
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
D. Y. Patil College Of Pharmacy Kadamwadi, Kolhapur
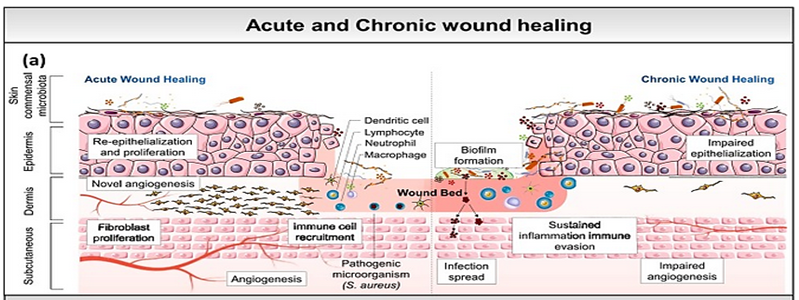
Hemostasis, inflammation, cell proliferation, and remodeling phases have been coordinated in the highly regulated biological process of wound healing. Chronic wounds—such as diabetic foot ulcers, pressure ulcers, and venous insufficiency wounds—fail to heal successfully due to prolonged inflammation, excessive protease activity, impaired angiogenesis, and disrupted extracellular matrix (ECM) remodeling, whereas acute wounds usually move through these stages in an orderly manner. Particularly among the elderly and diabetic populations, these wounds represent a significant global healthcare cost. Using a focus on diabetic wounds, this article offers a thorough explanation of the physiology of wound healing, the classification of wounds, and the factors that inhibit normal tissue repair. It critically examines many experimental wound models used to investigate acute and chronic wound healing as well as frequently used preclinical animal models, such as mice, rats, pigs, rabbits, and zebrafish. Each model's benefits and drawbacks are examined in light of their applicability to the healing of human wounds. Along newly developed advanced therapies, traditional wound management techniques such surgical tissue transplantation, negative pressure wound therapy, and oxygen-based therapies are discussed. Novel molecular and biological strategies, such as anti-scarring drugs, peptide-based treatments, biomaterials, and sophisticated wound dressings, are given particular attention. In mouse wound models, anti-MFAP5 monoclonal antibody therapy has been shown to promote wound closure, angiogenesis, collagen organization, and tensile strength. In order to better replicate human wound pathophysiology and enhance clinical results in the treatment of chronic wounds, this study highlights the need of integrative treatments and complex model systems.
Cutaneous wound healing is an essential physiological process consisting of the collaboration of many cell strains and their products(1). Attempts to restore the lesion induced by a local aggression begin very early on in the inflammatory stage. In the end, they result in repair, which consists of the substitution of specialized structures brought about by the deposition of collagen, and regeneration, which corresponds to the process of cell proliferation and posterior differentiation through preexisting cells in the tissue and/or stem cells(2) Tissue repair is a simple linear process in which the growth factors cause cell proliferation, thus leading to an integration of dynamic changes that involve soluble mediators, blood cells, the production of the extracellular matrix, and the proliferation of parenchymal cells. The skin healing process, according to Mitchel et al., illustrates the principles of repair for the majority of tissues(3).
A breakdown of the outer layer's functional and structural health at where it is damaged is commonly referred to as a wound. Trauma will start the natural process of healing a wound, which is frequently finished by the appearance of a scar. In order to preserve the skin's normal structural and functional structure, healing is therefore a vital survival process (4). Human wound healing involves a number of distinct features that depend on physiology, age, sex, illness, etc. One such illness that will lead to a number of impacts is diabetes mellitus (DM), of which diabetic wounds (DWs) are thought to be the most common and serious (5)
Process of wound healing and affecting factors: During an injury, tissues may generate tissue factors from the injured area's cells and structures to accelerate the healing process. Numerous complex and integrated dynamic processes take part in the wound healing process, which begins as an innate response to the injury. In wounds with optimal conditions, these processes may continue on a regular basis, but a number of adverse conditions can interfere with this process. Interrupted wound healing can result in high rates of morbidity and mortality, along with severe discomfort, loss of function, wound infection, and gangrene formation, all of these decrease the patient's quality of life. The overall cost of treatment will increase significantly in this case. Low protein levels, high blood sugar levels, low blood sugar, edema, malnutrition, multiple toxic agents, radiation, diabetes, uremia, systemic infections, and aging are some of the situations which alter the skin's composition and biology, affecting the normal repair cycle and delayed the healing process (6). An impairment of the layer's functional and structural integrity at the affected site is referred to as a wound. Trauma begins the biological process of wound healing, which usually concludes by the development of a scar. In order to preserve the skin's normal structural and functional integrity, healing is thus a vital survival process (7). Human wound recovery involves a variety of unique characteristics that relate to physiology, age, sex, diseases, etc. One such disease that will lead to a number of complications is diabetes mellitus (DM), of which diabetic wounds (DWs) are considered to be most prevalent and dangerous (8).
The morbidity, mortality, and quality of life of patients are all significantly affected by DWs, which are more complicated and persistent. However, there are a few chances to conduct controlled studies on the features and management of DWs. It can be challenging for doctors to observe treatments or results (9). In order to study the complexity of DW healing in settings with less biological and biological variation, researchers studied other animals at this time (10). Although there have been some significant developments in DW care enhancement, more work has to be done. In order to examine new approaches to therapy and further improvements in the current treatment approaches, it is essential to understand the pathophysiology of DW (11).
As a way to examine cellular and physiological responses in DW, a variety of experimental models have been created, primarily animal models. Since each of these DW animal models has benefits and drawbacks of its own, selecting the appropriate model is essential. Thus, it is appropriate to apply a reproducible animal model as is comparable to individuals for examining any treatment intervention before translating it into clinical application. Animal models have provided essential data to the standards of DW care, although being aware that animals are not developing DW in an approach that is similar to those that appear on humans (12).A vital procedure for an organisms survival, wound healing has been successfully conserved over evolution. In humans, any major injury usually develops in a scar, whereas certain organisms have the ability to recover after tissue damage or loss. Inflammation and the activation of certain fibroblast populations in the dermal layer are involved in the multifactorial regulation of skin fibrosis and development of scars (13). Increased vascular levels have been associated with worsening scars, due to several studies that also correlate angiogenesis to scar formation (14, 15, 16). Fibroblasts are cells that are a key component of the development of scars because they are the main cell type that accumulates new ECM (extracellular matrix) cells following damage and during the regenerative phases of the healing process (17)
Classification:-
There are various methods to categorize wounds. The duration is an essential factor when dealing with to infection repair and damage care. Accordingly, wounds can be clinically categorized into two categories: acute or chronic based on the duration one apply to heal. (18).
A acute wounds like burning and surgical scars usually recover effectively for proceeding through the normal phases of wound care, chronic injuries such as ulcers in diabetes with pressure ulcers trigger the healing process and undergo extended steps of inflammation, proliferation, or remodeling that cause tissue breakdown and prolonged healing. (19).
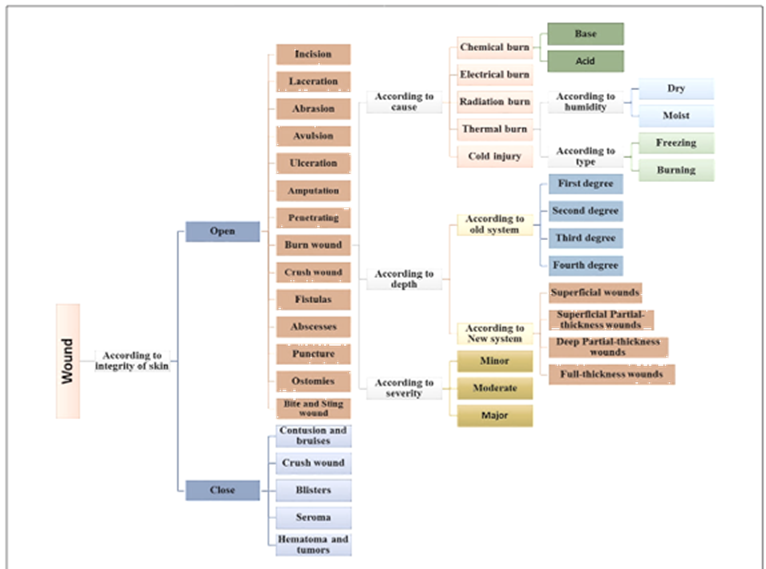
1) Acute wounds: -
Acute wounds are those that heal on their own, along a quick and orderly healing process, and lead to in both functional and anatomical restoration. Healing usually takes five to ten days or less than thirty days. Both surgical procedures and acute tissue loss can result in acute wounds (20).
2) Chronic Wound: -
Chronic wounds have to be managed effectively and systematic to ensure that they stay into the usual recovery cycles.(21).
Several of factors that prolong one or more stages in the phases of inflammation, proliferation, hemostasis, or remodelling cause the healing process to be incomplete and disrupted.These types of information indications consist of infection, tissue hypoxia, membrane necrosis, and enhanced inflammatory mediators levels.(22).
Chronic wounds may result from various causes, including naturopathic, pressure, arterial and venous insufficiency, burns and vasculitis (23)
3) Complicated Wound
Complicated Wound: A complex wound is a specific condition which involves a tissue defect and an infection (24). On the reverse hand, significant cellular tissue evacuation (such as in tumor management) or a traumatic or post-infectious cause may change the damage's site. Depending of the cause, size, location, or treatment, every wound is infected. The strength, quantity, and kind of microorganisms, the local blood supply, and the patient’s innate resistance all influence whether or not a manifest infection manifests. The five well-documented signs and symptoms of infection are redness, heat, discomfort, oedema, and loss or limited function in the affected area.The duration of infections around the wound is dependent on the method of surgery carried through and the position where the wound.(25)(26)
Process of Healing: - The physiology of the skin can be changed by wounds, specifically which impact the dermal layer. As a result of this, tissue damage can impact the anatomical structure the skin, while the extent of tissue harm is significantly affected on the process of wound healing. As the wound-healing method, some of mechanisms at the cell and molecular combine to recover the damaged area.(27).
The healing cycle is a planned chain of events that has been categorized to help us identify the dynamic processes that are closely related to healing. Different authors categorize the healing process differently; some believe that inflammation is the first step, followed by proliferation and repair in the remodeling stage (28) (29)(30)
Stages of wound healing:-
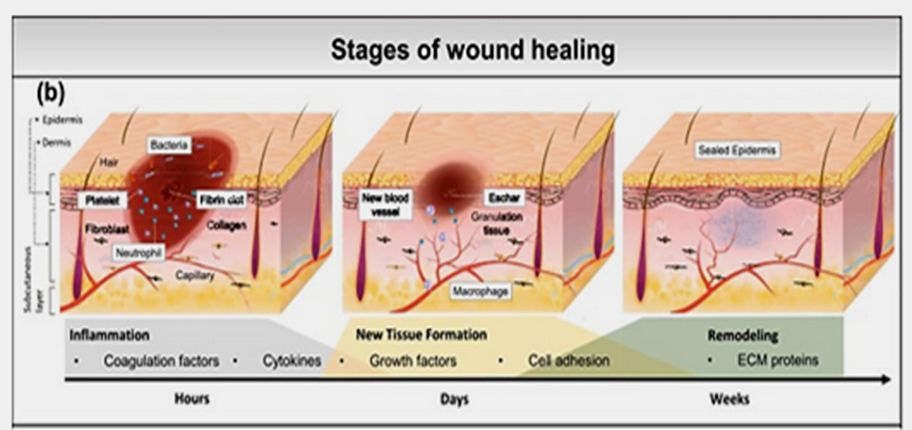
1) Inflammation :- Inflammation stimulates biological processes like vascular responses and systemic reactions meant to restore the balance of tissue homeostasis. It is a defensive response to harmful substances, such as bacteria and damaged cells created by the body. Without the inflammatory process, infections would spread uncontrollably, causing organs to undergo damaging processes that would eventually result in complete loss of function.The process of inflammation is often clinically evaluated using five traditional indications known as the "Cardinal Signals": swelling, heat, redness, pain, and loss of function. (31) (32).
When phagocytizing or generating chemicals that destroy bacteria and necrotic tissues, leukocytes act as an essential role in prevention. They can also degrade or inactivate antigens. This defines the primary objectives of the proinflammatory process. Neutrophils, monocytes, lymphocytes, and eosinophils are part of the circulating cells that enter the bloodstream, pass through the walls of blood vessels, and migrate in large numbers toward the site of aggression within the initial day during a wound.. The lymphocytes get drawn to the lesion by the significant inflammatory cytokine effects generated by platelet-stimulated blood vessel cells, and the pathogens' broken-down products. (33) (34).
2) Proliferation:- The wound closes through the period of proliferative growth. Angiogenesis, which fills the damaged tissue, is caused by the development of granulation tissue. Fibroblasts help to the creating new blood vessels that will carry nutrients and oxygen necessary for local cellular metabolism and to create a new extracellular matrix that will be used for cell proliferation. The freshly produced granulation tissue causes the temporary matrix to alter as the proliferative phase progresses. The last phase of the proliferative phase is represented by wound epithelialization (35) (36).
The extracellular matrix’s creation controls the growth, migration, and differentiation of cells inside it and serves as a substrate for cell adhesion. Structural proteins like collagen and elastin make up the extracellular matrix, whereas adhesive glycoproteins, proteoglycan, and glycosaminoglycan make up the inter cellular matrix (36)(38).
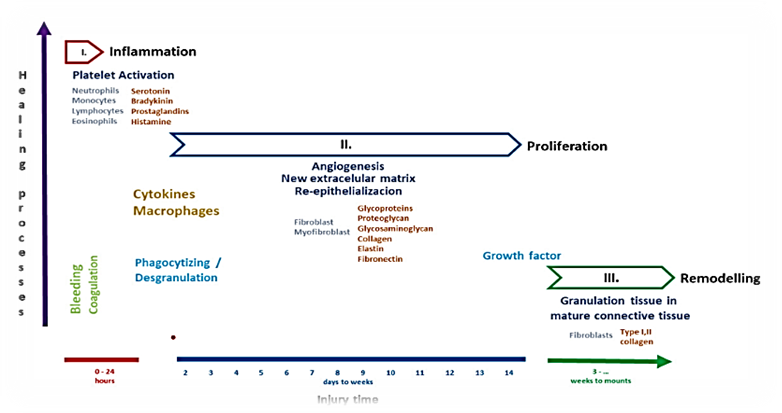
3) Remodling:- The granulation tissue remodels or matures into mature connective tissue or scar tissue during the last stage of wound healing. This stage is when the wound-healing process is most effective.Wound maturation, which is marked by a regulated reduction in collagen content and a growth in resistance to healing, starts in the third week following the injury. This process is characterized by a balance in the synthesis and breakdown of collagen fibers caused by the action of an enzyme known as collagenase. An imbalance in this interaction may promote the growth of hypertrophic and prolonged scarring. (39)(40).
The final step in the remodeling process is the appropriate deposition of the previously stated components, namely collagen fibers. The kind and distribution of collagen alter throughout this phase. Type III collagen, which is initially more prevalent in the wound than type I, is more actively broken down over time; inversely, as fibroblasts produce more collagen I, the amount of collagen decreases and tension force rises. (41)(42).
broken down over time; inversely, as fibroblasts produce more collagen I, the amount of collagen decreases and tension force rises. (41)(42).
Models and Methods: -
|
Animal Models |
Mice (43, 44, 45, 46, 47, 48, 49, 50) |
Rat (48,49,50) |
Pig (51, 52, 53, 54, 55, 56, 57, 58) |
Rabbit (59, 60, 61, 62, 63) |
Zebrafish (64, 65, 66, 67, 68, 69, 70, 71, 72) |
|
Skin Structure And Anatomy |
Thin epidermis and dermis,loose skin,presences of panniculus carmosus.
|
10–15% of human skin is formed up of the dermis and epidermis; skin that is loose.
There is a Panniculus is the carnosus. |
Identical to human dermis (30–140 µm), thick epithelium (50–120 µm) Fat tissue, tissue scars, and a completely developed dermis Thin subcutaneous region; thin hairs |
thin skin; cartilage that exists in the inner ear acts like a natural splint Huge flat areas and inadequate circulation in the inner ear |
thin epidermis; cartilage that exists in the ears acts like a natural bridge Large uniform surfaces in the inner ear that has limited circulation. |
|
Wound Healing Mechanism |
Contraction of a is the most common method of repair; wound re-epithelialization is minor. Minor growth of scars |
The contraction is the main way of recovery due to the panniculus carnosus. Healing injuries quicker than humans |
Like humans, healing mostly happens via regeneration of cells. A small contraction Similar to human formation of wounds |
Instead of causing contracting, regeneration and epithelial growth stimulate recovery. |
Increased healing of wounds without coagulation. Little scar
|
|
Biochemiacls And Molecular Features |
produces vitamin C, which is required for the development of collagen; no inflammation or hypertrophic scars are present.
|
Rapid accumulation of collagen and vitamin C development
|
Similar to human fatty acids, keratin protein content, and collagen |
Steroid and oxygen has an effect on collagen production. |
Repair is controlled by peroxide from hydrogen and strong STAT-3 and TGF-β signaling.
|
|
Research Applications |
DNA-knockout research, diabetic wounds, and serious wounds
|
Burning wounds, surgical incision models, and evacuation wound models
|
The highest standard for improving wounds in humans |
Models of ischemic wounds
|
Research on inflammation and regeneration. Molecular and genetic study Drug evaluations
|
|
Advantages |
Simple, cost-effective, accessible and complete with an extensive list of genetic information and resources. |
Cost-effective, easily accessible, and short duration (~20 days)
|
greatest similarity to human skin
|
Simple healing meditation using the opposite ear as a control Primary calculation of the wound
|
Real-time monitoring has been made likely by transparent worms. |
|
Limitations |
Heavy relaxation recovery looks to be two different from human recovery.
|
Human skin structures is similar outcome should be evaluated properly. |
Costly and needs limited facilities limited reagents targeted to pigs |
Limited relation to human skin a smaller of time used |
Skin texture changes widely the water model limited direct clinical translation |
Techniques for slowing down the healing of wounds in rats.
1) Back punch model
In the back punch model, full-thickness wounds are made on the animals’ dorsums to track wound healing. Multiple parallel wounds can be produced lateral to the spine depending on the animal's size, allowing for internal controls or duplicate measurements on the same animal (73). Contractile wound healing predominates in the absence of a splinting effect. Wounds can be collected at any point throughout the process of healing, though for histologic detection of differences between experimental and control groups, post-wounding days 3–5 are thought to be optimal (74).
2) Splinted back punch model
Splinting the incision open is advised to prevent wound healing, which is mostly aided by muscular contraction (75). In contrast to the back punch model, silicone rings are sutured past the edge of the wound. Mice require around two weeks to heal a wound with a diameter of six millimetres (75). This model’s potential flaw could be the local inflammation caused by the sutures’ anchoring (76). It is possible to collect internal controls as well as wounds of various sizes, ages, and treatments (77).
3) Head punch model
A full-thickness excisional wound is made at the top of the skull in order to build the head punch model. The underlying skull’s splinting effect causes these wounds to contract very little (78). Granulation tissue creation and re-epithelialization are the primary processes that facilitate healing.
On the level of the first wound, within 8 days. A semiocclusive dressing should be used to keep the wound from drying out. Various studies and readouts are limited by the limited size and quantity of the wounds. Information obtained from these wounds can be applied to the processes of dermal and epidermal repair (79).
4) Ear punch model
It basically consists of a thin layer of epidermis with very little subcutaneous tissue. Re-epithelialization is nearly the only process by which the wounds heal. Without a splinting device, a useful imitation of wound healing in humans is possible (79). Because the skin layer is so thin, ventral ear incisions can be made by scoring the area with a trephine and then carefully removing the epithelial tissue with a periosteal elevator (78). The animal can be prevented from manipulating the wound site by using a light bolster dressing in conjunction with a semiocclusive dressing. Usually, these wounds heal in a week (79). Demonstrated the usefulness of the mouse ear punch model for researching how radiation affects wound healing (80)
5) Tail excisional model
The wounds are produced on the proximal, hairless side of the mouse tail and removed all through to the fascia (81). Should make a 10 x 3 mm incision on the tail’s dorsal surface, 10 mm from the tail’s base. rate at which wounds heal, the presence or absence of fur, and the skin structure are the primary differences between the back punch and tail excisional models (81). In mice and rats, complete wound closure usually takes three weeks, whereas in mice, unsplinted dorsal punch wounds heal in seven to ten days (81)(82). One major drawback of the head punch and tail excisional models is their tiny maximum wound size (79).
6) Incisional wound models
In mice, they are positioned on the dorsum, parallel to the midline, and measure 10–15 mm in length. They pass through the dermis, epidermis, and subcutaneous tissue before reaching the muscle (77).
Only incisional wounds showed a statistically significant inverse relationship between planimetry and re-epithelialization. The incisional model is most useful for scarring research, but it can also be used to simulate how patients’ surgical incisions heal (83)(84). Additionally, The model able to used for researching surgical incision materials, such as the mechanical properties and degradation of various suture threads (85)(86)(87).
|
Wounds types |
Characteristics |
Benefit |
Drawback |
|
1.Full-thickness excision wound model in rodents 
|
Diabetic ulcer are clinically similar Damage to everyone of the skin's layers results in a wound.
|
Permits the pharmacological assessment of more recent compounds and formulations
|
Rodent diabetes does not fully mimic the complications associated with diabetes in humans.
|
|
2.Incision wound model in rodents 
|
Clinically, it looks like a cut into the surface
|
Checks the strength of tensile repaired skin tissue to help determine its quality. Their main application was in the research of wound scarring. |
Rodent diabetes does not fully mimic the complications associated with diabetes in humans.
|
|
3.Burn wound model in rodents 
|
Clinically associated with burn injuries from diabetes |
Due to their inexpensive cost, they are often employed in research.
|
Panniculus carnosus contraction accelerates healing.
|
|
4.Ischemic ear wound model in rabbit 
|
Clinically associated with ischemic ulcers
|
When unbroken skin is available, it is appropriate for researching type-1 pressure ulcers. Like in humans, healing happens through reepithelization. |
Genetic tractability is lacking. Does not fully replicate human hypoxia.
|
|
5.Dead space wound model in rodents 
|
Similar to the persistent inflammation found in wounds |
Because of fluid buildup, granuloma tissue and the wound environment can be studied.
|
It is unable to study reepithelization.
|
|
6.Tape striping wound model in rodents 
|
Like a human partial-thickness wound Adhesive tape is used to remove only the stratum corneum.
|
The model is easy to operate and causes the animal just mild discomfort. Makes it possible to evaluate the kind of adhesive wound dressing and reepithelization. Wound's consistency is challenging. |
Only the surface layer of the injury is affected. Because it depends on the tape's adhesiveness and the researcher's pressure, maintaining the |
|
7.Pressure ulcer model in rodents 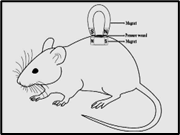
|
Clinically significant in relation to pressure ulcers A metal plate or magnet is placed beneath the wound. By repeatedly pushing the underlying plate with a magnet, pressure is produced. |
Different ulcer grades are caused by varying levels of blood circulation to the skin.
|
Human and rodent skin differ in architecture.
|
|
8.Parabiosis wound model in rodents 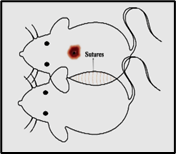
|
Similar to the common circulatory system in clinical terms. Two animal were surgically linked at the skin of their flanks. |
Helps investigate the vascular and immunological components of wound healing, which are crucial to different phases of wound healing. |
Elevated chance of death during and after surgery
|
|
9.Denervated wound model in rodents 
|
similar to diabetic neuropathy Major sensory nerve excision by surgery |
Assists in researching how diabetes-related sensory abnormalities affect wound healing |
In the end, human DW cannot reach sensationless. |
|
10.Skin fold chamber model in rodents 
|
Clinically similar to microvascular disorders The dorsal skin is sandwiched in a chamber. |
Angiogenesis and microvascular circulation pathophysiology can be investigated |
The animal experiences pain and discomfort.
|
|
11.Xenograft wound model in rodents 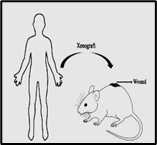
|
Resembles human wound healing with reepithelization The most human source is used, though xenografts may vary depending on the needs.
|
Beneficial for researching hypertrophic and keloid scars. |
Technically challenging and not cost-effective. It is impossible to get human-like immune responses. Has no denervation in human skin that has been transplanted. |
|
12.Infected wound model 
|
Clinically similar to DW that is infected
|
Aids in researching the host-pathogen connection along with the immune system's reaction to infections during DW healing. |
The main restriction is ethical approval.
|
|
13. Excision wound splint model 
|
Similar to human granulation and re-epithelialization, wound healing
|
Vasculature, granulation, and wound closure can all be seen, quantified, and recorded at various stages.
|
Splinting might hinder the process of healing and result in stress shielding. |
Treatments :-
1. Conventional Approaches to Wound Healing
Traditional wound management includes surgical procedures, natural therapies, and pharmaceutical treatments to accelerate skin repair. Common methods include wound drainage, skin grafts, topical antibiotics, wound dressings, and artificial skin substitutes. Surgery is effective and rapid but carries risks such as tissue damage and anesthesia-related complications. Skin grafting is widely used: Split-thickness grafts: suitable for superficial wounds involving epidermis. Full-thickness grafts: used for deep and extensive wounds; promote better regeneration with minimal fibrosis. Keratin proteins KRT16 and KRT17 play a crucial role in wound healing by supporting keratinocyte migration, proliferation, and epithelialization. Natural biomaterials like keratin-based fibers support cell attachment and tissue regeneration(88)
2. Physical Therapy for Wound Healing
Negative Pressure Wound Therapy (NPWT) enhances healing using controlled suction. It is effective for: Chronic wounds Diabetic foot ulcers (DFUs) Pressure ulcers Burns and post-surgical wounds NPWT improves blood flow, reduces infection, and accelerates tissue regeneration.
2.1 Oxygen-Based Therapies
Oxygen therapies improve healing by enhancing oxygen supply to wounds.
2.2 Hyperbaric Oxygen Therapy (HBOT)
HBOT increases oxygen levels systemically and: Promotes angiogenesis Enhances ECM production Reduces inflammation Activates growth factors (VEGF, TGF-β) Used for burns, chronic wounds, radiation injuries, and delayed healing.
2.3 Topical Hyperbaric Oxygen Therapy (THOT)
THOT delivers oxygen directly to wounds: More affordable than HBOT Fewer side effects Slower collagen synthesis and healing compared to HBOT
2.4 Continuous Diffusion Oxygen Therapy (CDOT)
CDOT provides continuous low-flow oxygen at ambient pressure: Convenient and cost-effective Used for DFUs and chronic wounds Limited clinical evidence but shows promising outcomes
3. Anti-MFAP5 Antibody Therapy
Mice were divided into three treatment groups: PBS Control IgG Anti-MFAP5 monoclonal antibody Wounds were treated topically and via subcutaneous injections on days 3, 6, 9, 12, and 15.
Healing was evaluated by: Wound area reduction Tensile strength Histology and immunofluorescence Collagen deposition (Masson’s trichrome staining) Anti-MFAP5 treatment significantly enhanced angiogenesis, collagen organization, and wound strength.(89)
4. Breakthrough Treatments for Accelerated Wound Healing
4.1 Advanced Preclinical Therapies
Innovative wound dressings aim to: Control bleeding Prevent infection Promote rapid closure
Examples include adhesive polymer-based dressings, chitosan-based materials, and inflammation-modulating therapies.
Reducing ROS and MMP-9 levels has shown improved healing in diabetic wound models.
4.2 Advanced Clinical Therapies
Several therapies are in clinical trials: OLX101 (siRNA) targeting CTGF to reduce scarring Peptide therapies (e.g., SLI-F06, Granexin) Fibromodulin (FMOD) to enhance collagen organization and tensile strength These therapies aim to accelerate healing while minimizing scar formation.
5. New Technologies in Wound Healing Research
5.1 Vascularized 3D Skin Models
3D skin equivalents with vascular networks improve in-vitro wound healing studies. Techniques include: Stem cell-embedded hydrogels VEGF stimulation 3D bio printing of skin layers
5.2 Microfluidics and Skin-on-a-Chip
Microfluidic devices replicate real skin physiology by simulating: Blood circulation Nutrient flow Drug delivery dynamics.(88,89)
CONCLUSION
The complicated and constant procedure of healing wounds can be significantly impeded by systemic illnesses like diabetes, aging, ischemia, and persistent inflammation. Chronic wounds have insufficient ECM remodeling, reduced angiogenesis, and an extended inflammatory state. Remains an important therapeutic issue.
This research emphasizes the necessity of studying the molecular and cell processes underlying wound reconstruction, along with the positive and negative aspects of present-day model organisms utilized for wound recovery studies. While mice still remain vital to fundamental research, more massive and physically suited models, such as animals with complicated biologically constructed structures, serve as vital to boost translating result.
Traditional injury therapies are frequently inadequate for intricate and prolonged injuries, although their ongoing effectiveness. Developing treatments like molecules, atomically focused therapies, and enhanced surgical coverings offer possible alternatives. In experimental experiments, MFAP5 suppression with immunoglobulin autoantibodies led in notable increases in wound healing, circulation, gelatin structure, and mechanical strength. This offers a potential pharmacological option for reducing stiffness while enhancing adaptive repair.
Future studies should concentrate on combining complex system models with targeted molecular treatments to develop personalized and successful wound care techniques. These approaches might significantly decrease morbidity, enhance quality of life, and decrease the chronic wounds' effect on the world's healthcare system.
REFERENCES






Gayatri Pujari, Tanvi Pokale, Sanika Mali, Shruti Patil, Samruddhi Patil, Dr. C. M. Jangme, An Integrated Outline of Wound Healing Diseases, Stages, and Treatment Techniques, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 3304-3320. https://doi.org/10.5281/zenodo.18715909
 10.5281/zenodo.18715909
10.5281/zenodo.18715909