cohort, and the 9.6% for long-term bladder catheterization or 11.5% for urinary tract instrumentation described by
Buonaiuto et al. (2014) (4) in a large study of complicated pyelonephritis. However, Bosch-Nicolau et al. (2017) (2) found that 52.9% of patients with healthcare-associated acute pyelonephritis, which frequently involves complicated cases, had a chronic urinary catheter. Renal calculi were present in 39.38% of the current cohort, a higher proportion than the 25.5% reported by Buonaiuto et al. (2014) (4), the 24.71% noted by Hase et al. (2021), and the 19% found by Shafi PKM and Rosh P. (2020) (3). Chronic or recurrent urinary tract infections affected 34.38% of patients in this study, comparable to the 37.07% reported by Hase et al. (2021) (6), but lower than the 44% incidence observed by Shafi PKM and Rosh P. (2020) (3). Buonaiuto et al. (2014) (4) reported recurrent lower UTI in 23.3% of their complicated pyelonephritis patients, while Bosch-Nicolau et al. (2017) (2) noted recurrent UTIs in 24.5% of community-acquired cases and 56.5% of healthcare-associated cases. Prostate enlargement was a risk factor for 33.13% of the cohort, primarily affecting males. This figure is higher than the 15.3% prevalence reported by Buonaiuto et al. (2014) (4) for benign prostatic hyperplasia and the 13% noted by Shafi PKM and Rosh P. (2020) (3). These findings highlight the diverse range and significant prevalence of underlying urological and medical conditions that contribute to the complexity of pyelonephritis in the studied population.
The most frequently observed complications in our study were sepsis (15.63%) and kidney scarring (13.13%), followed by kidney abscess (7.50%) and renal
failure (3.75%). Notably, 60.00% of patients did not exhibit these specific complications (Table 5.). While "complicated pyelonephritis" is often defined by underlying patient conditions or urological abnormalities rather than solely by the presence of these severe clinical sequelae, the prevalence of these complications in the studied population provides insight into the disease severity. The reported rate of sepsis (15.63%) in this study is comparable to the 14% incidence of septic shock reported by Shafi PKM and Rosh P. (2020) (3) and the 12.5% incidence of septic shock in a large cohort of complicated pyelonephritis patients studied by Buonaiuto et al. (2014) (4), who also noted severe sepsis in 25.9% of cases. Bosch-Nicolau et al. (2017) (2) reported septic shock in 7.4% of community-acquired and 4.2% of healthcare-associated acute pyelonephritis cases, though noted similar frequencies in both groups. The incidence of acute kidney injury (AKI), which can contribute to renal failure and potentially long-term scarring, was remarkably high in some comparative studies, reaching 96.8% in the cohort evaluated by Eby Mathew et al. (2024) (7) and 41% in the study by Shafi PKM and Rosh P. (2020) (3). Both AKI and pre-existing chronic kidney disease (CKD) were significantly associated with poor renal outcomes in the study by Eby Mathew et al. (2024) (7). Kidney or renal abscesses were observed in 7.50% of patients in this study, a figure slightly lower than the 9.7% reported by Buonaiuto et al. (2014) (4) based on CT findings and the 8% reported by Shafi PKM and Rosh P. (2020) (3), but higher than the 1.6% noted by Eby Mathew et al. (2024)
(7) and the 5.6% reported by Hase et al. (2021) (6). While kidney scarring is a long-term consequence, the observed rate of renal failure (3.75%) aligns with the potential for significant renal damage in a proportion of patients. The presence of these complications, particularly sepsis and renal dysfunction, underscores the significant morbidity associated with complicated pyelonephritis.
The distribution of single antibiotic therapies administered to the cohort highlights the varied approaches to managing pyelonephritis in this setting. Ciprofloxacin was the most frequently employed single agent, used in 26.92% of cases, followed by Meropenem in 21.79% and Piperacillin-tazobactam in 14.10%. Ceftriaxone and Gentamicin were each utilised in 12.82% of patients, while Amoxicillin-clavulanate was given to 11.54% (Table 6.). Comparing this to other studies, a cross-sectional study by Shafi PKM and Rosh P. (2020) (3) on acute pyelonephritis reported Ciprofloxacin as the most common empirical antibiotic (54%), although Piperacillin–tazobactam was also widely used empirically (35%). Shafi PKM and Rosh P. (2020) (3) further noted that 85% of isolated organisms in their study were sensitive to Piperacillin–tazobactam, suggesting its potential as a first-line empirical option. Resistance to Ciprofloxacin is a significant concern documented in the literature; Shafi PKM and Rosh P. (2020) (3) found resistance rates of 68% to Ciprofloxacin, and Hase et al. (2021) (6) reported 92.30% resistance for E. coli isolates to quinolones, leading to high empirical treatment failure rates with Ciprofloxacin (70.37%).
The notable use of Meropenem and Piperacillin-tazobactam in the current cohort (21.79% and 14.10% respectively) aligns with guidance recommending broader spectrum agents for patients with sepsis or risk factors for multidrug-resistant organisms, which are common in complicated pyelonephritis. Carbapenems (including Meropenem), and Piperacillin/tazobactam, are active against ESBL-producing organisms, and studies by Hase et al. (2021) (6) confirm good sensitivity of ESBL producers to carbapenems. Gentamicin, an aminoglycoside, is another parenteral option recommended for initial dosing, or daily therapy in hospitalised patients. Although Amoxicillin-clavulanate was used in a proportion of patients (11.54%), sources indicate that oral beta-lactams are generally considered inferior for empirical use due to resistance patterns, and should preferably be used in combination with an initial parenteral dose or guided by susceptibility testing. A large prospective study on complicated pyelonephritis by Buonaiuto et al. (2014) (4) indicated that single therapy was the predominant approach (76.4%) compared to combined therapy (23.6%). Therefore, the antibiotic choices observed in the current study appear to reflect a strategy of employing potent agents, likely guided by the severity of the patient population and the need to cover potential resistant pathogens in the context of complicated pyelonephritis.
The data indicate that antibiotic combination therapy was commonly utilised in this cohort, with Gentamicin combined with Meropenem being the most frequent
regimen, administered in 21.78% of recorded instances (Table 7.). Overall, 101 patients received one of the listed combination therapies, suggesting a high prevalence of this approach, which contrasts with a large study on complicated pyelonephritis by Buonaiuto et al. (2014) (4) that reported single therapy as predominant (76.4%). The observed use of combinations, particularly those incorporating Meropenem and Gentamicin, likely reflects the management of patients with complicated pyelonephritis, severe illness, or risk factors for multidrug-resistant organisms. Meropenem, a carbapenem, is highly active against ESBL-producing Enterobacteriaceae, which showed high resistance rates to commonly used antibiotics such as quinolones and cephalosporins in studies by Hase et al. (2021) (6). Gentamicin, an aminoglycoside, is another parenteral option with activity against ESBL producers. The high failure rate of empirical Ciprofloxacin therapy reported by Shafi PKM and Rosh P. (2020) (3), likely due to high resistance rates, may necessitate the use of broader or combination regimens in this patient population. Furthermore, Piperacillin-tazobactam, also frequently seen in combinations in this cohort, is noted for its good activity against many resistant strains and recommended as a potential empirical option, particularly where ESBLs are prevalent. The selection of these combinations likely reflects an approach targeting a broad spectrum of potential pathogens, especially in cases with indicators for resistant infections or increased severity (6).
FUTURE DIRECTIONS
• Addressing the threat of rising antimicrobial resistance requires continuous monitoring of local resistance patterns and identifying risk factors for infections caused by resistant organisms.
• Developing improved risk stratification models is needed to help guide decisions regarding hospital admission and the initial intensity of therapy, particularly for patients with complicated pyelonephritis.
• Further research is necessary to refine the optimal duration of antibiotic therapy for different patient subgroups.
• Testing novel antimicrobial drugs and non-antibiotic methods for treating pyelonephritis is an important area for future study.
• More research is needed to evaluate the long-term renal outcomes following acute pyelonephritis, especially in individuals with pre-existing kidney disease or those who experienced acute kidney injury.
LIMITATIONS
• Single-Center Design
The study was conducted at a single institution, which may limit the generalizability of the findings to broader populations or different healthcare settings.
• Limited Sample Size
With a sample size of 160 participants, the study may lack the statistical power to detect less common outcomes or subtle associations between variables.
• Lack of Microbiological Correlation
The absence of detailed microbiological data, such as pathogen identification and antimicrobial susceptibility patterns, limits the ability to correlate antibiotic effectiveness with specific organisms.
• Observational Nature
Being an observational study, causality between risk factors, treatments, and outcomes cannot be firmly established. Confounding variables may have influenced the observed associations.
• Variation in Treatment Protocols
The use of varied single and combination antibiotic therapies without a standardized treatment protocol may introduce heterogeneity and bias in outcome evaluation.
• Short-Term Follow-Up
The study may have focused primarily on acute outcomes, with limited data on long-term complications such as chronic kidney disease or recurrence rates.
• Incomplete Assessment of Comorbidities
Potential confounding conditions (e.g., diabetes, immunosuppression) that could influence risk and response to treatment may not have been fully accounted for.
• Reliance on Self-Reported Symptoms
Clinical symptom reporting may be subject to recall bias or subjective interpretation, affecting the accuracy of symptom prevalence data.
• No Assessment of Treatment Adherence
The study does not account for patient compliance with prescribed antibiotic regimens, which could impact treatment outcomes.
• Lack of Radiological Confirmation
If imaging studies (e.g., ultrasound, CT) were not consistently used, misclassification of pyelonephritis severity or complications may have occurred.
CONCLUSION
Our study findings provide valuable insight into the characteristics of patients presenting with this condition. The study cohort primarily consisted of adults with a mean age of 51.01 ± 18.98 years and a female predominance (58.75%). Several risk factors were frequently identified, including catheterisation (44.38%), kidney stones (39.38%), chronic urinary tract infection (34.38%), and prostate enlargement (33.13%). Management involved both single and combination antibiotic regimens, with ciprofloxacin being the most common single agent used (26.92%), while gentamicin combined with meropenem was the most frequent combination therapy administered (21.78%), suggesting approaches targeting severe illness and potential multidrug-resistant organisms. Although a majority of patients (60.00%) did not experience the specific complications assessed, sepsis (15.63%) and kidney scarring (13.13%) were the most prevalent complications observed among those who did. These results underscore the importance of considering underlying risk factors and the diverse clinical management strategies employed in pyelonephritis, particularly in complicated cases, within this hospital setting.
SUMMARY
aimed to evaluate the risk factors and management approaches used in patients diagnosed with pyelonephritis. Undertaken between November 2024 and April 2025, the research sought to analyse clinical presentations, identify key risk factors including gender, age, and comorbidities, and assess the effectiveness of current treatment strategies in a hospital setting. The study included 160 patients aged 20 years or older with a confirmed diagnosis of pyelonephritis based on laboratory reports, symptoms, and/or imaging studies, while excluding pregnant women, immunocompromised individuals, and patients with chronic kidney disease.
The study cohort comprised 160 individuals, with a mean age of 51.01 ± 18.98 years. Females represented the majority of the patient population, accounting for 94 participants (58.75%), compared to 66 males (41.25%). Various clinical symptoms were reported by the patients, with uni/bilateral loin pain being the most common, affecting 41.25% of the cohort. Other frequently noted symptoms included increased urine frequency (36.88%), pedal oedema (35.63%), haematuria (34.38%), fever
(33.75%), flank pain (33.75%), vomiting (33.75%), nausea (33.13%), dysuria
(33.13%), and burning micturition (32.50%).
Several underlying conditions were identified as prevalent risk factors among the participants. Catheterisation was the most frequently observed risk factor, present in
71 individuals (44.38%). This was followed by the presence of kidney stones in 63 patients (39.38%), a history of chronic urinary tract infection in 55 individuals (34.38%), and prostate enlargement in 53 patients (33.13%).
Regarding complications, a significant proportion of the cohort, 96 individuals (60.00%), did not experience the specific complications assessed. Among those who did, sepsis was the most commonly reported complication, affecting 25 participants (15.63%), followed by kidney scarring in 21 individuals (13.13%), kidney abscess in 12 patients (7.50%), and renal failure in 6 patients (3.75%). These findings provide insight into the spectrum and frequency of severe outcomes in this patient group.
The management of pyelonephritis in the study involved both single and combination antibiotic regimens. Among the 78 instances of single antibiotic therapy, ciprofloxacin was the most frequently administered agent, prescribed to 21 individuals (26.92%). Meropenem was used in 17 participants (21.79%), followed by piperacillin-tazobactam in 11 (14.10%), while ceftriaxone and gentamicin were each used in 10 participants (12.82%), and amoxicillin-clavulanate in 9 individuals (11.54%). For the 101 instances of combination antibiotic therapy, the combination of gentamicin and meropenem was the most frequently employed regimen, administered to 22 individuals (21.78%). Other combinations were utilised with varying frequencies, including amoxicillin-clavulanate with piperacillin-tazobactam, ceftriaxone with gentamicin, and ceftriaxone with piperacillin-tazobactam, each given to 8 participants (7.92%).
REFERENCES

Bagul Samruddhi, Deshmukh Rajeshwari, Kolekar Aniket, Suryawanshi Kirti, A Prospective Observational Study on The Risk Factors and Management of Pyelonephritis, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 7, 77-92, https://doi.org/10.5281/zenodo.21103378
 10.5281/zenodo.21103378
10.5281/zenodo.21103378