
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmaceutics, Loknete Dr. J. D. Pawar College Of Pharmacy, Kalwan Nashik, India.
Ocular drug delivery encounters major challenges. because to the rapid precorneal loss caused by tears turnover, corneal barriers, and low bioavailability (<1%) of conventional eye drops, necessitating frequent dosing for conditions like glaucoma and conjunctivitis. These limitations often result in poor therapeutic efficacy and patient non-compliance. This review aims to evaluate pH-sensitive in situ hydrogels as innovasive systems for sustained ocular drug delivery, highlighting their formulation strategies and potential to enhance bio-availability. This review centers on in-situ gel systems, including pH-triggered systems. It involves detailed method of preparation, mechanisms of gel formation and the pH-triggered system's assessment parameters. Finding the ideal medication concentration at the site of action is a significant challenge in eye therapies. A sufficient amount of the active sub-stance must be administered and kept in the eye for ophthalmic therapy to be effective. This work primarily focuses on pH-triggered in situ gelling systems that include polymers like chitosan, carbopol, and combinations with hydroxypropylmethylcellulose (HPMC). At ocu-lar pH, PH-sensitive hydrogels go through a sol-gel transition.(6.9-7.4), triggered by poly-mers like carbopol 940, which swells in neutral environments, or chitosan, which protonates for mucoadhesion and permeation enhancement. Common polymers include carbopol for pH-dependent viscosity increase. Advantages encompass sustained release up to 95% over 24 h, and reduced dosing frequency
As a sensory organ, the eye transforms light into an electric signal that the brain processes and interprets.1 One of the body's most important and sensitive organs is the eye, and administering medication to it is the most difficult undertaking since the eye has several defense mechanisms that protect it from different foreign particles2. Creating effective ways to deliver medication to the eye is difficult for scientists because the eye has a unique structure and function that makes it hard to design the right treatments.3 The main issue with applying medication to the surface of the eye is that the drug quickly disappears before it can work, mainly because it drains away through the tear ducts and the tears keep changing often. As a result, only a small portion about 10% of the medicine actually reaches the area where it needs to act4. Two ways to boost how much medicine gets into the eye are either making the cornea more permeable by using penetration enhancers or prodrugs, or by increasing the time the medicine stays in contact with the eye using viscosity-enhancing or in-situ gelling polymers5. In-situ gelling polymers experience a sol-to-gel transition when they come into contact with the physiological conditions found in the eye6. After being administered as solutions or suspensions, ocular in situ gels undergo a rapid sol-gel transition triggered by extrinsic factors such as pH changes7. These formulations also take the best parts of solutions, like longer-lasting protection for the cornea, less chance of draining into the nose, easy way to use, not causing blurry vision or stuck eyelids, accurate and consistent dosing, and the benefits of ointments8.
When these polymer-based eye products touch the surface of the eye, they change from a liquid-like state to a solid-like state through a process called sol-gel transition. 9. At room temperature (25 °C), they are liquid. Based on the physiological processes that cause them to gel, the following are the primary types of polymers: pH-induced in situ gelling polymers. When the pH changes, protons are either released or absorbed by weak acidic or basic groups in pH-sensitive polymers. This causes the polymer's structure to change shape, which in turn restricts how much it can expand or swell10 Chitosan is a type of polymer that reacts to changes in pH and remains dissolved in water until the pH reaches 6.211. The balance between the protonation and deprotonation of amino groups provides pH-sensitive properties, which enable the development of controlled release systems12. At a pH of 7.4, chitosan can turn into an eye gel. Inside the mucin structure, the positively charged amino groups and the negatively charged sialic acid parts form secondary chemical bonds like hydrogen bonds or ionic bonds13,14. When an acidic chitosan solution comes into touch with an alkaline environment, chitosan can independently form physical gels.
According to research, the degree of chitosan deacetylation affects the gelation time. High deacetylation compounds have a low density charge because they include a lot of hydrophobic groups, which makes the gelling process easier15. Since they don't use chemical cross-linking agents, physically cross-linked gels are usually well-tolerated and safe for the body. But they aren't very strong and can change how they behave when the environment around them changes, like when the temperature, acidity, or salt level changes16.
EYE ANATOMY:
The front part of the eye, which includes the cornea, conjunctiva, and iris, is one of the two main parts of the human eye. This section also contains the aqueous humor, anterior chamber, ciliary body, pupil, and crystalline lens. The other part of the eye includes the trabecular meshwork, vitreous, sclera, retina, choroid, macula, and optic nerve17. The outer part of the eye is known as the cornea. It is a thin, clear tissue that allows light to pass through. It has several layers, including the endothelium, Bowman's layer, stroma, Descemet's membrane, and epithelium. The cornea contains a clear liquid that fills the back part of the eye's front chamber18. The iris is a thin, circular muscle that covers the front part of the lens. Underneath the cornea, there is a diaphragm that changes size, which controls how big the pupil becomes. This helps control how much light gets into the eye.The dilator muscle and the iris sphincter work together to make these adjustments19. ciliary muscle is a ring of smooth muscles located in the middle layer of the eye, controls the region that can be used to view objects at various distances20. A thin layer of clear material is placed over the transparent biconvex shape that forms the lens. This structure is flexible and made up of layers of tissue that are contained within a capsule. It is kept separate from the ciliary muscles by very thin fibers known as zonules21. Starting at the edge of the cornea, the conjunctiva is a thin, mucous membrane that covers the inside of the eyelids and the sclera up to the limbus. This membrane helps protect the eyes by producing mucus that keeps them moist and prevents germs from entering. The sclera, often called the "white of the eye," is the tough, outer layer of the eye that keeps it shaped and acts as the main defense for the inner parts of the eye22.
The choroid is a part that has a lot of blood vessels and is found between the sclera and the retina, unlike the sclera itself.. The choroid is the second layer of the eye, right between the sclera and the retina. It is a dark brown, thin membrane that has a lot of blood vessels and a pigment that helps absorb extra light, which stops it from causing problems with vision23. The vitreous humor is a smaller area in front that spreads between the retina and the lens, containing a clear, thin, jelly-like fluid that is similar to water24.
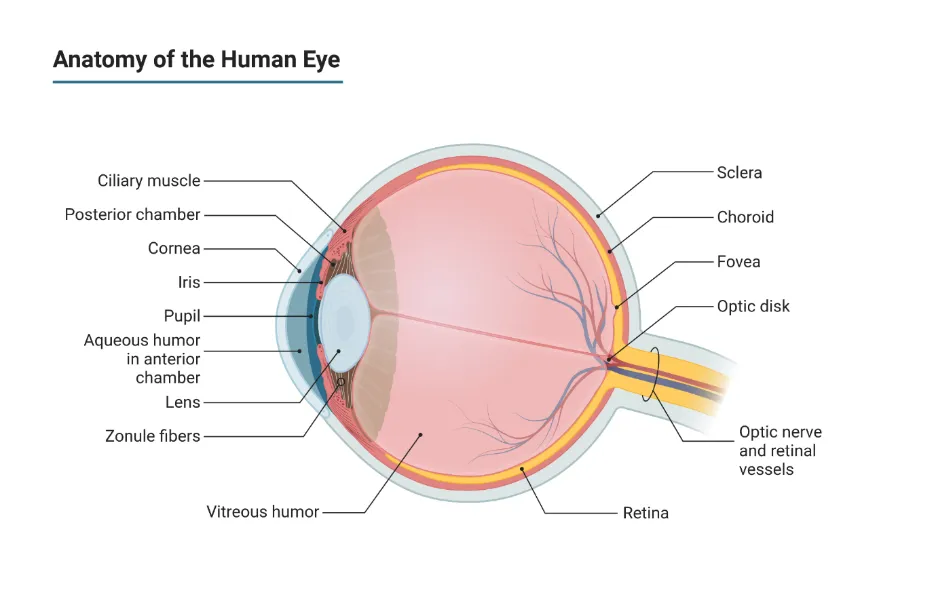
Fig : Anatomy Of Eye
BARRIER FOR OCULAR DRUG DELIVERY:
Numerous static and dynamic obstacles to ocular drug delivery significantly restrict drug bioavailability, frequently to less than 5% for topical treatments. Although these defense mechanisms preserve ocular homeostasis, Anterior and posterior segment problems are very challenging to treat26.
1 Precorneal Barriers :
Precorneal parts quickly take drugs off the surface of the eye. Blinking and draining through the nose help get rid of extra liquid (>9 microliters) in a few minutes, which shortens how long the drug stays in contact. The tear film turns over at a rate of about 1 microliter per minute. Since the mucin layer of the tear film doesn't hold onto water-loving molecules very well, blinking helps remove them27.
2.Corneal Barriers :
The main static barrier for anterior segment delivery is the cornea's multilayered structure consists of the epithelium, Bowman's layer, stroma, Descemet's membrane, and endothelium. Although lipophilic medications have a higher paracellular penetration rate, their overall bioavailability is still less than 5%28.
3. Conjunctival and Scleral Barriers:
Conjunctival non-corneal pathways prevent systemic overflow but delay local absorption due to blood flow and lymphatic clearance. Larger hydrophilic molecules can pass through the sclera, but this is blocked by fast choroidal circulation29.
4. Blood-Ocular Barriers:
Tight connections in ciliary and retinal pigment epithelia create blood-aqueous and blood-retinal barriers that restrict posterior segment access and protect intraocular homeostasis. P-glycoprotein and other efflux pumps actively eliminate substances30.
5. Posterior Segment Barriers:
Intravitreal gene treatments are blocked by the inner limiting membrane and the slow diffusion of vitreous fluid. Metabolic and vascular clearance obstacles are added by the retina and choroid31.
PH-SENSITIVE IN-SITU POLYMERIC SYSTEM CLASSIFICATION:
1. A Carbopol:
At alkaline pH, the well-known pH-sensitive polymer carbopol forms a low viscosity gel, whereas at acidic pH, it remains in solution form. HPMC is combined with using carbopol to give the carbopol solution viscosity while lowering the solution's acidity32. Water-soluble polymers like the carbopol system, hydroxy propyl methyl cellulose system, poly (methacrylic acid), and poly (ethylene glycol) are classified as pH-triggered in-situ gelling polymeric systems. This concept served as the foundation for developing and testing an ocular delivery system for indomethacin, a drug used to treat uveitis. Because an eight-hour sustained release of indo-methacin was observed in vitro, this method is an excellent choice for ocular delivery33.
Carbopol in Ocular Ph Sensitive In-Situ Gels:
1.pH-Triggered Mechanism: When the pH goes above about 5.5, the polyacrylic acid (PAA) polymer, which is carbopol, starts to form gels, although it stays liquid at acidic pH levels34.
2. Formulation Strategy: Low-concentration Carbopol is sometimes mixed with other polymers like HPMC or chitosan, which also lower the total polymer concentration required, to prevent eye irritation brought on by its high acidity.
3. Common Grades: Because of their superior gelling and viscosity properties, Carbopol 934, 940, and 981 are regularly mentioned.
4. Key Advantages: It offers significant mucoadhesion, Increasing the time the drug stays on the eye's surface and enhancing the effectiveness of the treatment35.
2. Cellulose acetate phthalate:
Cellulose Acetate Phthalate, which is also called CAP, is a type of anionic polymer that responds to changes in pH. which is derived from cellulose ester, commonly used as an enteric coating and in latex form for ocular in situ gels36,37. At an acidic pH of 4.4–4.8, CAP latex dispersion is a stable, low-viscosity liquid that is perfect for painless instillation as eye drops. It facilitates sustained drug release for anterior region targeting and is non-irritating and biocompatible38. When CAP comes into touch with tear fluid (pH ~7.4), phthalate groups deprotonate and quickly neutralize the surface charge, causing particle aggregation and coagulation into a thick gel in a matter of seconds. This increases bioavailability and decreases nasolacrimal drainage by extending the corneal residence time34. used in formulations such as timolol maleate gels at low doses (0.5-2% w/w); it forms clear, pseudoplastic gels after instillation and is stable for storage at pH 4-539.
Cellulose Acetate Phthalate in Ocular ph sensitive In-situ Hydrogels:
1.Increased Residence Time: By creating a viscous "micro-reservoir," CAP stops medicine from draining down the nasolacrimal duct quickly40.
2. Sustained Release: It reduces the need for frequent dosage by offering a regulated release of medications like Timolol Maleate and Cyclosporine A41.
3. Hydrophobic Drug Loading: Because of its structure, CAP can efficiently load and shield hydrophobic medications that would otherwise be poorly soluble in water42.
3. Chitosan :
Chitosan offers the crucial mucoadhesive and permeation-enhancing qualities that keep the formulation in contact with the cornea, while carbopol frequently acts as the main pH-responsive agent43. Chitin is the source of chitosan, a linear cationic polysaccharide. Its major amine groups determine how it responds to pH44. The polymer becomes water soluble due to the chains' electrostatic repulsion because the amine groups are protonated at acidic pH levels (less than 6.0).When the formulation comes into contact with the tear film at ocular pH 7.4, the amine groups deprotonate. A decrease in electrostatic repulsion and an increase in hydrophobic interactions and hydrogen bonding cause the polymer to undergo a sol-gel transition45.
Chitosan in Ocular ph sensitive In-situ Hydrogels:
1.pH-Triggered Gelation: At pH 7.4, Sometimes in combination with polymers like carbopol or alginate, chitosan transforms from a liquid to a thick gel.
2. Mucoadhesion: The positive charge of chitosan enhances its retention time by interacting with the negatively charged mucin on the corneal surface.
3. Permeation Enhancement: It improves transcorneal permeability, which makes it easier for therapeutic medications to be absorbed46.
Preparation technique (pH triggered Method ):
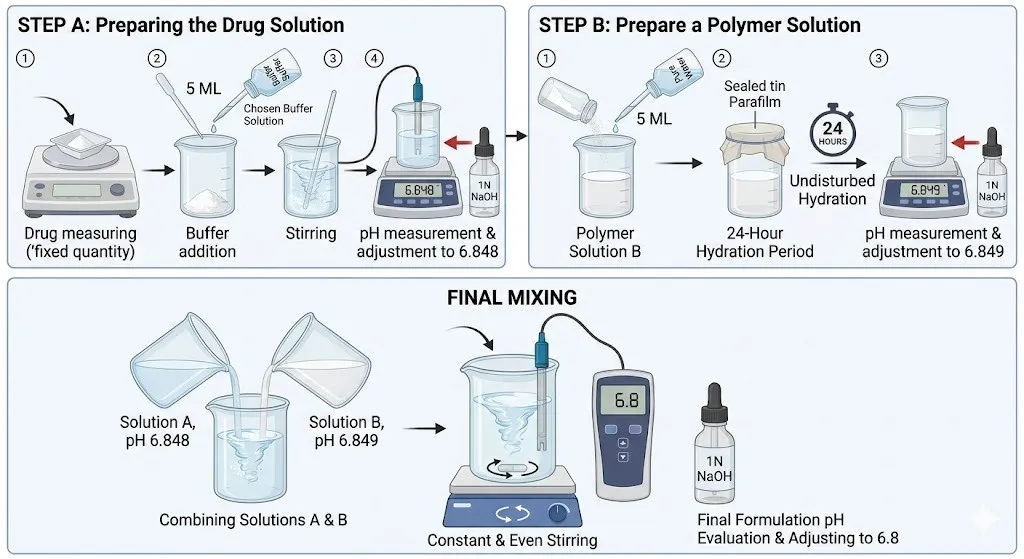
Step A: Creating the Drug Solution
Step B: Prepare a Polymer Solution
Final Mixing
EVALUATION PARAMETER:
1.Physical Appearance:
Formulations are visually examined in good light against black and white backgrounds to check for color, homogeneity, and particle matter. Solutions that are transparent, colorless to pale yellow, and free of turbidity are considered to have an excellent appearance50,51.
2. pH
The pH of the in situ gelling system will be measured using a calibrated digital pH meter. Transfer the specific volume of formulated solution into a clean beaker. Immersed the electrode in the solution at room-temperature. Once the reading has stabilized, note the value52,53.
3. Clarity Test:
The pH-sensitive in situ hydrogel's clarity assessment guarantees that the formulation is transparent and particle-free for ocular drug administration, which is essential to avoiding blurred vision after administration. Visual inspection of the solution both before and after gelling resulted on by change in pH is part of the procedure54. Place 1-2 mL of the mixture in a transparent container with a bright fluorescent light and a black and white backdrop. Inspect for turbidity, foreign particles, or opalescence with the naked eye; if compliant, formulations seem transparent and clear55.
4. Gelling ability:
A drop is placed into a vial containing 2.0 ml of freshly prepared simulated tear fluid to test how well the formula can form a gel. The time it takes for the gel to form is then noted56.
5. Viscosity:
The viscosity is mostly assessed using the Brookfield viscometer. Viscosity is a way to measure how much a solution resists flowing when force is applied. It plays a big role in how long a medicine stays in the eye. The viscosity was tested using a Brookfield viscometer after the solutions had formed a gel in the STF. The in situ gel was placed into the sampler tube. The speed of the viscometer, called angular velocity, was set between 10 and 100 revolutions per minute. The thicker the solution becomes, the higher its viscosity, especially when there's more polymer in the mix. To calculate the viscosity, two sets of data were combined, and the order of shear rates was reversed. The samples were tested at room temperature, which is 25 degrees Celsius57.
6. Test for content of drug:
One milliliter of the formulation is diluted with one hundred milliliters of distilled water to ascertain the drug concentration. After removing one milliliter, distilled water was added to dilute it to 10 ml. UV visible spectroscopy was used to measure the concentration at 200–400 nm58.
7. Drug Release Study in Vitro:
Franz diffusion cells were used to perform an in vitro drug release study of the in-situ gel solution. The receptor chamber gets fresh, prepared stimulated tear fluid, and the donor chamber gets the formulation. The dialysis membrane is placed between the donor and the receptor59. After that, the whole system is put into a magnetic stirrer that keeps the temperature steady. The temperature of the solution is kept at 37 degrees Celsius plus or minus 0.5 degrees. At set times between one and six hours, one milliliter of the sample is taken out and replaced with the same amount of fresh solution. The collected sample is then mixed with the right solvent in a 10 ml measuring flask and analyzed using a UV spectrophotometer60.
8. Sterility Test:
IP (2014) describes how the sterility test is conducted. Direct inoculation is the method used to test for sterility. Soyabean casein digest medium, artificial fluid thioglycolate, and 5ml of sterile fluid thioglycolate medium were utilized61. Each of the three prepared sets has three tubes of each medium. Sterile media served as the starting set of negative controls. Sterilized media incubated with Staphylococcus aureus served as the second set of positive controls. The test set was the third set. A 5 mL test solution was added to each medium after the 1 mL sterile ideal composition was diluted with 100 mL sterile water for injection. For the purpose of detecting bacterial and fungal contamination at 20–25, the incubation period was 14 days. The method of detection was the ocular examination of turbidity62,63.
9. Isotonicity Test:
In order to prevent cell irritation or injury, the isotonicity test for pH-sensitive in situ hydrogels makes sure the formulation matches the osmotic pressure of physiological fluids (such as tears, 290–310 mOsm/kg). It is frequently assessed by mixing the gel with red blood cells (RBCs) and observing no discernible shrinkage or swelling, much like 0.9% NaCl64. RBCs are examined under a microscope to check for structural alterations following interaction with the gel. The preparation can be considered isotonic if the RBCs retain their typical size and form after exposure. Because of cell swelling or shrinkage, a non-isotonic gel might seriously harm the eyes65.
10. Ocular Irritation Test (HET-CAM):
The Hen's Egg Test on the Chorioallantoic Membrane (HET-CAM) uses the membrane from a developing chicken egg to test for harsh chemicals or serious eye irritants. This method helps replace the use of animals in testing. The test checks if the conjunctiva becomes swollen or inflamed by looking at how the membrane is affected. It's a great model for studying eye irritation because the membrane has a well-developed network of blood vessels.66,67,68.
11 Study of Stability:
As part of the stability trial, the formulation was stored for three months. The test conditions for the stability study were room temperature and a relative humidity of 75±5%. At specified intervals of 30 days, the physical characteristics of the formulations were primarily evaluated, such as drug concentration, pH, viscosity, appearance, and clarity69,70.
REFERENCES
Pavčnik L, Prunk M, Trdan Lušin T, Roškar R. Accelerated Predictive Stability Testing: Accelerating Registration Phase and Application of Reduced Designs for Shelf-Life Determination of Parenteral Drug Product. Pharmaceutics. 2025 Jan 25;17(2):160


Abhay Jejurkar, Dr. Rajendra Surawase, A systematic review on: ocular drug delivery using ph sensitive in-situ hy-drogel, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 6, 2959-2971, https://doi.org/10.5281/zenodo.20644063
 10.5281/zenodo.20644063
10.5281/zenodo.20644063